[level-membership-for-radiology-category] Most common type of CCA










 and bile ducts
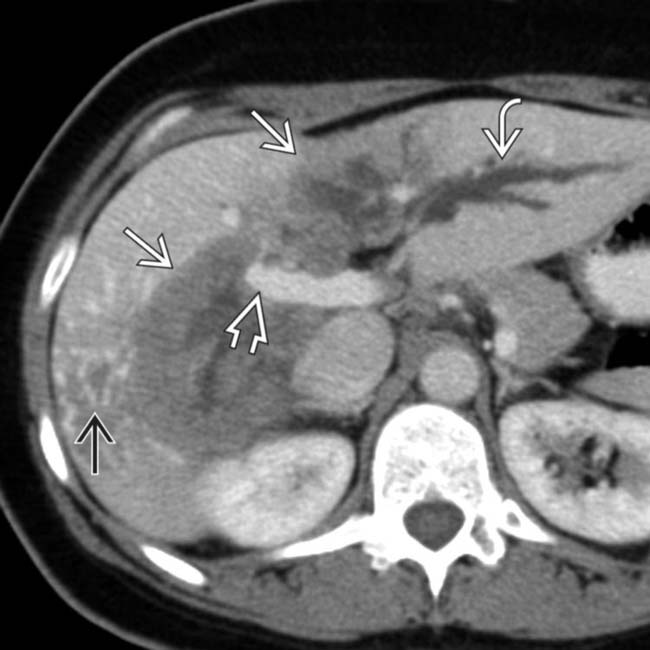
and bile ducts  encased and obstructed by the tumor
encased and obstructed by the tumor  , accounting for the altered perfusion of the right hepatic lobe. Hepatic veins were encased as well, resulting in collateral blood vessels seen within the right lobe
, accounting for the altered perfusion of the right hepatic lobe. Hepatic veins were encased as well, resulting in collateral blood vessels seen within the right lobe  .
.
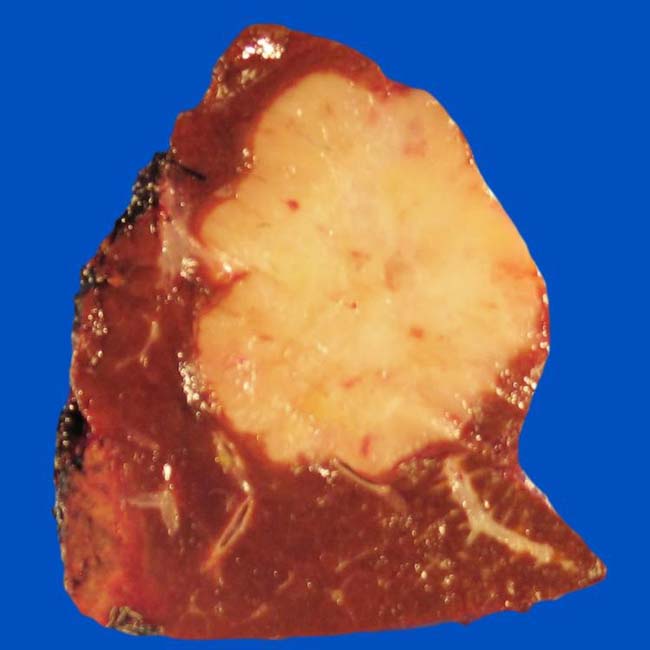
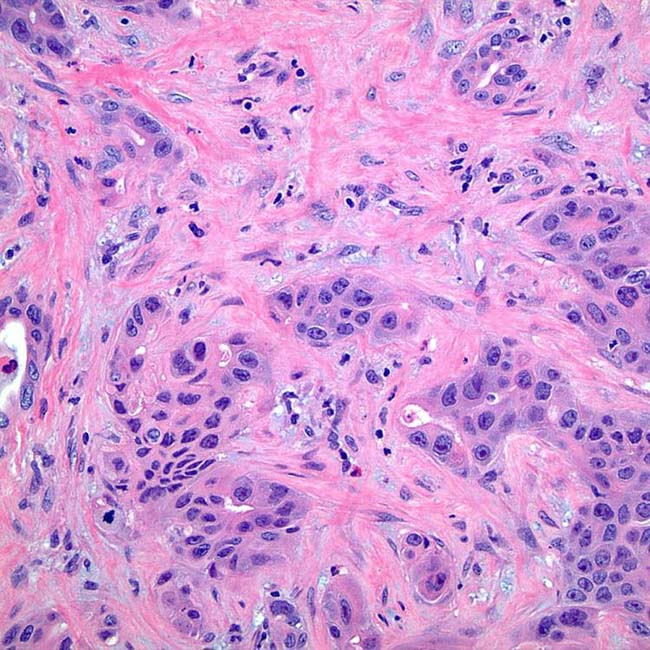
 , a feature of cholangiocarcinoma (and other tumors with fibrous stroma).
