[level-membership-for-radiology-category]
Penetrating foreign bodies
Appearances on plain radiographs
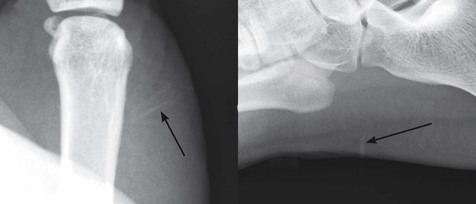
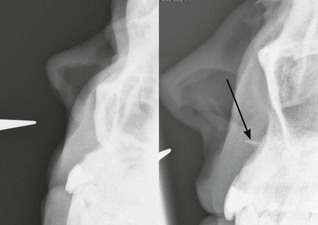
Glass
All glass is radio-opaque. Visibility of glass is not dependent on its lead content1,2.
The radiographic density of the different types of glass does vary. Imaging technique is important. A soft tissue exposure is essential.
Zooming on a digital image is often necessary, otherwise very small fragments are easily overlooked.
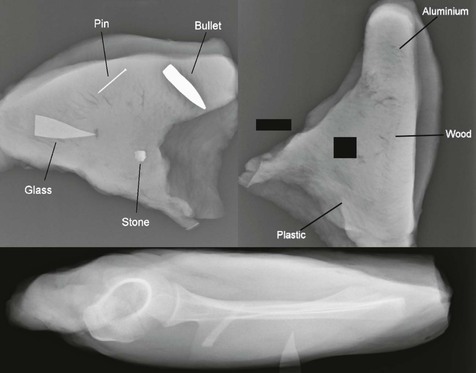
Metal
Most metals are radio-opaque. A notable exception is aluminium.
Wood or plastic
Only occasionally will wood be visualised3–5. A splinter might be well defined on a radiograph if the fragment has paint on its surface.
Why is wood almost non-opaque on a radiograph?
In clinical practice it is best to assume that all splinters, thorns, and fragments of plastic will be non-opaque on a radiograph.

Suspected foreign bodies
Soft tissue laceration6–8
Foreign body detection
First choice in the Emergency Department: plain radiography.
Back up options in specific cases:
□ Glass, metal, wood and plastic well visualised.
□ But… operator dependent, and will detect superficial foreign bodies only.
▪ CT.
□ Most foreign bodies are well visualised.
□ Wood can be difficult to visualise.
▪ MRI.
Foreign body removal
Prior to surgical exploration it will sometimes be helpful if the precise position of a glass fragment or wooden splinter is shown beneath the skin. In these instances sonography can provide guidance at the time of removal. If a foreign body is situated deep in the soft tissues and sonography cannot provide the required information, then CT or MRI will often provide excellent localisation.
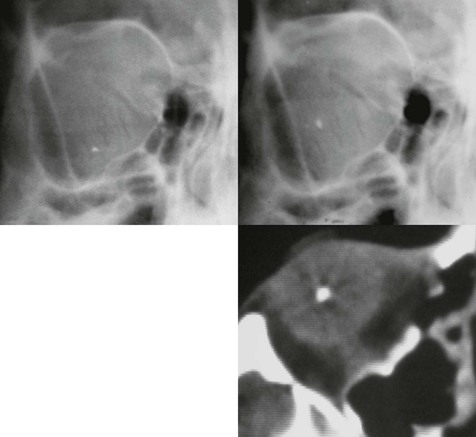
Orbital injury
Foreign body detection10,11
Most foreign bodies will be detected with slit lamp ophthalmoscopy.
Plain radiography, ultrasound, or CT will be of assistance in selected cases.
▪ Glass or metal fragments
Plain film radiography is recommended.
▪ Wood or plastic fragments
Sonography is recommended. The accuracy of detection is dependent on an experienced operator and the quality of the equipment. CT is an alternative to ultrasound and is the preferred investigation in some centres. CT is sensitive, shows the retrobulbar space better than ultrasound, and is less operator-dependent10. MRI is also available. It can be utilised when CT findings are uncertain11. A history of a ferromagnetic foreign body injury to the orbit is a contraindication to a MRI examination.
Foreign body removal
Ultrasound or CT can provide accurate localisation prior to exploration of the orbit10.
[/level-membership-for-radiology-category][not-level-membership-for-radiology-category]
Penetrating foreign bodies
Appearances on plain radiographs
Glass
All glass is radio-opaque. Visibility of glass is not dependent on its lead content1,2.
The radiographic density of the different types of glass does vary. Imaging technique is important. A soft tissue exposure is essential.
Zooming on a digital image is often necessary, otherwise very small fragments are easily overlooked.
Metal
Most metals are radio-opaque. A notable exception is aluminium.
Wood or plastic
Only occasionally will wood be visualised3–5. A splinter might be well defined on a radiograph if the fragment has paint on its surface.
Why is wood almost non-opaque on a radiograph?
In clinical practice it is best to assume that all splinters, thorns, and fragments of plastic will be non-opaque on a radiograph.
[/not-level-membership-for-radiology-category]
