). The bowel is now at risk of ischemia at the hiatal margin as the tight orifice further constricts the arterial and venous blood supply. Ultimately, if hernias are left untreated, bowel infarction (see Chapter 4) and sometimes death occur. All external hernias are at risk of this dynamic.

Figure 10-1 Coronal contrast-enhanced CT in an 85-year-old woman with an obstructed right inguinal hernia (large arrow), dilated proximal bowel (curved arrows), and collapsed distal small bowel (arrowhead).
Diaphragmatic Hernia
Diaphragmatic hernias can be congenital or develop as a result of trauma (blunt injury or iatrogenic).
Bochdalek Hernia
Bochdalek∗ hernia accounts for approximately 95% of congenital diaphragmatic hernias and is situated in a posterolateral position, mostly on the left. Sometimes the hiatus is large enough for stomach, small or large bowel, and rarely the spleen to freely enter the chest, which can cause compression of the left lung and mediastinal displacement. Many patients are asymptomatic, however, and the hernia is detected at CT performed for incidental reasons (Fig. 10-2).
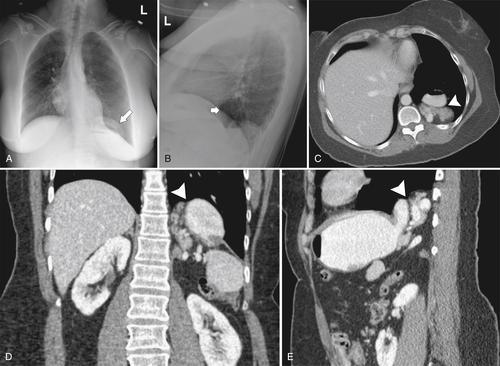
Figure 10-2 Posteroanterior (A) and lateral plain chest radiograph (B) and axial (C), coronal (D), and sagittal (E) contrast-enhanced CT in a 39-year-old woman with a Bochdalek hernia. A posterior soft tissue supradiaphragmatic density (large arrow) and gas lucency (small arrow) are identifiable on chest radiograph, and represent stomach and pancreas, identified on axial, coronal, and sagittal CT images (arrowheads).
Morgagni Hernia
Morgagni† hernia is uncommon, comprising approximately 2% of congenital diaphragmatic hernias. It is situated anteriorly and occurs when the colon and omentum (less commonly stomach, small bowel, and liver) herniate through the foramen of Morgagni, situated adjacent to the sternal xiphoid process. Most are asymptomatic, but the heart may be compressed by the herniated bowel (Fig. 10-3).
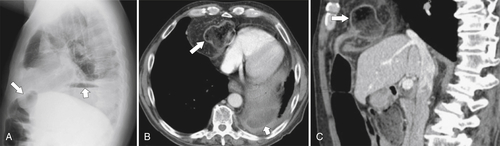
Figure 10-3 Lateral plain radiograph of the chest (A) and axial (B) and sagittal (C) contrast-enhanced CT in a 77-year-old man with a Morgagni hernia and the hepatic colonic flexure passing into the chest anteriorly (large arrows). There is also a small left subphrenic collection (small arrows).
Diaphragmatic Eventration
Diaphragmatic eventration is not actually a hernia, but rather a congenital elevation of one side of an intact diaphragm, creating a space above the normally situated diaphragm that becomes filled by the bowel. It is quite common, usually small (Fig. 10-4) but occasionally large (Fig. 10-5), and asymptomatic in most cases. In the newborn, however, it can cause respiratory distress.
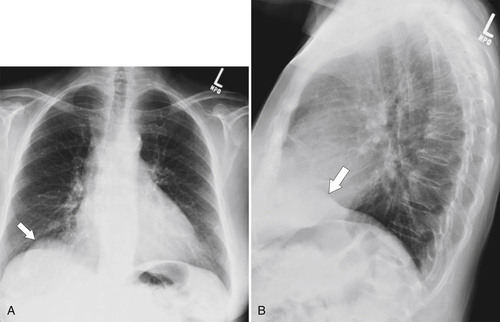
Figure 10-4 Plain posteroanterior (A) and lateral chest radiograph (B) in a 66-year-old woman with right hemidiaphragmatic elevation caused by slight eventration (arrows).
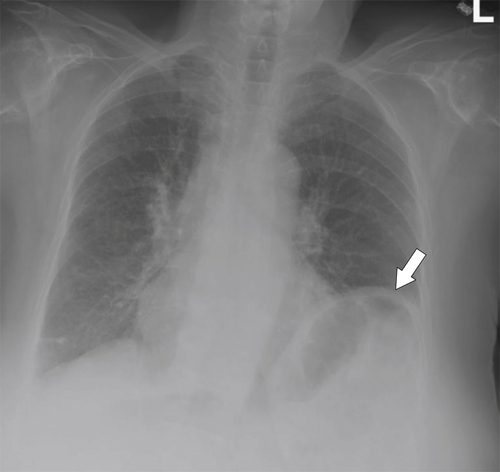
Figure 10-5 Posteroanterior chest radiograph in an 83-year-old woman with a large left diaphragmatic eventration with elevation of the splenic flexure (arrow), which remains in the abdomen.
Diaphragmatic Rupture
Diaphragmatic rupture is a tear of the diaphragm and is usually traumatic. Given that abdominal pressure is higher than chest pressure, the bowel often herniates through the diaphragmatic rent, which may sometimes be sufficient to cause symptomatic compression of the lungs or heart. The diagnosis is usually made by multiplanar CT or MRI (Figs. 10-6 and 10-7), although oral contrast material injected through a nasogastric tube should demonstrate herniated bowel contents in the chest. Most traumatic diaphragmatic hernias require surgical repair.
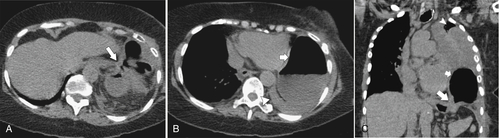
Figure 10-6 Axial (A and B) and coronal (C) noncontrast CT in a 78-year-old woman who was recently involved in a motor vehicle accident. She has left diaphragmatic rupture (large arrows) and herniation of the splenic flexure (small arrows) into the chest, causing lung compression (arrowheads).
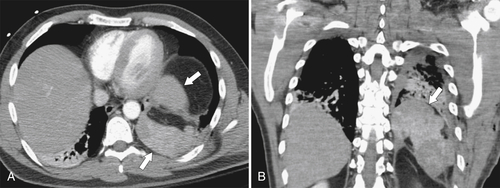
Figure 10-7 Axial (A) and coronal (B) contrast-enhanced CT in a 29-year-old man who was recently involved in a motor vehicle accident and has left diaphragmatic rupture and splenic herniation into the chest (arrows).
Pneumoperitoneum
Although pneumoperitoneum is sometimes referred to as “free air,” the gas is generally not “air,” but rather carbon dioxide inserted from laparoscopic procedures or bowel gas that is present in an extraluminal location. The gas may resemble air, however, for a short while after open laparotomy procedures. The presence of pneumoperitoneum may therefore be a benign postsurgical finding or may represent more sinister causes secondary to bowel ischemia or perforation (Box 10-1). The detection of pneumoperitoneum is important and sometimes critical because it may be the only imaging sign of bowel perforation. Its detection, however, can be challenging (especially on plain radiograph) but is more likely when the x-ray beam is tangential to the location of the gas, which rises to the most nondependent part of the abdomen. Therefore, on an upright view the gas is most likely to be identified under the diaphragm (Fig. 10-8), but on an anteroposterior view the gas may not be appreciated because the x-ray beam does not pass tangential to it. Pneumoperitoneum in the lateral or sagittal plane is better appreciated with computed tomography (CT), which demonstrates the extraluminal gas against the anterior abdominal wall (Fig. 10-9). Smaller volumes of pneumoperitoneum can be quite subtle to detect on plain radiograph (Fig. 10-10), and a lateral chest view may be required before small volumes of gas are identified (Fig. 10-11). The most sensitive plain radiograph procedure is the left decubitus (right side up) view of the right upper quadrant, where as little as 1 mL of extraluminal gas can be detected between the liver margin and diaphragm. This procedure is rarely performed, primarily because CT is a far more sensitive tool for the detection of pneumoperitoneum, especially for small volumes of gas. However, even larger volumes of extraluminal gas may be missed unless viewed using lung window contrast settings, since the gas might otherwise be confused with intraluminal gas (Fig. 10-12). Other plain radiograph findings can be demonstrated with larger volumes of gas. These include the visualization of the falciform ligament (Fig. 10-13), which is also better visualized by CT (Fig. 10-14) or recognized as a “football” sign, representing a large ovoid lucency in the center of the abdomen on supine radiographs. Gas can also sometimes be visualized in the Morison∗ pouch or may outline the lateral umbilical ligaments, but more often both sides of the bowel wall are outlined, usually referred to as the Rigler† sign (less commonly, double-wall sign). This sign is generally identified on the supine view, and large volumes of extraluminal gas are usually present (Fig. 10-15). The sign may be quite subtle or obvious (Fig. 10-16).
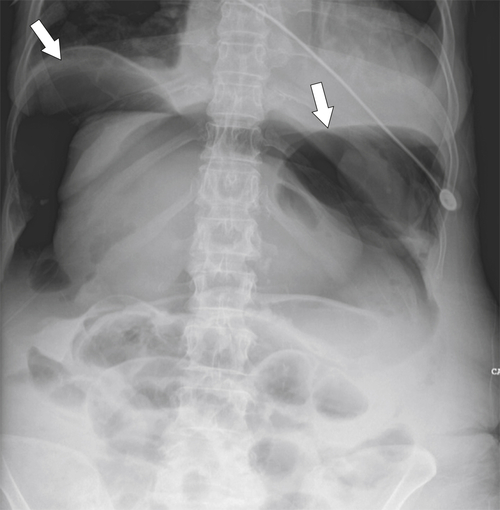
Figure 10-8 Upright plain abdominal radiograph in a 51-year-old woman who recently underwent abdominal surgery. A large pneumoperitoneum is best appreciated in the most nondependent part under the diaphragms (arrows).
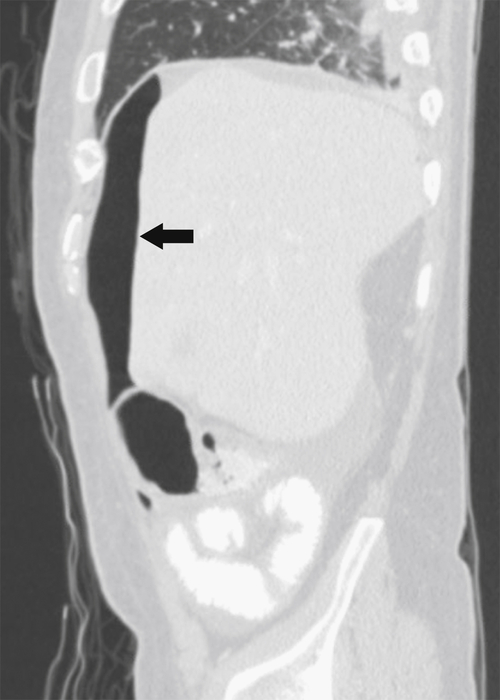
Figure 10-9 Sagittal reconstruction CT on lung window settings in a 41-year-old man with extraluminal gas against the anterior abdominal wall (arrow).
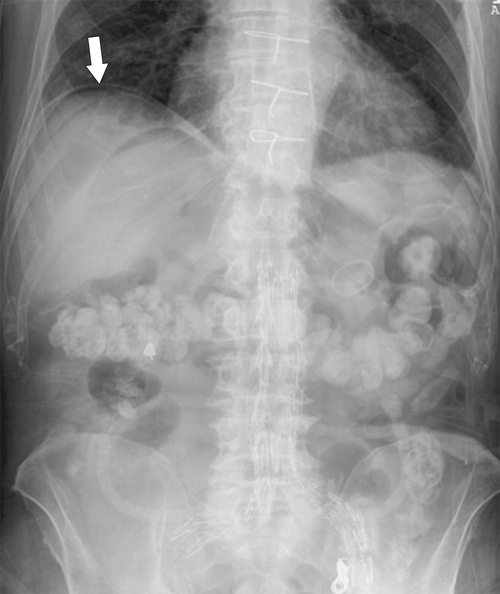
Figure 10-10 Upright abdominal radiograph in an 83-year-old man who recently underwent abdominal and chest surgery. A “sliver” of gas (arrow) under the right hemidiaphragm represents pneumoperitoneum.
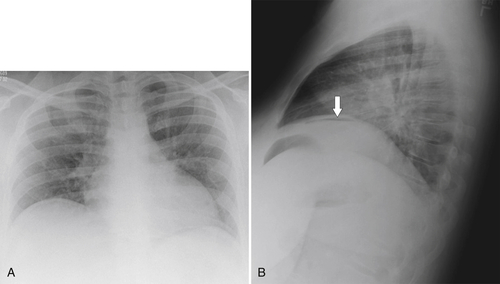
Figure 10-11 Posteroanterior (A) and lateral chest radiograph (B) in a 40-year-old woman who recently underwent abdominal surgery. Subtle pneumoperitoneum is detected only on the lateral view (arrow).
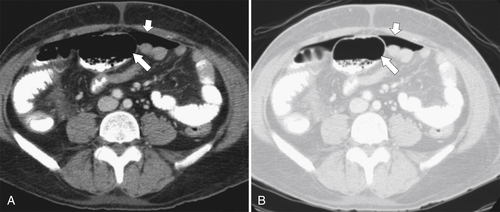
Figure 10-12 Axial contrast-enhanced CT on soft tissue (A) and lung window (B) contrast settings in a 51-year-old man. The differentiation of intraluminal (large arrows) from extraluminal (small arrows) gas is far better appreciated on lung window settings.
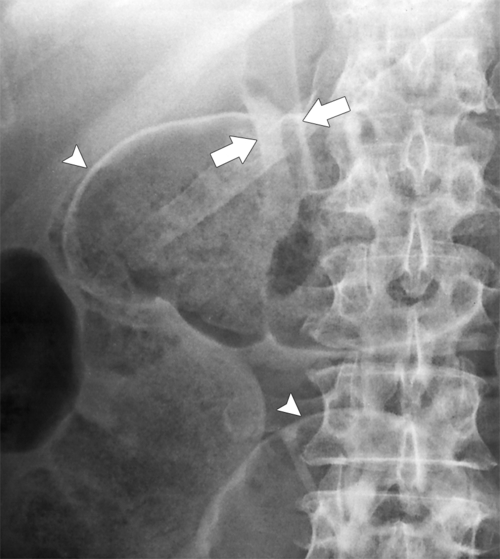
Figure 10-13 Magnified view of supine abdominal radiograph in a patient with pneumoperitoneum that outlines the falciform ligament (arrows) and a Rigler sign (arrowheads).