, a feature of cholangiocarcinoma (and other tumors with fibrous stroma).IMAGING
General Features







CT Findings

• CECT
 Mass-forming PCC
Mass-forming PCC
Mass-forming PCC
– Thin or thick rim-like enhancement frequently seen around periphery of tumor on arterial phase images



































 .
.
 . The intrahepatic bile ducts are dilated
. The intrahepatic bile ducts are dilated  , and the left lobe of the liver is atrophic. Parenchymal atrophy of liver segments affected by peripheral cholangiocarcinoma is common and may be evident as lobar atrophy or capsular retraction.
, and the left lobe of the liver is atrophic. Parenchymal atrophy of liver segments affected by peripheral cholangiocarcinoma is common and may be evident as lobar atrophy or capsular retraction.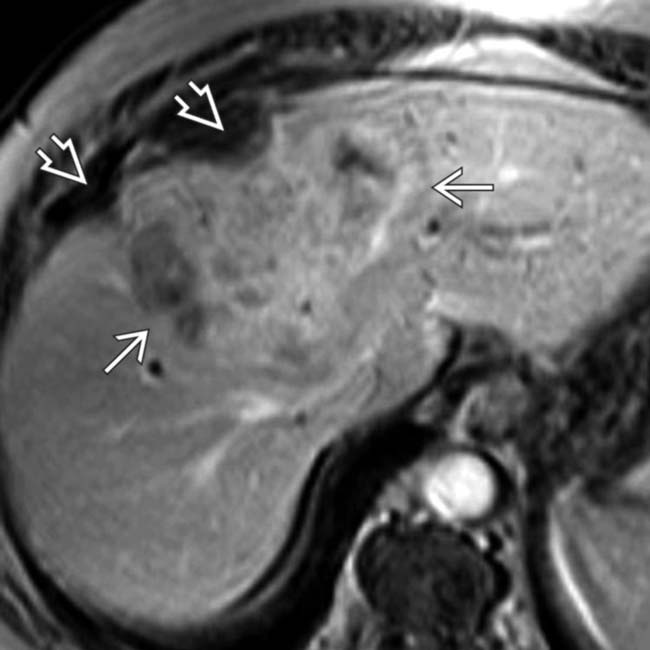
 . Capsular retraction
. Capsular retraction  is also noted. This tumor showed persistent enhancement on 10-minute delayed images.
