Chapter 30 Percutaneous Pedicle Screw Fixation
Anterior lumbar interbody fusion (ALIF) has advantages over other fusion procedures, such as shorter operating time, lower blood loss, and no epidural complications [1–6]. However, in the case of spondylolytic or degenerative spondylolisthesis at multiple vertebral levels, higher pseudarthrosis rates have been reported with ALIF [7,8].
Percutaneous pedicle screw fixation (PPF) was developed as a minimally invasive posterior augmentation for ALIF [9]. At present, the PPF technique has been applied to a wide range of fusion procedures, including mini–open transforaminal lumbar interbody fusion (TLIF) [10].













Preoperative preparation
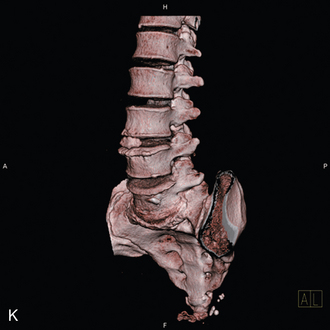
 Computed tomography is used to ascertain the size of the pedicle and to plan the length and direction of the screw (Fig. 30-1).
Computed tomography is used to ascertain the size of the pedicle and to plan the length and direction of the screw (Fig. 30-1).
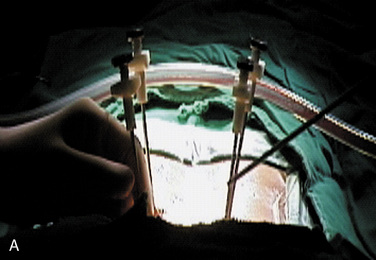
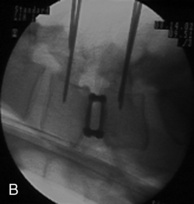
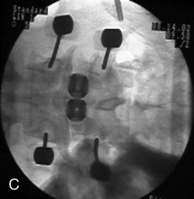
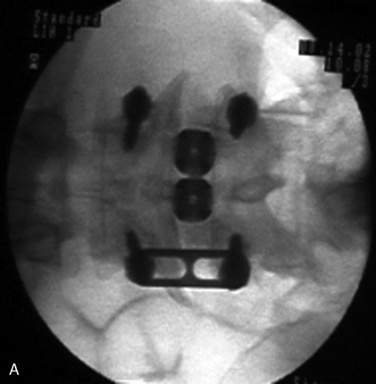
 For older women, a bone density study helps determine whether the bone mineral content is adequate for pedicle screw fixation. In patients with severe osteoporosis, vertebral augmentation by vertebroplasty is needed (Fig. 30-2).
For older women, a bone density study helps determine whether the bone mineral content is adequate for pedicle screw fixation. In patients with severe osteoporosis, vertebral augmentation by vertebroplasty is needed (Fig. 30-2).

Procedures
Procedure for Percutaneous Pedicle Screw in General





Procedure for Use of the Sextant System
Patient Positioning and Operating Room Setup


Procedure for Percutaneous Pedicle Screw Fixation
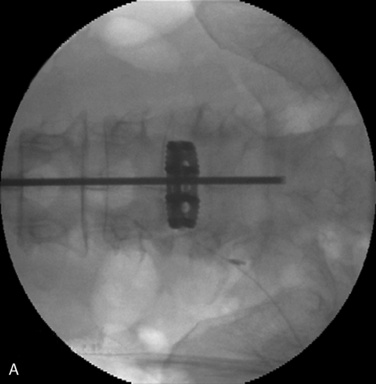