Figure 10-14 Coronal contrast-enhanced CT on lung windows in a 53-year-old man with pneumoperitoneum (arrow) with the falciform ligament outlined (small arrow).
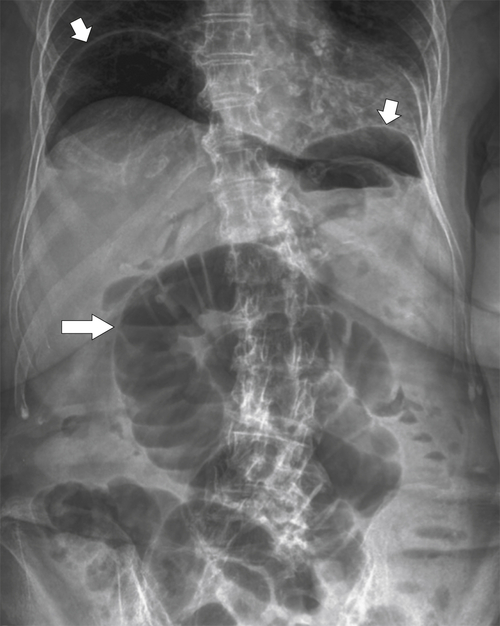
Figure 10-15 Upright abdominal radiograph in a 78-year-old woman with Rigler sign (arrow) and gas under both diaphragms (small arrows).
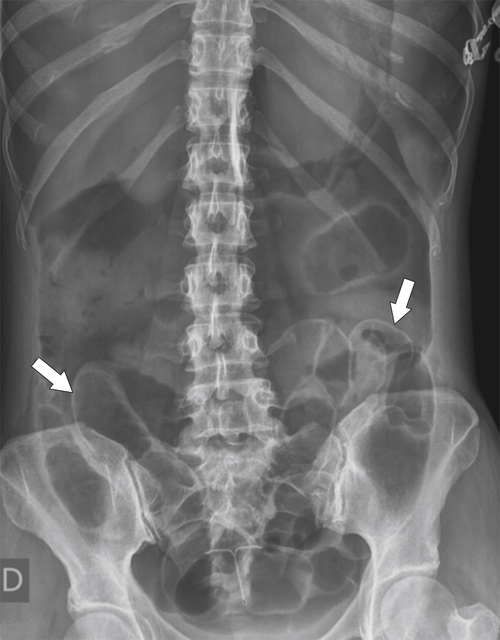
Figure 10-16 Supine plain abdominal radiograph in a 63-year-old woman with obvious Rigler sign (arrows) caused by pneumoperitoneum.
Peritoneal Disease
As a potential space, the peritoneal cavity can fill with fluid (ascites) and is susceptible to a number of inflammatory conditions. There are also a number of rare primary neoplastic lesions involving the mesentery, although metastatic deposits from intraabdominal malignancies are more common, particularly given its larger surface area.
Peritonitis
Peritonitis is an inflammatory process within the peritoneum, either infectious or otherwise but usually bacterial, which can be spontaneous or caused by rupture of an intraabdominal viscus (traumatic, inflammatory, neoplastic, or iatrogenic). Patients on peritoneal hemodialysis are particularly susceptible because they are often immunosuppressed. Tuberculosis is a common cause worldwide and is usually hematogenous in origin. Common symptoms of peritonitis are abdominal pain, fever, and sometimes distention, particularly because ileus is often associated with inflammatory disease. Most causes of peritonitis are associated with the development of ascites. Indeed, the absence of ascites normally excludes the diagnosis of peritonitis. Early in the process there may be simple ascites, which is difficult to differentiate from other causes of ascites (see later in the chapter). As the peritonitis worsens, however, the mesenteric fat becomes infiltrated and edematous (fat stranding) and the peritoneal linings become thickened and may show enhancement after the administration of IV contrast medium at CT. Peritoneal loculations, in which ascitic fluid becomes trapped within peritoneal folds and is not free to move throughout the abdomen, then develop as an inflammatory response. These can further develop into secondary loculated abscesses.
At imaging, the presence of ascites, loculated or otherwise (Fig. 10-17), can be confirmed by ultrasound (US) or contrast-enhanced CT. The features are generally nonspecific, and the diagnosis is based on clinical symptoms and signs (e.g., history of recent endoscopic procedure). Chronic peritonitis (which is sometimes recognized in patients undergoing peritoneal hemodialysis) may heal by peritoneal calcification that envelops the intraabdominal organs (Fig. 10-18). Tuberculous peritonitis often demonstrates regional adenopathy, terminal ileitis, diffuse ascites, and omental thickening (Fig. 10-19). Sometimes there is a characteristic “cocoon” appearance as the fibrotic mesenteric process encapsulates the small bowel (also known as sclerosing encapsulating peritonitis) (Fig. 10-20).
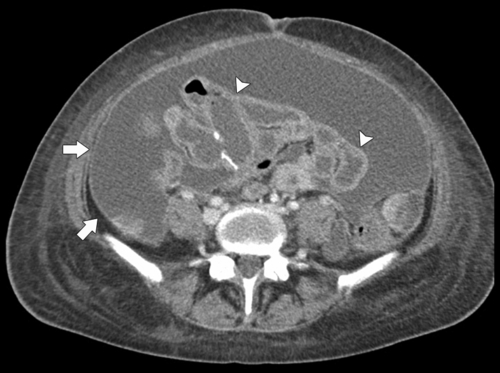
Figure 10-17 Axial contrast-enhanced CT in a 35-year-old man with tuberculous peritonitis and enhancing peritoneal lining (arrows) and a cocoon-like appearance to the small bowel (arrowheads).
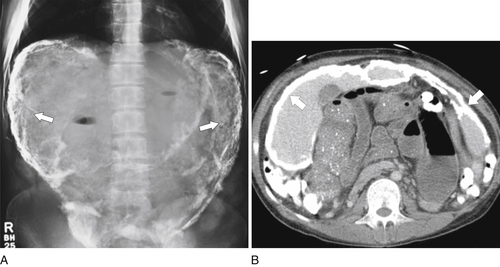
Figure 10-18 Plain abdominal radiograph (A) and axial contrast-enhanced CT (B) in a 25-year-old woman with diffuse peritoneal calcification (arrows) from multiple prior episodes of peritonitis resulting from hemodialysis.
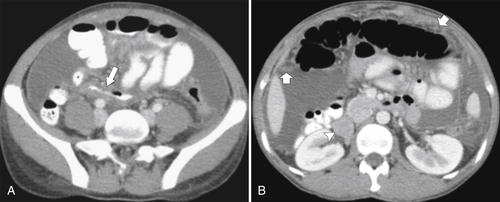
Figure 10-19 Axial contrast-enhanced CT in a 20-year-old woman with tuberculous peritonitis and diffuse ascites, terminal ileal thickening (A; arrow), and omental thickening (B; small arrows). There are also retroperitoneal nodes (arrowhead).
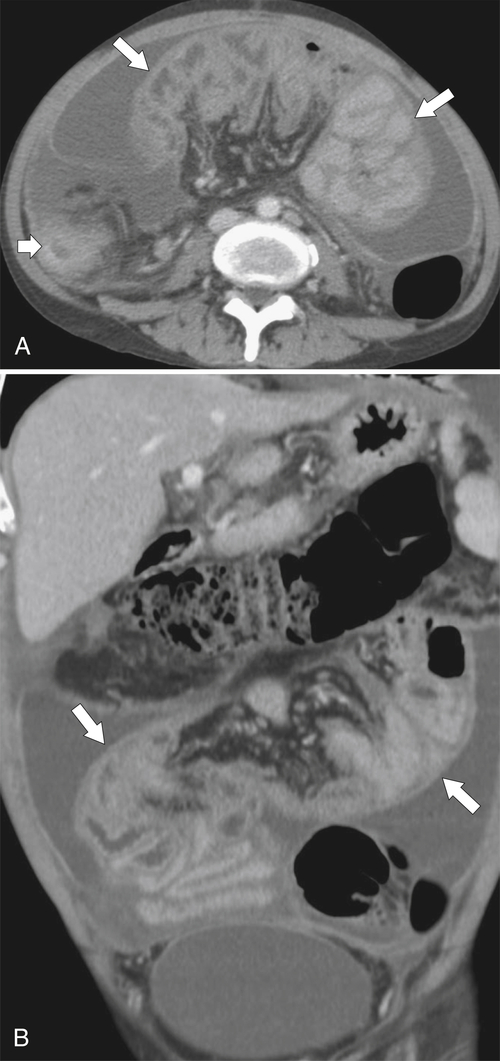
Figure 10-20 Axial (A) and coronal (B) contrast-enhanced CT in a 29-year-old man with diffuse tuberculous peritonitis with peritoneal fibrosis and confinement of the small bowel mesentery and bowel centrally (arrows) in a cocoon-like appearance. There is also colonic tuberculous disease (small arrow).
Peritoneal Abscess
Peritoneal abscess represents a peritoneal collection of pus. The abscesses may be single or multiple and are usually secondary to infection of intraabdominal organs (appendicitis, diverticulitis) or localized perforation from inflammatory bowel disease. They may result from peritonitis and often reside within peritoneal spaces (subhepatic, subdiaphragmatic, Morison pouch, or the cul-de-sac). Patients usually have abdominal pain and fever and demonstrate a peripheral leukocytosis. Imaging demonstrates a well-circumscribed, low-density collection, but definitive confirmation of abscess may require percutaneous aspiration and microbiological evaluation because infected and noninfected intraabdominal fluid can appear identical in the early stages. As the abscess develops, however, gas may form, which may be evidenced as multiple gas bubbles (Fig. 10-21) or show a fluid level (Fig. 10-22), and the lining to the abscess may enhance after administration of IV contrast material at CT (Fig. 10-23). Tumor necrosis can have similar features (Fig. 10-24).