is also noted. This tumor showed persistent enhancement on 10-minute delayed images.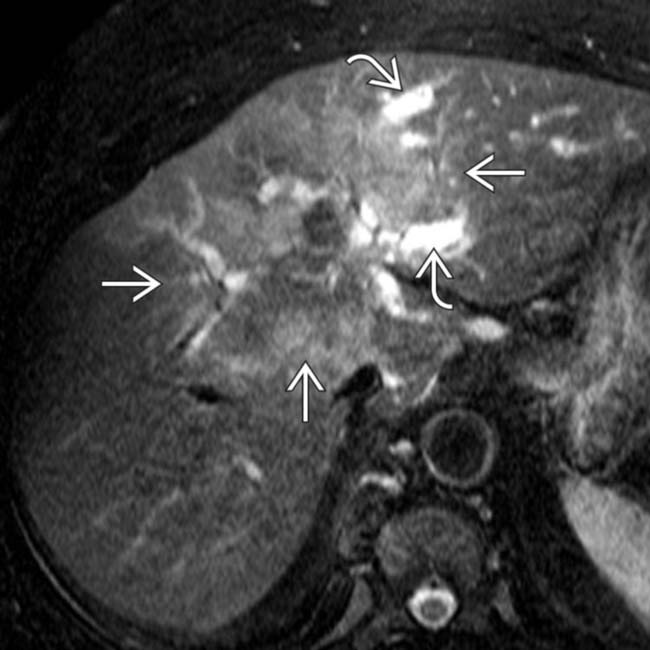
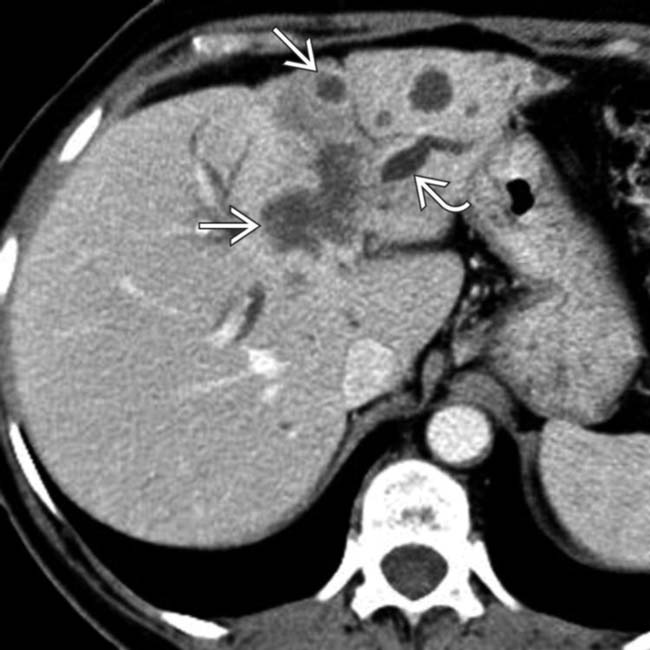
 . Dilated intrahepatic ducts
. Dilated intrahepatic ducts  are noted upstream from the mass. This is a typical feature of cholangiocarcinoma but may be seen with other tumors.
are noted upstream from the mass. This is a typical feature of cholangiocarcinoma but may be seen with other tumors.
 with heterogeneous minimal enhancement. Hepatic capsular retraction
with heterogeneous minimal enhancement. Hepatic capsular retraction  is a prominent feature of this cholangiocarcinoma.
is a prominent feature of this cholangiocarcinoma.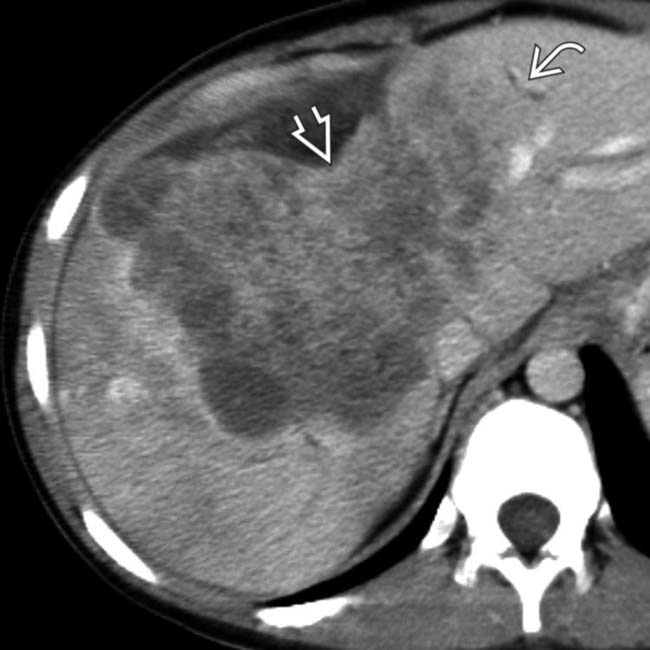
 , and there is marked retraction of the liver capsule
, and there is marked retraction of the liver capsule  .