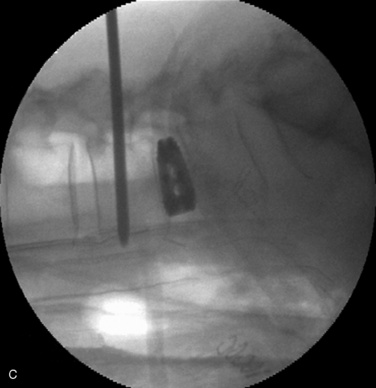
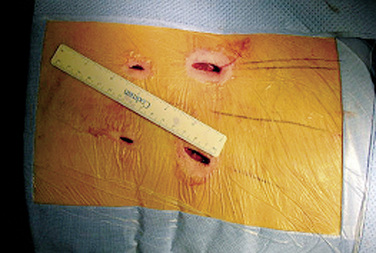
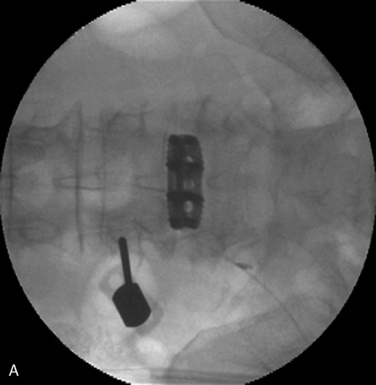
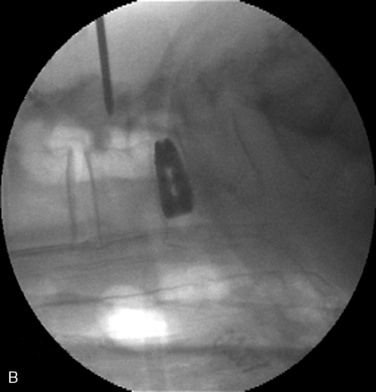
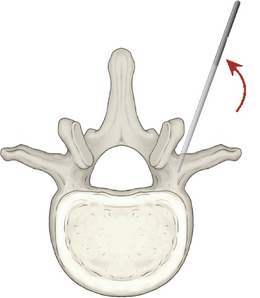
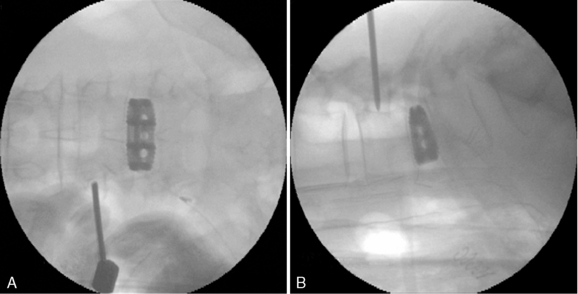
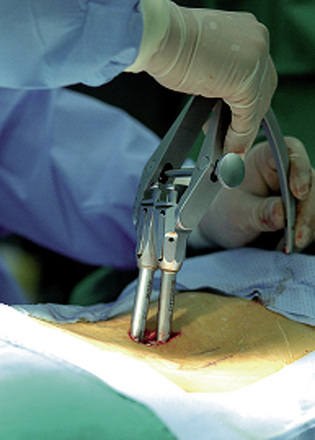
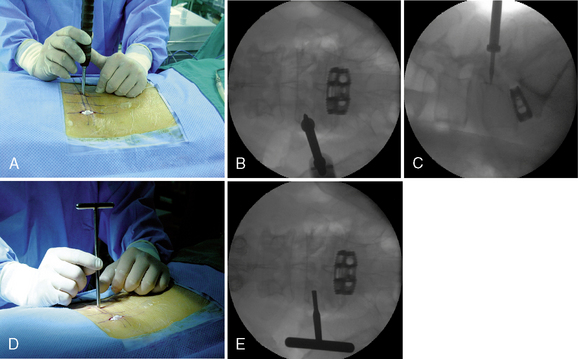
Figure 30–14 The pedicle is tapped with the cannulated tap needle. Intraoperative view (A) and fluoroscopic lateral view (B).

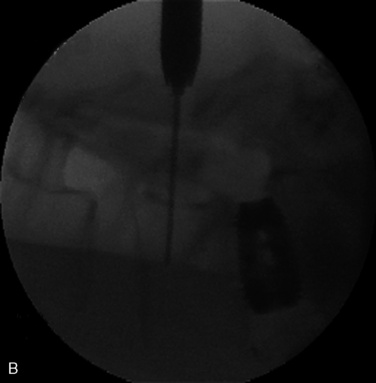

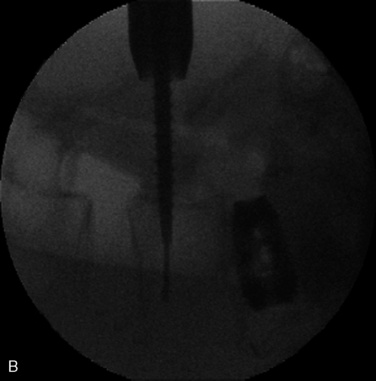
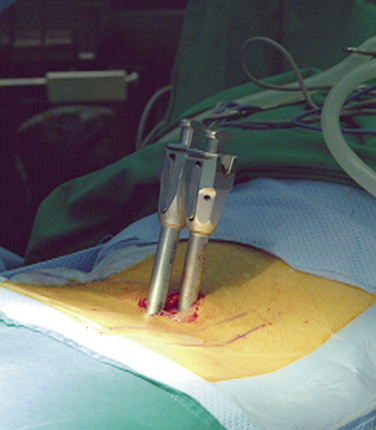
Figure 30–17 Rotation of the extenders so that the two flat sides are facing each other makes no gap between the two extenders.