Figure 10-21 Axial contrast-enhanced CT in a 67-year-old man with intraabdominal abscess (arrows) and multiple small gas bubbles.
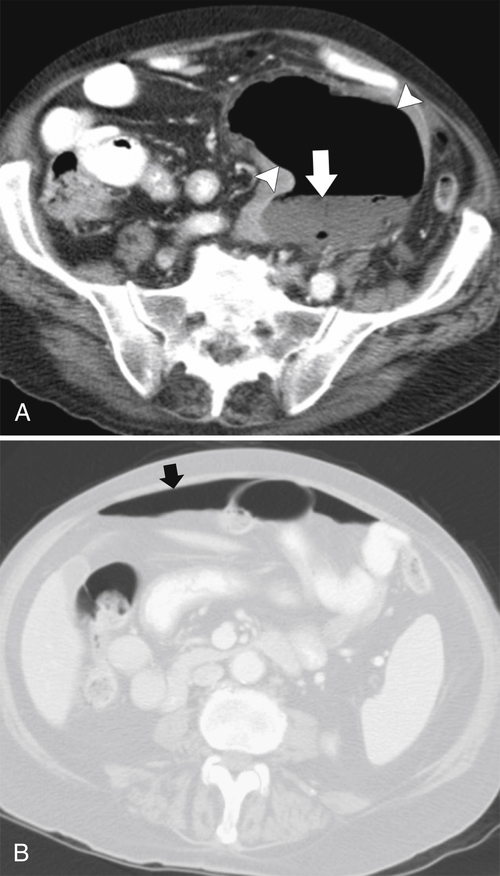
Figure 10-22 Axial contrast-enhanced CT in a 75-year-old man with colonic perforation and intraabdominal abscess (A; arrowheads) with a gas-pus fluid level (A; arrow) and anterior extraluminal gas (B; arrow) as seen on lung window settings.
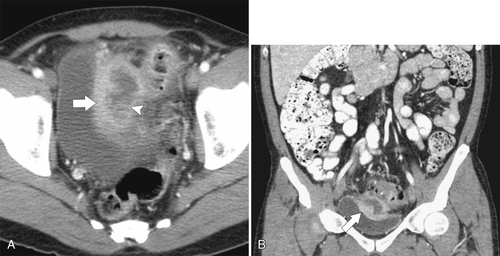
Figure 10-23 Axial (A) and coronal (B) contrast-enhanced CT in a 59-year-old man with a sigmoid diverticular abscess (arrowhead) and an enhancing wall (arrows).
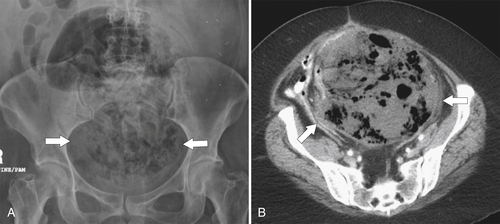
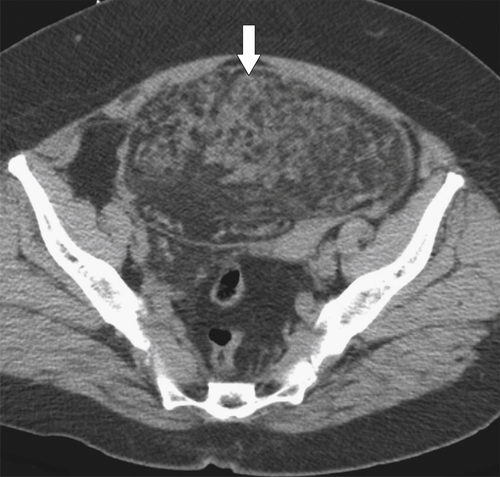
Figure 10-24 Plain abdominal radiograph (A) and axial contrast-enhanced CT (B) in a 59-year-old woman with a large necrotic pelvic sarcoma (arrows).
Mesenteritis
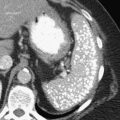
Mesenteritis is a benign process of unknown cause and is also known as fibrosing mesenteritis, sclerosing mesenteritis, retractile mesenteritis, or mesenteric panniculitis. It represents inflammation of the mesenteric fat that is identified at CT as a “hazy” mesentery produced by inflammatory change (Fig. 10-25). It often heals by fibrosis as a simple mesenteric mass (with or without associated calcification) (Fig. 10-26) or with constriction or retraction of the mesentery, often with calcification (Fig. 10-27). It should be differentiated from mesenteric metastases from carcinoid, which can have similar appearances (Fig. 10-28).
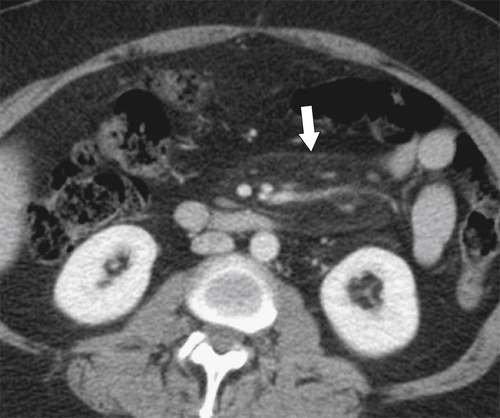
Figure 10-25 Axial contrast-enhanced CT in a 58-year-old woman with “hazy” mesentery (arrow) resulting from mesenteritis.