.
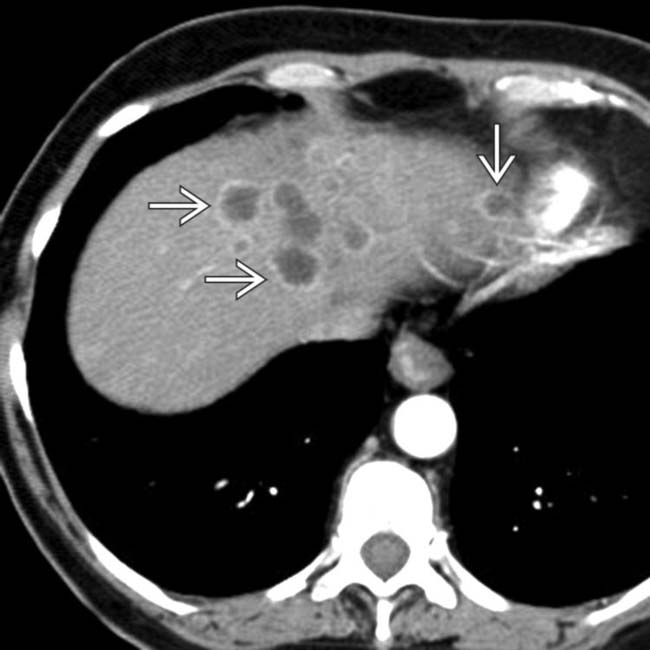
 filling much of the right lobe of the liver. The mass obstructs central bile ducts, causing dilation of the peripheral intrahepatic ducts
filling much of the right lobe of the liver. The mass obstructs central bile ducts, causing dilation of the peripheral intrahepatic ducts  .
.
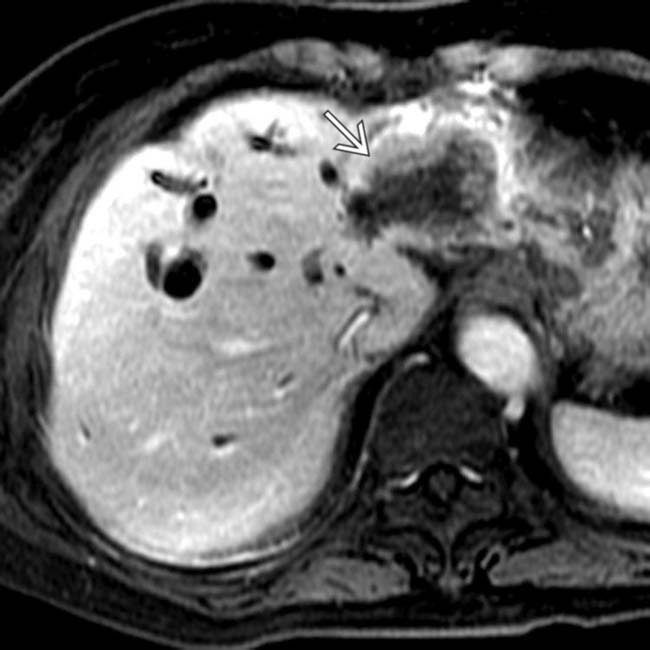
 encases the portal vein
encases the portal vein  . The delayed set of images (not shown) showed some persistent enhancement in some parts of the tumor and no washout.
. The delayed set of images (not shown) showed some persistent enhancement in some parts of the tumor and no washout.
 with dilation of intrahepatic bile ducts
with dilation of intrahepatic bile ducts  . The CT findings are typical, but not diagnostic, of cholangiocarcinoma.