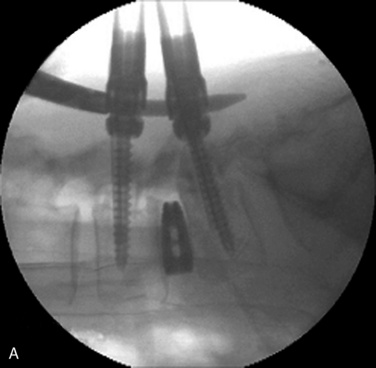
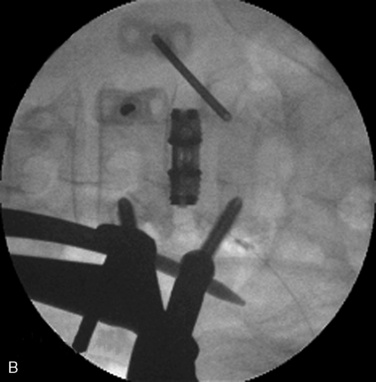


Figure 30–20 Appropriate forces with compression (A) or distraction (B) can be applied to the construct prior to final tightening.

Limitations of the Sextant System





Modified methods allow for these limitations
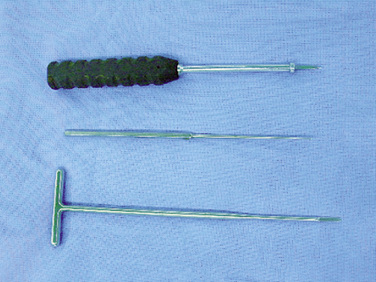
 An adjuvant instrument, such as an awl, T-probe, or long, straight, beaded-tip probe, can be used for checking the wall of the body (Fig. 30-23).
An adjuvant instrument, such as an awl, T-probe, or long, straight, beaded-tip probe, can be used for checking the wall of the body (Fig. 30-23). An awl is placed on the junction of the facet and transverse process under fluoroscopic guidance. The tip of awl should reach the pedicle–vertebral body junction on the lateral view, and it should be positioned in the center of the pedicle on the anteroposterior view (Fig. 30-24).
An awl is placed on the junction of the facet and transverse process under fluoroscopic guidance. The tip of awl should reach the pedicle–vertebral body junction on the lateral view, and it should be positioned in the center of the pedicle on the anteroposterior view (Fig. 30-24).
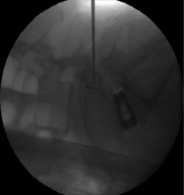
 A long, straight, beaded-tip probe (wall checker) is inserted into the pedicle and vertebral body. The wall checker is used to palpate the bony surface of the pedicle for proper insertion of the screw and to prevent screw misplacement (Fig. 30-25).
A long, straight, beaded-tip probe (wall checker) is inserted into the pedicle and vertebral body. The wall checker is used to palpate the bony surface of the pedicle for proper insertion of the screw and to prevent screw misplacement (Fig. 30-25).
Complications
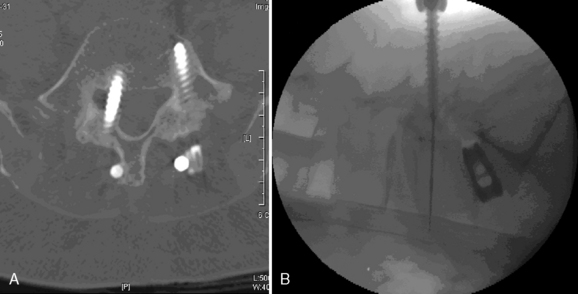
Screw misplacement is a well-known complication of open pedicle screw placement, and it is certainly a potential problem in PPF (Fig. 30-26). Unlike with open surgery, there are no visible landmarks, and there is little palpation feedback during navigation of the pedicle. The surgeon must rely on the quality of the fluoroscopic images and his or her ability to interpret the images.
CASE STUDY 30.1 Lytic Spondylolisthesis at the L4-L5 Level Corrected by Percutaneous Pedicle Screws Without Laminectomy
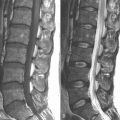
A 45-year-old woman experienced severe neurologic claudication in both legs. Magnetic resonance imaging and plain films demonstrated lytic spondylolisthesis at the L4-L5 level (Fig. 30-27A and B). The anterior lumbar interbody fusion with pecutaneous pedicle screw was performed without laminectomy. Postoperative radiographs confirmed no laminectomy, acceptable pedicle screw placement, good reduction of slippage, and increased disc height (Fig. 30-27C and D).