Figure 10-26 Axial contrast-enhanced CT in a 56-year-old woman with an irregular calcified mesenteric mass (arrow) caused by prior mesenteritis.
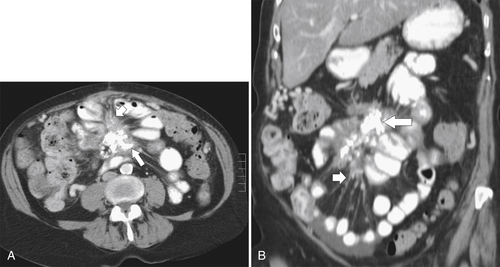
Figure 10-27 Axial (A) and coronal (B) contrast-enhanced CT in a 73-year-old woman with a calcified mesenteric mass (large arrows) with mesenteric retraction (small arrow) caused by retractile mesenteritis.
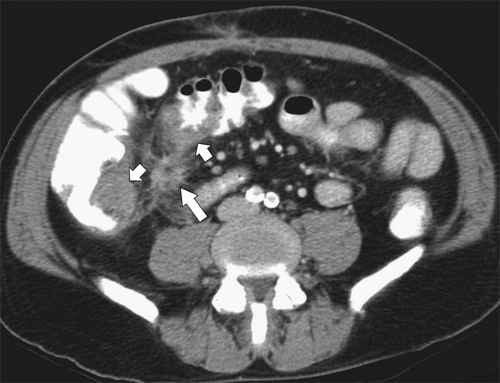
Figure 10-28 Axial contrast-enhanced CT with a right lower quadrant mass representing carcinoid (large arrow) and a mesenteric desmoplastic reaction and associated colonic thickening (small arrows).
Mesenteric Adenitis
Inflammation of the mesenteric nodes is not uncommon. It is usually nonspecific and recognized on CT as a number of slightly enlarged mesenteric lymph nodes associated with inflammatory fat changes (fat stranding) (Fig. 10-29). It is most often idiopathic but can be bacterial (Fig. 10-30) or tuberculous (Fig. 10-31). Reactive adenitis can also occur with small or large bowel infections or inflammatory bowel disease (see Chapter 4).
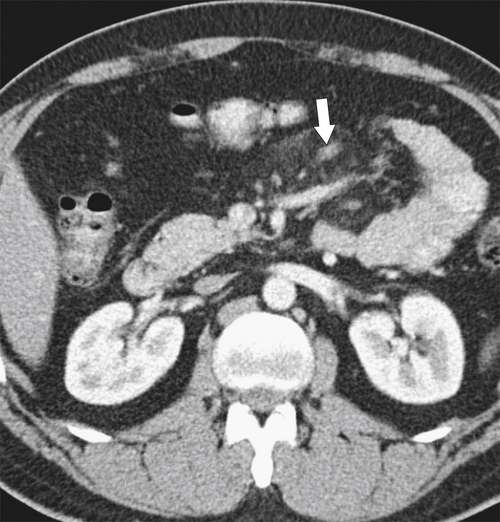
Figure 10-29 Axial contrast-enhanced CT in a 56-year-old man with several slightly enlarged mesenteric nodes (large arrow) and inflammatory fat changes resulting from mesenteric adenitis.

Figure 10-30 Axial contrast-enhanced CT in a 61-year-old man with a number of enlarged right lower quadrant mesenteric nodes (arrows) due to bacterial mesenteric adenitis.

Figure 10-31 Axial contrast-enhanced CT in a 29-year-old woman with intraabdominal tuberculosis and multiple mesenteric nodes (arrow). There are also tuberculous deposits on the liver capsule (small arrows).
Mesenteric Fat Necrosis
Mesenteric fat necrosis is often referred to as an omental infarct and simply represents arterial disruption of a small area of mesentery, leading to infarction. It is most commonly identified in obese elderly patients and in those who have had recent abdominal surgery. Patients present with acute abdominal pain, which can be mistaken for appendicitis, diverticulitis, or epiploic appendagitis. CT findings, which can be quite subtle, are a focal area of omentum or peritoneal fat with heterogeneous edematous change (Fig. 10-32). Larger areas of fat necrosis may show gas within the infarction (Fig. 10-33, A) and even fat/fluid levels (Fig. 10-33, B).

Figure 10-32 Axial contrast-enhanced CT in a 39-year-old woman with omental fat necrosis (arrow).
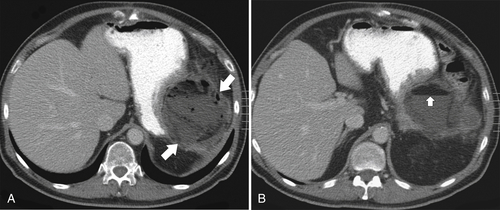
Figure 10-33 Axial contrast-enhanced CT in a 54-year-old man with left upper quadrant fat necrosis and gas formation (A; arrows). Slightly cephalad, there is a fat/fluid level (B; arrow).
Necrotizing Fasciitis
Necrotizing fasciitis is a rare, often fatal, infection of the skin and subcutaneous tissue that is caused by gram-positive and -negative bacteria, most commonly in patients with immunosuppression, diabetes mellitus, malignancy, or alcoholism. The infection is usually secondary to trauma (surgical or nonsurgical) and develops rapidly, along with widespread fat necrosis (Fig. 10-34).
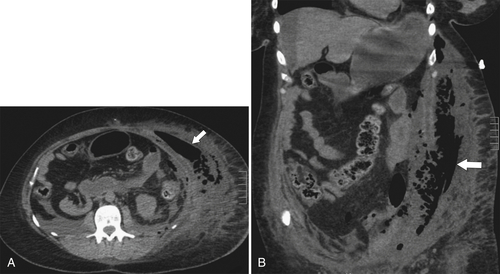
Figure 10-34 Axial (A) and coronal (B) noncontrast CT in a 44-year-old woman with necrotizing fasciitis. There is diffuse fat necrosis and gas formation in the abdominal wall (arrows).
Injection Fat Necrosis and Granuloma
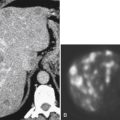
Injection fat necrosis and granuloma are commonly identified in patients who are hospitalized and have received multiple subcutaneous injections. Their features are characteristic at CT and include rounded, soft tissue changes in the subcutaneous fat because of localized fat necrosis (Fig. 10-35, A). Sometimes they show increased fluorodeoxyglucose (FDG) activity on positron emission tomography (PET) (Fig. 10-35, B). They often heal by dystrophic calcification (Fig. 10-36).
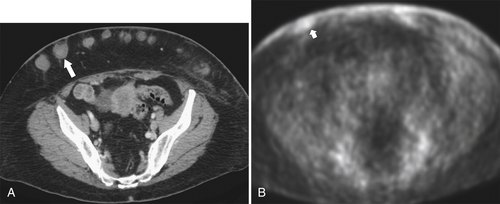
Figure 10-35 A, Axial contrast-enhanced CT in a 71-year-old woman with multiple subcutaneous soft tissue masses (large arrow) in the anterior abdominal wall caused by fat necrosis from subcutaneous injections. B, These can demonstrate mild fluorodeoxyglucose uptake at PET (small arrow) because of the inflammatory nature of the fat necrosis.
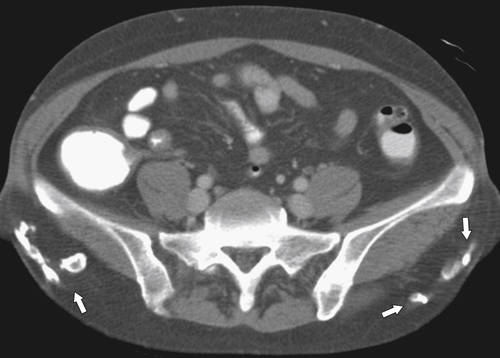
Figure 10-36 Axial contrast-enhanced CT in a 73-year-old woman with multiple calcified buttock injection granulomata (arrows).
Benign Peritoneal Masses
Peritoneal Inclusion Cyst
Peritoneal inclusion cysts represent loculated simple fluid within the abdomen, usually resulting from adhesions, and are identified primarily in an adnexal location. Therefore they must be differentiated from ovarian cysts. They are seen in women, mostly those of reproductive age, who have had prior pelvic inflammatory diseases or surgery. At imaging the cysts are usually complex with fluid and thin septa but do not typically contain solid elements (Fig. 10-37). They can become large, filling almost the entire pelvis (Fig. 10-38).
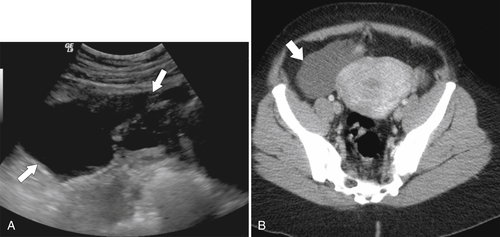
Figure 10-37 Transvaginal US (A) and axial contrast-enhanced CT (B) in a 39-year-old woman with a complex cystic lesion representing a peritoneal inclusion cyst (arrows).
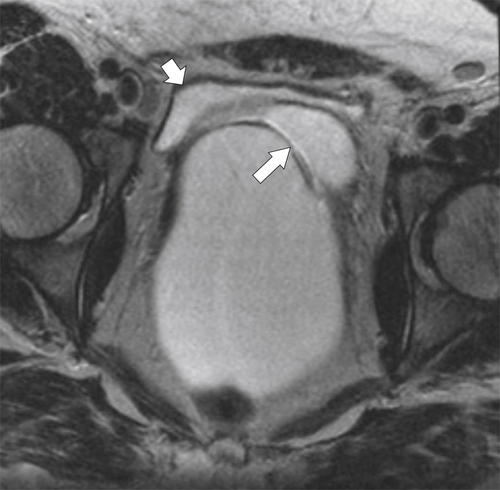
Figure 10-38 Axial T2-weighted MRI in a 37-year-old woman with a large peritoneal inclusion cyst (large arrow), distinct from the bladder (small arrow).
Lymphangioma (Mesenteric Cyst)
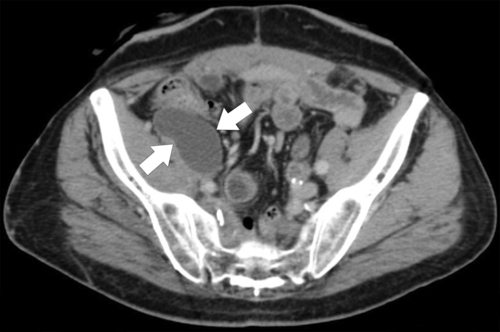
Lymphangiomas (mesenteric cysts) are cystic lesions arising within the abdomen and are usually caused by obstructed lymphatics. They are to be differentiated from mesenteric duplication cysts, which are also cystic. They are usually identified incidentally at CT as simple irregular cystic structures (Fig. 10-39) that may show punctate calcification in the cyst wall. These cysts can also occur in a retroperitoneal location (Fig. 10-40).