. The CT findings are typical, but not diagnostic, of cholangiocarcinoma.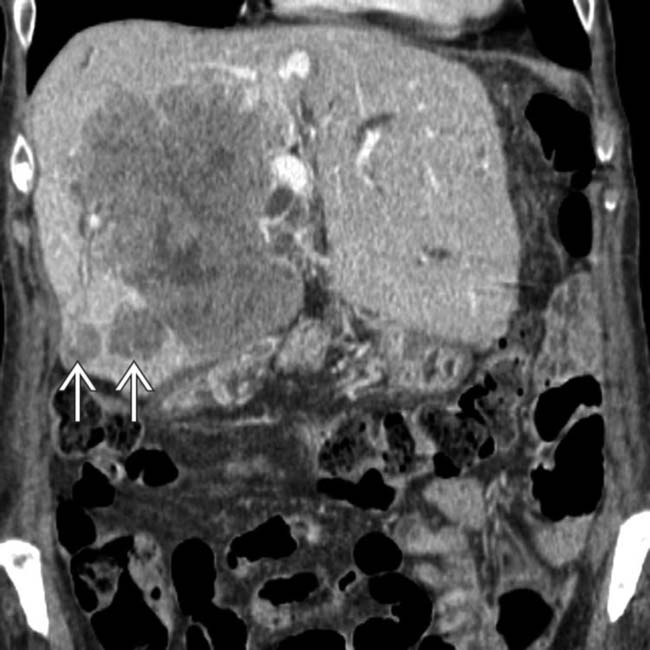
 , a common feature of intrahepatic cholangiocarcinoma. The term “peripheral” cholangiocarcinoma seems to be a misnomer in cases such as this, but it implies that the tumor arose from intrahepatic bile ducts.
, a common feature of intrahepatic cholangiocarcinoma. The term “peripheral” cholangiocarcinoma seems to be a misnomer in cases such as this, but it implies that the tumor arose from intrahepatic bile ducts.
 with stones and pus within the dependent ducts
with stones and pus within the dependent ducts  . Marked ductal dilation plus lobar atrophy of the left lobe are caused by an obstructing mass
. Marked ductal dilation plus lobar atrophy of the left lobe are caused by an obstructing mass  .
.
 and the intrahepatic ductal dilation. Cholangiocarcinoma was confirmed at left hepatic resection.
and the intrahepatic ductal dilation. Cholangiocarcinoma was confirmed at left hepatic resection.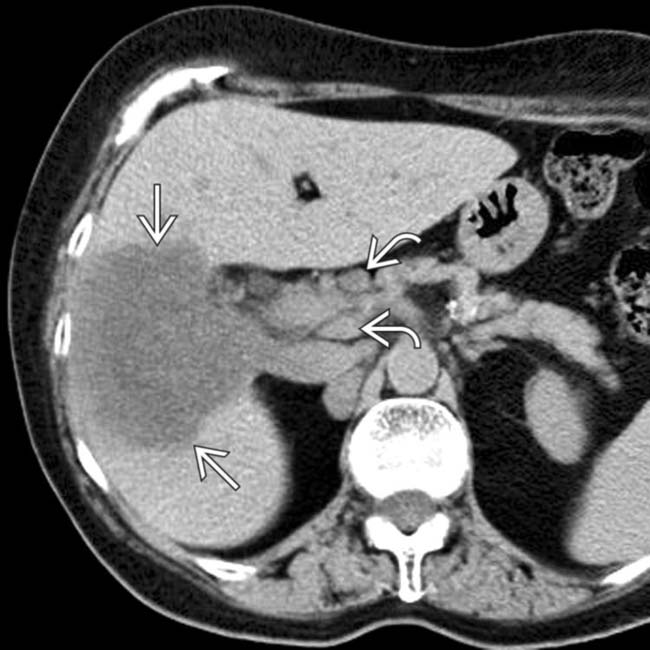
 with porta hepatic lymphadenopathy
with porta hepatic lymphadenopathy  .
.

 have the same enhancement pattern as the intrahepatic cholangiocarcinoma, indicating nodal metastases.
have the same enhancement pattern as the intrahepatic cholangiocarcinoma, indicating nodal metastases.
 , but the lesion does not fill in from the periphery as would be expected of a hemangioma.