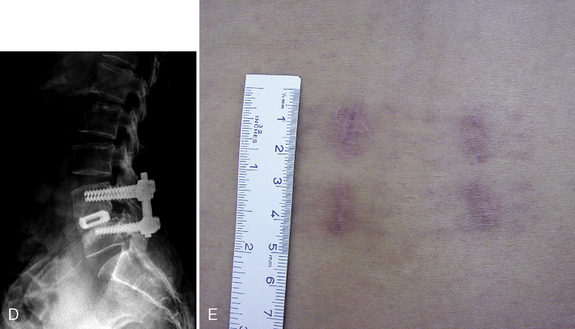
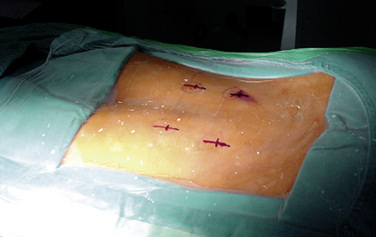
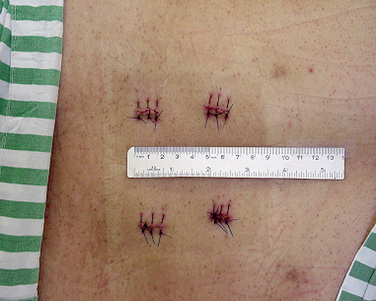
Figure 30–27 Case Study 30.1: Lytic spondylolisthesis at the L4-L5 level demonstrated on preoperative lateral magnetic resonance image (A) and plain film (B). (C) Postoperative anteroposterior radiograph demonstrates no laminectomy and acceptable screw placement. (D) Postoperative lateral radiograph reveals good reduction of slippage and increased disc height. (E) Photograph taken 4 months after surgery showing 15-mm skin incisions for each pedicle screw.
CASE STUDY 30.2 Lytic Spondylolisthesis at the L4-L5 Level Corrected by Percutaneous Pedicle Screws Without Laminectomy
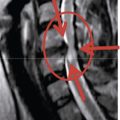
Magnetic resonance imaging and plain radiographs demonstrated that a 55-year-old woman had severe lytic spondylolisthesis at the L4-L5 level (Fig. 30-28A and B). The anterior lumbar interbody fusion with pecutaneous pedicle screw (sextant system) was performed without laminectomy. Postoperative radiographs demonstrated acceptable screw placement, good reduction of slippage, and increased disc height (Fig. 30-28C and D).

Figure 30–28 Case Study 30.2: Severe lytic spondylolisthesis at L4-L5 demonstrated on preoperative sagittal magnetic resonance image (A) and lateral plain film (B). (C) Postoperative anteroposterior radiograph demonstrates acceptable screw placement. (D) Postoperative lateral radiograph shows good reduction of slippage and increased disc height.
1 Lee S.H., Choi W.G., Lim S.R., et al. Minimally invasive anterior lumbar interbody fusion followed by percutaneous pedicle screw fixation for isthmic spondylolisthesis. Spine J. 2004;4:644-649.
2 Choi W.G., Lee S.H., Jung B.J., et al. Mini-open anterior lumbar interbody fusion and simultaneous percutaneous pedicle screw fixation for low-grade isthmic spondylolisthesis with leg pain. Korean J Spine. 2004;1:255-262.
3 Chang S.B., Lee S.H., Lee S.C., et al. Anterior lumbar interbody fusion with Chuinard & Peterson bone graft and posterior percutaneous facet screw fixation for post-discectomy pyogenic spondylitis. Korean J Spine. 2004;1:76-82.
4 Shim C.S., Lee S.H., Jung B.J., et al. Fluoroscopically-assisted percutaneous facet screw fixation following anterior lumbar interbody fusion. Spine. 2005;30:838-843.
5 Jang J.S., Lee S.H., Lim S.R. Guide device for percutaneous placement of translaminar facet screws after anterior lumbar interbody fusion: Technical note. J Neurosurg. 2003;98:100-103.
6 Jang J.S., Lee S.H. Clinical analysis of percutaneous facet screw fixation after anterior lumbar interbody fusion. J Neurosurg Spine. 2005;3:40-46.
7 Herkowitz H.N., Kurz L.T. Degenerative lumbar spondylolisthesis with spinal stenosis: A prospective study comparing decompression with decompression and intertransverse process arthrodesis. J Bone Joint Surg Am. 1991;73:802-808.
8 Fischgrund J.S., Mackay M., Herkowitz H.N., et al. Volvo award winner in clinical studies: Degenerative lumbar spondylolisthesis with spinal stenosis: A prospective, randomized study comparing decompressive laminectomy and arthrodesis with and without spinal instrumentation. Spine. 1997;22:2807-2812.
9 Lowery G.L., Kulkarni S.S. Posterior percutaneous spine instrumentation. Eur Spine J. 2000;1:S126-S130.
10 Jang J.S., Lee S.H. Minimally invasive transforaminal lumbar interbody fusion with ipsilateral pedicle screw and contralateral facet screw fixation. J Neurosurg Spine. 2005;3:218-223.
11 Kim D.Y., Lee S.H., Chung S.K., Lee H.Y. Comparison of multifidus muscle atrophy and trunk extension muscle strength: Percutaneous versus open pedicle screw fixation. Spine. 2005;30:123-129.