Figure 10-39 Axial contrast-enhanced CT in a 53-year-old man with a lower abdominal cystic mesenteric lesion (arrow) representing lymphangioma.
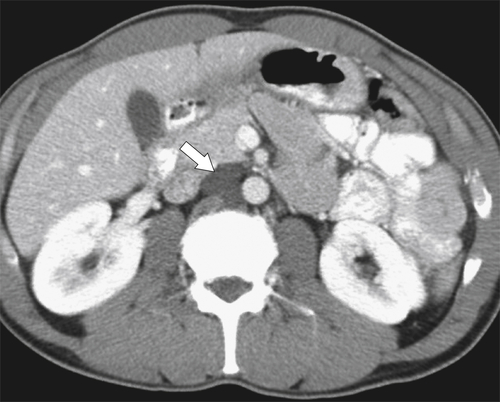
Figure 10-40 Axial contrast-enhanced CT in a 39-year-old woman with a 3-cm retroperitoneal cystic structure (arrow) representing lymphangioma.
Seroma
Seroma refers to a well-circumscribed, low-density mass representing a pocket of serous fluid that most commonly has collected as leakage from surgically damaged regional vasculature. Seromas less commonly result from trauma. Their appearances at CT are characteristic, with a well-defined smooth mass (Fig. 10-41) of uniform fluid density. The diagnosis is likely in patients with the appropriate surgical history.
Lymphangiectasia
Lymphangiectasia is a benign, usually congenital disease that is caused by dilated peritoneal lymphatics, usually idiopathic in nature but sometimes resulting from the lymphatic obstructive effects of granulomatous disease or malignancies. The lymphatic obstruction can lead to diarrhea, hypoproteinemia, and small bowel mucosal thickening (see Chapter 4). The disease is usually identified at CT as cystic structures (sometimes similar to lymphangioma) along the route of the mesentery (Fig. 10-42).
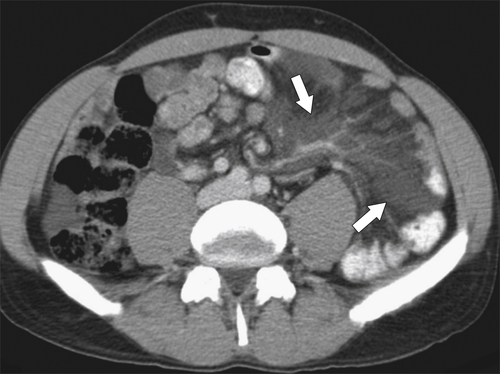
Figure 10-42 Axial contrast-enhanced CT in a 49-year-old woman with congenital lymphangiectasia (arrows).
Desmoid Tumor
Desmoid tumors are of unknown origin (although often identified in patients with prior abdominal surgery and commonly associated with Gardner syndrome, particularly when multiple), can be single or multiple, and are also known as fibromatosis. Although benign, these tumors can recur after resection and locally invade surrounding bowel. Therefore they are difficult to remove completely. They are usually located within the mesentery but can reside in the retroperitoneum or abdominal wall. Desmoid tumors are most commonly identified incidentally at CT, typically as single (sometimes multiple), nonspecific, rounded soft tissue masses within the mesentery (Fig. 10-43). They can cause displacement or retraction of bowel loops.
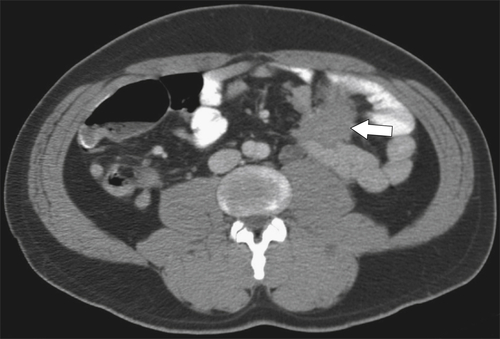
Figure 10-43 Axial contrast-enhanced CT in a 41-year-old man with a solitary soft tissue mass in the central mesentery (arrow) that represents a desmoid tumor.
Dermoid Tumor
Dermoid tumors are most commonly present in the pelvis, but larger lesions can extend into the abdomen and are ovarian in origin. They are also known as dermoid cysts or cystic teratomas and represent a primitive tumor that contains multiple tissue elements, including fat, teeth, hair, and cartilage, among other tissues. Almost all of these tumors are benign, although a malignant teratoma is recognized. They are readily identifiable at CT by their fat content (Fig. 10-44) (and sometimes other soft tissue or calcified features) and at US by diffuse hyperechogenicity resulting from the fat content. Rarely, multiple well-circumscribed fatty dermoid masses can be identified throughout the abdomen after traumatic rupture of the pelvic neoplasm, which disseminates throughout the peritoneum. At ultrasound, dermoid tumors are thought to appear similar to falling snow or a snowstorm (Fig. 10-45), but they might also be identified by other calcified or soft tissue elements.

Figure 10-44 Axial contrast-enhanced CT in a 41-year-old woman with a predominantly fatty mass due to a dermoid tumor (large arrow). There is also dense internal calcification (small arrow).
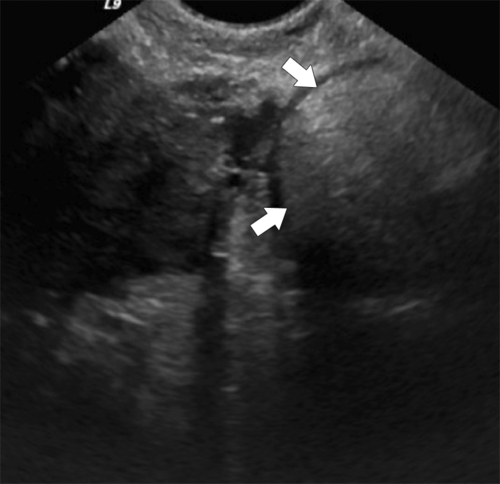
Figure 10-45 Transvaginal US in a 33-year-old woman with a left adnexal dermoid tumor (arrows) and a diffuse hyperechogenicity caused by its fat content.
Malignant Peritoneal Masses
Metastases
Metastatic deposits are by far the most common malignant peritoneal mesenteric masses or retroperitoneal deposits. They arise by direct invasion or ascitic spread (Figs. 10-46 and 10-47) or via hematogenous or lymphatic routes. The deposits can be either single and focal (Fig. 10-48) or diffuse. Diffuse involvement can invade the omentum, causing it to be studded with tumor deposits (known as omental “caking”), an appearance that can be subtle (Fig. 10-49) or obvious (Fig. 10-50). This should be differentiated from the omental caking resulting from diffuse tuberculous abdominal disease (Fig. 10-51).
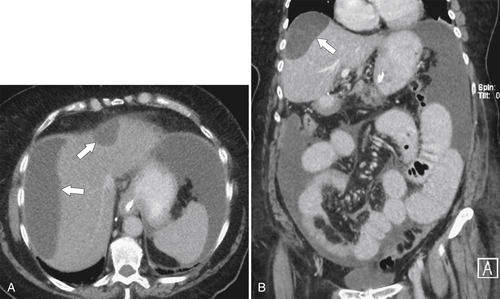
Figure 10-46 Axial (A) and coronal (B) contrast-enhanced CT in a 61-year-old woman with metastatic ovarian cancer that characteristically “scallops” the liver capsule (arrows). There is widespread malignant ascites.

Figure 10-47 Axial contrast-enhanced CT in an 83-year-old woman with diffuse peritoneal ascites and crowding of small bowel caused by metastatic ovarian cancer.

Figure 10-48 Axial contrast-enhanced CT in a 64-year-old woman with a soft tissue metastatic deposit (arrow) in Morison pouch from ovarian cancer.