, but the lesion does not fill in from the periphery as would be expected of a hemangioma.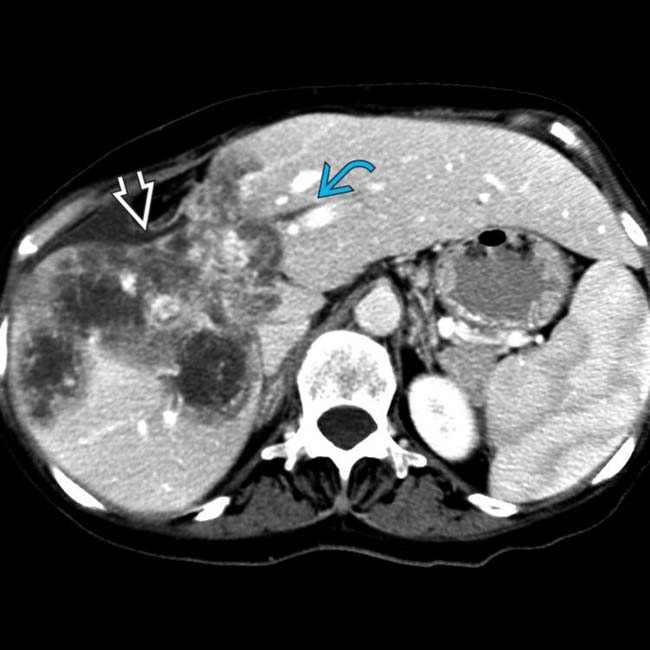
 and volume loss with capsular retraction
and volume loss with capsular retraction  .
.
 due to its fibrous stroma. Other tumor foci have the “target” pattern of enhancement
due to its fibrous stroma. Other tumor foci have the “target” pattern of enhancement  of other types of adenocarcinomas.
of other types of adenocarcinomas.


 along with low-intensity, nonenhancing (fibrotic/necrotic) areas.
along with low-intensity, nonenhancing (fibrotic/necrotic) areas.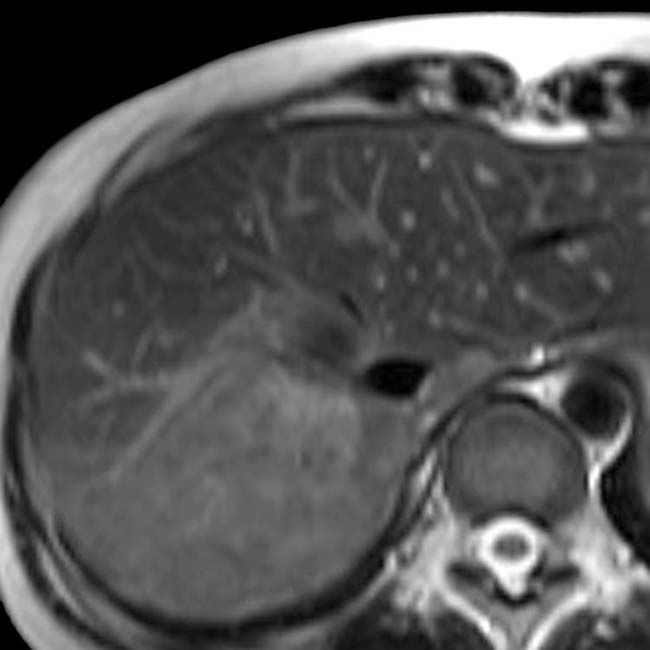
[/level-membership-for-radiology-category][not-level-membership-for-radiology-category] Most common type of CCA
and bile ducts encased and obstructed by the tumor , accounting for the altered perfusion of the right hepatic lobe. Hepatic veins were encased as well, resulting in collateral blood vessels seen within the right lobe ., a feature of cholangiocarcinoma (and other tumors with fibrous stroma).IMAGING
General Features
CT Findings
• CECT
Mass-forming PCC
Mass-forming PCC
– Thin or thick rim-like enhancement frequently seen around periphery of tumor on arterial phase images
MR Findings
• T1WI C+
 Dynamic MR: Minimal or moderate rim enhancement and progressive and concentric filling with contrast material
Dynamic MR: Minimal or moderate rim enhancement and progressive and concentric filling with contrast material
Dynamic MR: Minimal or moderate rim enhancement and progressive and concentric filling with contrast material
–
Buy Membership for Radiology Category to continue reading. Learn more here
[/not-level-membership-for-radiology-category]