Figure 10-49 Axial contrast-enhanced CT in a 56-year-old man with several omental nodules (arrow) representing gastric cancer metastases.
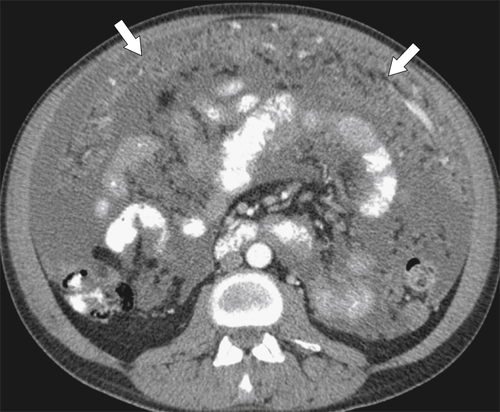
Figure 10-50 Axial contrast-enhanced CT in a 48-year-old woman with diffuse omental “caking” (arrows) and ascites caused by metastatic gastric cancer.
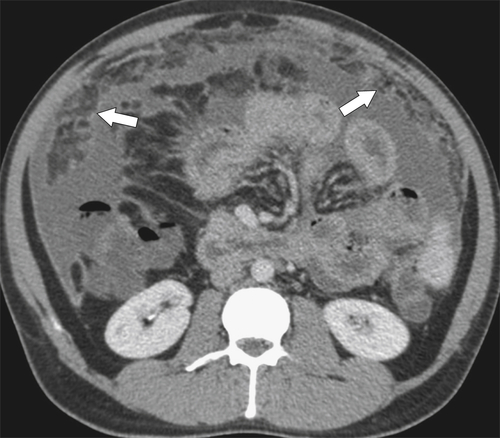
Figure 10-51 Axial contrast-enhanced CT in a 33-year-old woman with omental thickening (arrows) and ascites caused by abdominal tuberculosis.
Abdominal Mesothelioma
Abdominal mesothelioma is a rare primary malignancy of the peritoneum and is a similar tumor to the more common pleural mesothelioma. It is associated with prior asbestos exposure. In fact, up to 50% of patients show calcified pleural plaques. The diagnosis is therefore suggested in patients with peritoneal or omental thickening and calcified pleural plaques. The findings at CT vary, from ascites and fine reticular-like peritoneal changes (Fig. 10-52) to more mass-like deposits (Fig. 10-53).
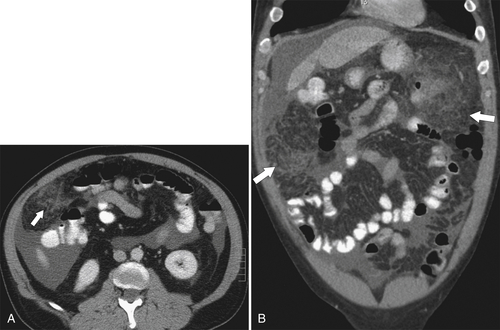
Figure 10-52 Axial (A) and coronal (B) contrast-enhanced CT in a 50-year-old man with ascites and mesenteric and omental reticular thickening (arrows) caused by abdominal mesothelioma.
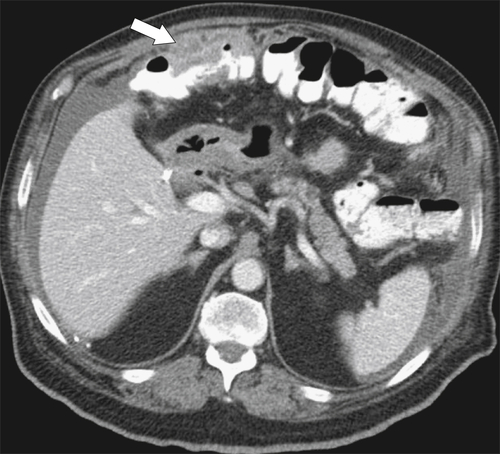
Figure 10-53 Axial contrast-enhanced CT in a 65-year-old man with ascites and omental mass (arrow) caused by abdominal mesothelioma.
Pseudomyxoma Peritonei
Pseudomyxoma peritonei is caused by the widespread peritoneal deposition of mucinous material usually from a ruptured appendix. Other mucin-producing tumors, including those of the colon and rectum among others, can also metastasize to produce pseudomyxoma. It produces multiple low-density globular masses throughout the abdomen and can envelop the small bowel, causing multiple areas of stricturing. It surrounds the liver capsule and, like ovarian metastatic disease, causes a scalloped appearance of the liver capsule (Fig. 10-54). Pseudomyxoma peritonei is difficult to treat because it is usually impossible to remove all the intraabdominal mucinous material, which therefore frequently recurs. Most patients ultimately die of the relentless mucinous process.
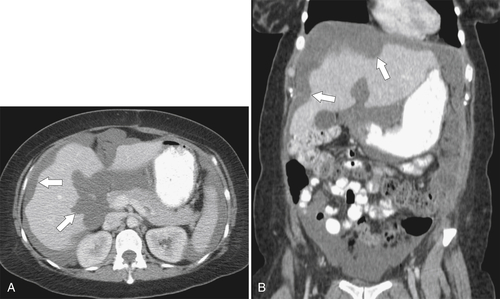
Figure 10-54 Axial (A) and coronal (B) contrast-enhanced CT in a 38-year-old woman with pseudomyxoma peritonei, scalloping of the liver margin (arrows), and diffuse intraabdominal mucinous deposits.
Liposarcoma
Liposarcoma is a malignant tumor of adipose tissue in the retroperitoneum or peritoneum (it can also occur elsewhere, such as the thigh). These are usually large bulky tumors with mass effect. On CT they can be quite subtle (Fig. 10-55) or may be recognized only by their mass effect (Fig. 10-56). Most masses are more obvious and multilobulated and predominantly fatty with few soft tissue elements (Fig. 10-57), although occasionally there is a larger soft tissue component (Fig. 10-58). These tumors require differentiation from uterine lipoleiomyoma, a benign fatty fibroid identified rarely in postmenopausal women (Fig. 10-59).

Figure 10-55 Axial contrast-enhanced CT in a 53-year-old man with a subtle fatty mass (arrow) in the left pelvis resulting from liposarcoma. Fat necrosis could have similar appearances.

Figure 10-56 Axial contrast-enhanced CT in a 49-year-old man with a right retroperitoneal fatty mass (arrows) that has mass effect on the colon and small bowel and is caused by a liposarcoma.
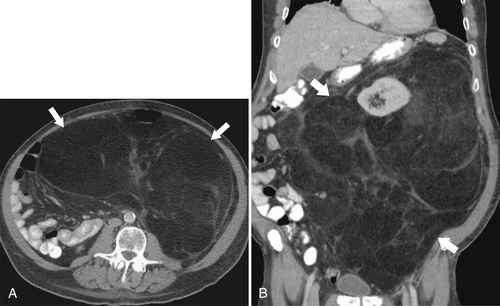
Figure 10-57 Axial (A) and coronal (B) contrast-enhanced CT in an 83-year-old man with a large multilobulated peritoneal fatty mass (arrows) with minor soft tissue components, caused by liposarcoma.
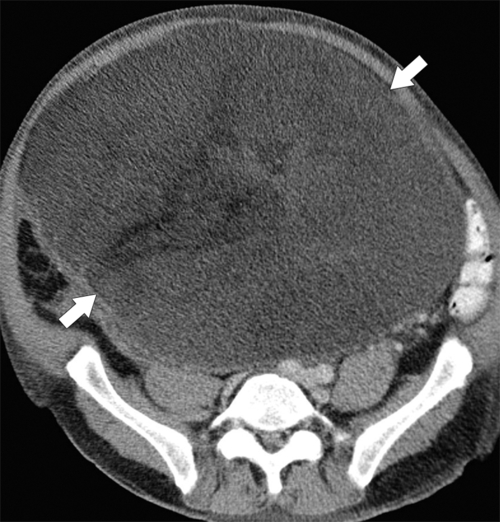
Figure 10-58 Axial contrast-enhanced CT in a 75-year-old woman with a large mixed fatty/soft tissue abdominal mass caused by liposarcoma (arrows).
Lymphoma (see Chapters 2 and 4)
Multiple enlarged mesenteric lymph nodes are most likely caused by intraabdominal lymphoma, especially if associated with retroperitoneal adenopathy. There are numerous subtypes of lymphoma, discussed in greater detail in Chapter 2. The disease is usually evaluated by CT, which readily demonstrates intraabdominal lymphadenopathy as discrete nodes (Fig. 10-60) or a conglomerate mesenteric or retroperitoneal mass (Fig. 10-61). After chemotherapy there is often a dramatic response with almost complete resolution of the lymphoid masses, but subtle residual disease that resembles mesenteric panniculitis frequently remains (Fig. 10-60). However, there is usually no residual tumor within the mass. The disease is frequently monitored with PET/CT and may show response to chemotherapy earlier on the PET than the CT study (Figs. 10-61 and 10-62).
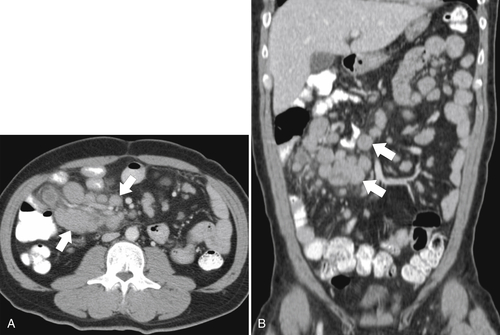
Figure 10-60 Axial (A) and coronal (B) contrast-enhanced CT in a 40-year-old man with intraabdominal lymphadenopathy (arrows) caused by lymphoma.
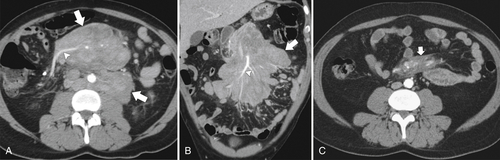
Figure 10-61 Axial (A) and coronal (B) contrast-enhanced CT in a 52-year-old man with bulky abdominal lymphadenopathy (large arrows) caused by lymphoma. After chemotherapy, on contrast-enhanced CT (C) there is almost complete disappearance of the disease, with residual hazy fat changes (small arrow). This is most likely a metabolic response with no active residual tumor. Note that vascular integrity is preserved as is characteristic with lymphoma (arrowheads).
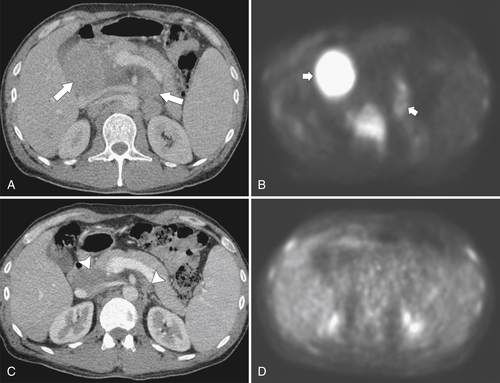
Figure 10-62 Axial contrast-enhanced PET/CT in a 40-year-old man with follicular lymphoma with abdominal lymphadenopathy (A; arrows), which are fluorodeoxyglucose avid (B; small arrows). After chemotherapy, there is still residual, but less, disease seen on CT (C; arrowheads) but complete response seen on PET (D).
Retroperitoneal Lymphadenopathy
Small (<1 cm in short axis) lymph nodes are often present in the retroperitoneum and mesentery. Although usually clinically insignificant, they are also a common site for neoplastic and nonneoplastic disease. Neoplastic disease is often secondary to lymphoma, but many intraabdominal and extraabdominal malignancies metastasize to the retroperitoneum, either as discrete, sometimes single nodes (Fig. 10-63) or as multiple and sometimes less-defined nodes (Fig. 10-64). Many infectious (e.g., tuberculosis, appendicitis, cholecystitis), autoimmune (rheumatoid arthritis), and systemic (e.g., sarcoidosis, systemic lupus erythematosus, amyloidosis, mastocytosis) diseases can also cause retroperitoneal lymphadenopathy, but these are often part of a wider spectrum of lymphadenopathy elsewhere. Lymphadenopathy caused by tuberculosis or Mycobacterium avium-intracellulare infection (often seen in acquired immune deficiency syndrome) is characteristically hypodense (Fig. 10-65).

Figure 10-63 Axial contrast-enhanced CT in a 56-year-old woman with colon cancer and a single discrete retroperitoneal 2.3-cm lymph node (arrow).
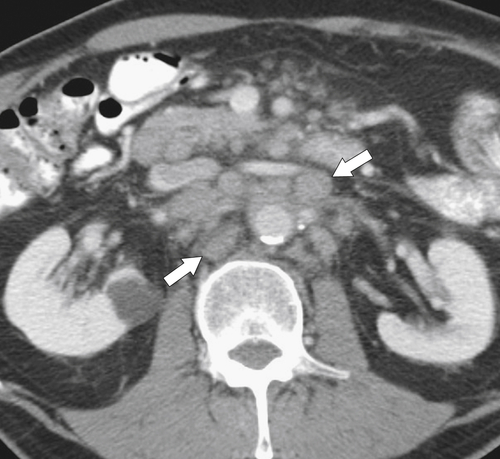
Figure 10-64 Axial contrast-enhanced CT in a 66-year-old woman with colon cancer and multiple ill-defined retroperitoneal nodes (arrows).

Figure 10-65 Axial contrast-enhanced CT in a 23-year-old woman with tuberculosis and multiple hypodense retroperitoneal lymph nodes (arrows).
Retroperitoneal Fibrosis
Retroperitoneal fibrosis is a fibrotic disease of the retroperitoneum, usually the lower retroperitoneum. The cause is most commonly idiopathic but can also be autoimmune disease (ankylosing spondylitis, systemic lupus erythematosus, scleroderma), inflammatory periaortitis (secondary to aortic aneurysms), some malignancies (lymphoma, sarcoma, carcinoma), and drug therapy (beta-blockers, methyldopa). Depending on the cause, patients respond well to immunosuppressive therapy. Patients present with nonspecific back pain or peripheral edema caused by venous compressive effects; deep venous thrombosis is therefore a complication. On imaging, a soft tissue mass envelops the lower aorta and inferior vena cava (Fig. 10-66) and may also involve the ureters, resulting in hydronephrosis. Because of its inflammatory nature, retroperitoneal fibrosis in the acute phase may demonstrate intense uptake at FDG-PET (Fig. 10-66). Diffuse retroperitoneal lymphadenopathy from lymphoma can appear similar and may also demonstrate increased uptake on PET imaging, but the retroperitoneum is often not the only site of disease and therefore it can be differentiated from retroperitoneal fibrosis (Fig. 10-67).
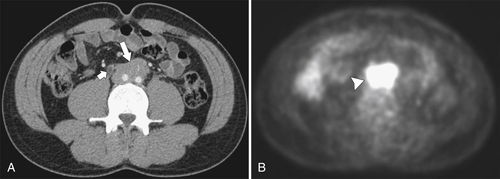
Figure 10-66 A, Axial contrast-enhanced CT in a 44-year-old woman with idiopathic retroperitoneal fibrosis and a soft tissue mass that envelops the aortic bifurcation and inferior vena cava (large arrow). There is right ureter dilatation (small arrow) caused by inflammatory involvement more caudally. B, The disease is fluorodeoxyglucose avid at PET (arrowhead).
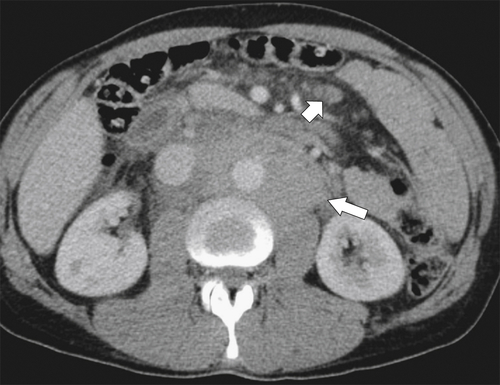
Figure 10-67 Axial contrast-enhanced CT in a 44-year-old woman with retroperitoneal lymphoma (large arrow) with appearances similar to retroperitoneal fibrosis. There are, however, smaller nodes in the mesentery (small arrow).
Extramedullary Hematopoiesis
Extramedullary hematopoiesis refers to ectopic hematopoiesis outside the bony medulla. It is therefore associated with conditions causing bone marrow displacement, particularly myelofibrosis but also congenital hemolytic anemias and thalassemia. Patients are usually asymptomatic, but mediastinal, retroperitoneal, or pelvic sites of hematopoiesis can develop and can be mistaken for lymphadenopathy or other malignant masses (Fig. 10-68).
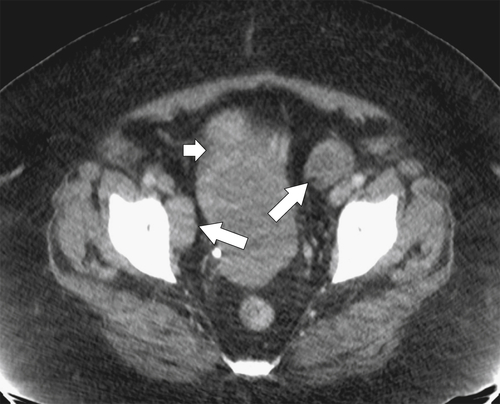
Figure 10-68 Axial contrast-enhanced CT in a 48-year-old woman with extramedullary hematopoiesis in the pelvis (large arrows). There is a fibroid uterus (small arrow).
Abdominal Wall Hemorrhage
Hemorrhage in the abdominal wall musculature is a relatively common event in patients receiving anticoagulant therapy. However, it may be traumatic (blunt injury or surgery) or caused by excessive coughing or sometimes pregnancy. At imaging, the diagnosis is usually straightforward with a hyperdense mass in the affected musculature (Fig. 10-69), which may demonstrate a hematocrit level (Fig. 10-70).
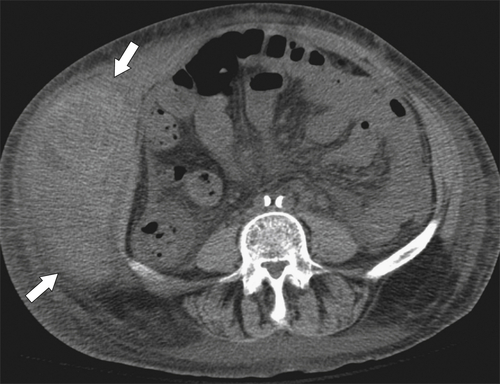
Figure 10-69 Axial noncontrast CT in a 71-year-old woman with a right-sided hyperdense mass representing an external oblique muscle hematoma (arrows).

Figure 10-70 Axial contrast-enhanced CT in a 68-year-old woman with a left-sided rectus sheath hematoma (arrowhead) that demonstrates a hematocrit level (arrow).
Propylene (Prolene) Plug
Propylene (Prolene) plug is a nonabsorbable material that is used to “fill” the hernial orifice and thus prevent hernial recurrence. Its appearance at CT imaging should be recognized (Fig. 10-71) and not confused with other, more sinister soft tissue masses. It is usually identified based on the appropriate history and expected location of the plug.
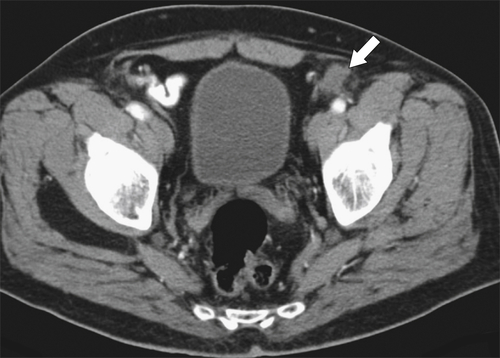
Figure 10-71 Axial contrast-enhanced CT in a 51-year-old man with a left-sided propylene (Prolene) plug (arrow) used in prior left hernia repair.
AlloDerm Spacers
AlloDerm spacers are a patented human tissue matrix (acellular human dermis) increasingly used in patients undergoing radiation or proton beam therapy. The cadaveric human tissue separates vital normal anatomical strictures from the radiation portal. AlloDerm has also been used for graft repair, breast reconstructive surgery, and hernia repairs. Its appearances are characteristic at CT with a multilayered, sometimes whorled appearance of the dermal collagen matrix (Fig. 10-72). The spacer involutes after a period of time and can be mistaken for a soft tissue mass and possible metastatic deposit, particularly because many patients are being treated for an underlying malignancy (Fig. 10-72).
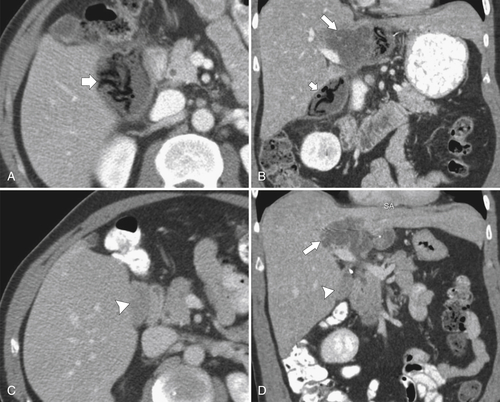
Figure 10-72 Axial (A and C) and coronal (B and D) contrast-enhanced CT in a 53-year-old man with cholangiocarcinoma (large arrows) and AlloDerm spacers (small arrows). Recent placement demonstrates serpiginous formation but later appears as a soft tissue density, mimicking a mass and recurrent disease (arrowheads).
Gossypiboma
Gossypiboma refers to retained intraabdominal surgical material that is accidently left within the abdominal cavity. The name gossypiboma is derived from the Latin word for cotton (gossypium) and usually refers to retained surgical sponge material. Gossypibomas are thought to occur in only approximately 1 in 5000 surgeries. Patients usually present with a sign and symptom of abscess formation (Fig. 10-73). If uninfected, patients present with adhesions and a foreign body granuloma.
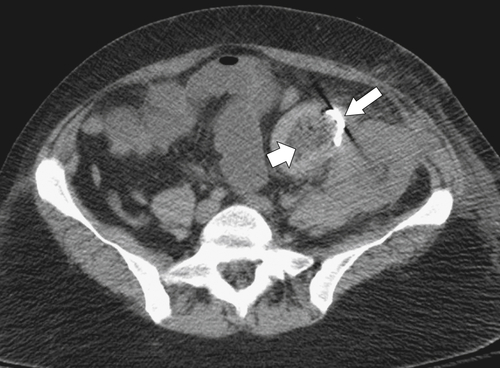
Figure 10-73 Axial contrast-enhanced CT in a 22-year-old woman with a curvilineal density (large arrow) in the pelvis and associated abscess (small arrow) caused by a gossypiboma from a retained surgical sponge.
Suggested Readings
Abdominal wall hernias: imaging features, complications, and diagnostic pitfalls at multi-detector row CT. Radiographics 2005;25(6):1501–1520.
The accuracy of ultrasound in the diagnosis of clinically occult groin hernias in adults. Eur Radiol 2005;15(12):2457–2461.
Surgically important bowel and/or mesenteric injury in blunt trauma: accuracy of multidetector CT for evaluation. Radiology 2008;249(2):524–533.
Diagnosis of inguinal region hernias with axial CT: the lateral crescent sign and other key findings. Radiographics 2011;31(2):E1–E12.
Internal hernia following Roux-en-Y gastric bypass surgery for morbid obesity: evaluation of radiographic findings at small-bowel examination. Radiology 2009;251(3):762–770.
Internal hernia with volvulus and intussusception: case report. Abdom Imaging 2004;29(2):164–165.
Multimodality imaging of the pediatric diaphragm: anatomy and pathologic conditions. Radiographics 2010;30(7):1797–1817.
Radiologic anatomy of the inguinofermal region: insights from MDCT. AJR 2007;189(4):W177–W183.
The diagnosis and classification of inguinal and femoral hernia on multisection spiral CT. Clin Radiol 2008;63(2):184–192.
Cytoreduction and hyperthermic intraperitoneal chemotherapy in the treatment of peritoneal carcinomatosis from pseudomyxoma peritonei. World J Gastroenterol 2008;14(44):6817–6823.
Retroperitoneal fibrosis: a review of clinical features and imaging findings. AJR 2008;191(2):423–431.
Pictorial essay: multitechnique imaging findings of prolene plug hernia repair. AJR 2010;195:701–706.
Case 108: sclerosing encapsulating peritonitis. Radiology 2007;242(3):937–939.
CT of blunt diaphragmatic rupture. Radiographics 2012;32(2):477–498.
Pathologic and MR imaging features of benign fibrous soft-tissue tumors in adults. Radiographics 2007;27(1):173–187.
CT can help the surgeon consider conversion from laparoscopic to open cholecystectomy. Radiology 2012;263(1):128–138.
Autoimmune pancreatitis associated with idiopathic retroperitoneal fibrosis. AJR 2003;181(4):993–995.
Subcutaneous and breast metastasis from asymptomatic gallbladder carcinoma. Hepatobiliary Pancreat Dis Int 2009;8(2):209–211.
Foreign objects encountered in the abdominal cavity at CT. Radiographics 2011;31(2):409–428.
Computed tomography appearances of sclerosing encapsulating peritonitis. Clin Radiol 2007;62(8):732–737.
US of the peritoneum. Radiographics 2003;23(3):663–684: discussion 684-685.
Pseudomyxoma peritonei. Clin Oncol (R Coll Radiol) 2004;15(2):73–77.
CT findings in sclerosing mesenteritis (panniculitis): spectrum of disease. Radiographics 2003;23(6):1561–1567.
Sensitivity and specificity of eight CT signs in the preoperative diagnosis of internal mesenteric hernia following Roux-en-Y gastric bypass surgery. Clin Radiol 2009;64(4):373–380.
Pseudomyxoma peritonei: review on a cluster of peritoneal mucinous diseases. Acta Chir Belg 2005;105(2):127–133.
Practice patterns in percutaneous image-guided intraabdominal abscess drainage: survey of academic and private practice centers. Radiology 2004;233(3):750–756.
The molecular biology of peritoneal carcinomatosis from gastrointestinal cancer. Ann Acad Med Singapore 2003;32(2):219–225.
The elephant trunk procedure for aortic aneurysm repair: an illustrated guide to surgical technique with CT correlation. AJR 2011;197:W1052–W1059.
Imaging manifestations of abdominal fat necrosis and its mimics. Radiographics 2011;31(7):2021–2034.
Combined transmesocolic and left paraduodenal hernia: barium, CT and MRI features. Abdom Imaging 2007;32(2):224–227.
Esophageal varices in patients with cirrhosis: multidetector CT esophagography—comparison with endoscopy. Radiology 2007;242(3):759–768.
Diagnostic problems of abdominal desmoids tumors in various locations. Eur J Radiol 2007;62(2):180–185.
Helical CT with sagittal and coronal reconstructions: accuracy for detection of diaphragmatic injury. AJR 2002;179(2):451–457.
Aggressive fibromatosis: MRI features with pathologic correlation. AJR 2006;186(1):247–254.
Infected (mycotic) aneurysms: spectrum of imaging appearances and management. Radiographics 2008;28(7):1853–1868.
From the archives of the AFIP: benign fibrous tumors and tumorlike lesions of the mesentery: radiologic-pathologic correlation. Radiographics 2006;26(1):245–264.
Internal hernia after gastric bypass: sensitivity and specificity of seven CT signs with surgical correlation and controls. AJR 2007;188:745–750.
Diffusion-weighted MR imaging for the whole body metastatic disease and lymphadenopathy. Magn Reson Imaging Clin N Am 2009;17(2):245–261.
The Rigler sign. Radiology 2003;228(3):706–707.
Review of internal hernias: radiographic and clinical findings. AJR 2006;186(3):703–717.
MRI and biologic behavior of desmoids tumors in children. AJR 2007;189(3):633–640.
Best cases from the AFIP: extraabdominal desmoids-type fibromatosis. Radiographics 2008;28(3):901–906.
Recurrent prostatic stromal sarcoma with massive high-grade prostatic intraepithelial neoplasia. J Clin Pathol 2007;60(3):330–332.
Imaging of the diaphragm: anatomy and function. Radiographics 2012;32(2):E51–E70.
Fitz-Hugh-Curtis syndrome: radiologic manifestation. J Comput Assist Tomogr 2003;27(5):786–791.
Primary retroperitoneal neoplasms: CT and MR findings with anatomic and pathologic diagnostic clues. Radiographics 2003;23(1):45–57.
Small bowel obstruction related to left side paraduodenal hernia: CT findings. Abdom Imaging 2005;30(1):53–55.
Recurrent ovarian malignancy: patterns and spectrum of imaging findings. Abdom Imaging 2003;28(3):404–415.
CT assessment of anastomotic bowel leak. Clin Radiol 2007;62(1):37–42.
Beyond appendicitis: common and uncommon gastrointestinal causes of right lower quadrant abdominal pain at multidetector CT. Radiographics 2011;31(4):927–947.
Peritoneal carcinomatosis. Eur Radiol 2001;11(11):2195–2206.
Clinical observations: diagnosis of transmesocolic internal hernia as a complication of retrocolic gastric bypass: CT imaging criteria. AJR 2007;189:52–55.
Multidetector-row CT of right hemidiaphragmatic rupture caused by blunt trauma: a review of 12 cases. Clin Radiol 2005;60(12):1280–1289.
Inguinofemoral hernia: accuracy of sonography in patients with indeterminate clinical features. AJR 2006;187(5):1168–1178.
Colonoscopy after CT diagnosis of diverticulitis to exclude colon. Radiology 2012;263:383–390.
CT findings of rupture, impending rupture, and contained rupture of abdominal aortic aneurysms. AJR 2007;188(1):W57–W62.
Imaging of groin masses: inguinal anatomy and pathologic conditions revisited. Radiographics 2001;21(Spec. No):S261–S271.
Pictorial essay: A to Z of desmoid tumors. Am J Roentgenol 2011;197(6):W1008–W1014.
Neoplastic iliopsoas masses in oncology patients: CT findings. Abdom Imaging 2008;33(4):493–497.
Omental infarct: CT imaging features. Abdom Imaging 2006;31:549–554.
Taxonomy and imaging spectrum of small bowel obstruction after Roux-en-Y gastric bypass surgery. AJR 2010;194:120–128.
Pathogenesis of malignant ascites: Starling’s law of capillary hemodynamics revisited. Ann Oncol 2001;12(10):1353–1357.
Nodal status of malignant lymphoma in pelvic and retroperitoneal lymphatic pathways: PET/CT. Abdom Imaging 2010;35(2):232–240.
Pattern of the month: patterns of fat stranding. AJR 2011;197:W1–W14.
Pictorial essay: imaging features of encapsulating peritoneal sclerosis in continuous ambulatory peritoneal dialysis patients. AJR 2010;195:W50–W54.
Peritoneal and retroperitoneal anatomy and its relevance for cross-sectional imaging. Radiographics 2012;32(2):437–451.
Clinical perspective: an unusual cause of intestinal obstruction: abdominal cocoon. AJR 2010;194:W176–W178.
Best cases from the AFIP: multicystic mesothelioma. Radiographics 2004;24(1):247–250.
Abdominal hernias: CT findings. AJR 1995;164:1391–1395.
∗ From epipluo (Greek root) “to float upon” as in the omentum that floats upon abdominal contents (omentum in Latin).
∗ Vincent Bochdalek (1801-1883), Bohemian anatomist.
† Giovanni Morgagni (1682-1771), Italian anatomist.
∗ James Rutherford Morison (1853-1939), British surgeon.
† Leo George Rigler (1896-1979), American radiologist.