CHAPTER NINE PELVIS AND SACROILIAC JOINT
INTRODUCTION
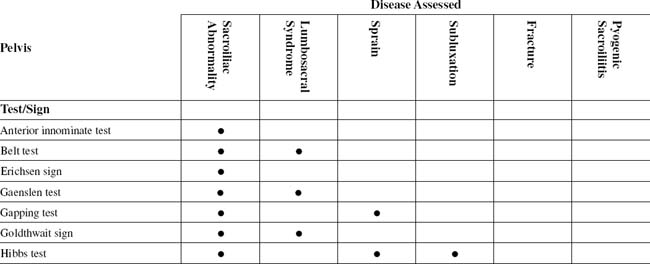
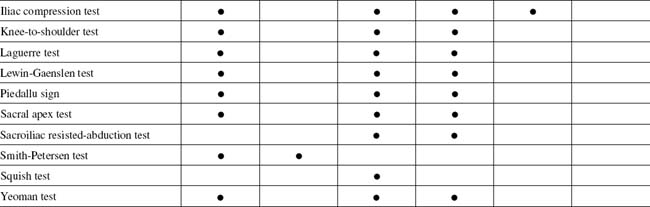
TABLE 9-2 PELVIS AND SACROILIAC JOINT CROSS-REFERENCE TABLE BY SYNDROME OR TISSUE
| Fracture | Iliac compression test |
| Lumbosacral syndrome |
The stability of the sacroiliac joint lies in the nature of its articular surfaces and ligaments. Cardinal in this role are the dense, interosseous ligaments lying dorsal to the joint and the ventral sacroiliac ligament covering its anterior aspect.
ESSENTIAL ANATOMY
ORTHOPEDIC GAMUT 9-2 SUPERIOR HALF OF THE PELVIS
Interior surfaces of the superior half of the pelvis include:
The lumbosacral plexus takes shape on the medial surface of the levator ani muscle (Table 9-3).
| Anterior Divisions | Posterior Divisions |
|---|---|
| Nerve to quadratus femoris/inferior gemellus | Nerve to piriformis |
| Superior gluteal nerve | |
| Nerve to obturator internus/superior gemellus | Inferior gluteal nerve |
| Posterior femoral cutaneous nerve* | |
| Posterior femoral cutaneous nerve* | Common peroneal nerve |
* Both divisions contribute to this nerve.
Adapted from Mathers LH et al: Clinical anatomy principles, St Louis, 1996, Mosby.
ESSENTIAL MUSCLE FUNCTION ASSESSMENT
ORTHOPEDIC GAMUT 9-3 LUMBOPELVIC FLEXIBILITY TESTING PROCEDURES
ANTERIOR INNOMINATE TEST
ALSO KNOWN AS MAZION PELVIC MANEUVER
Assessment for Unilateral Forward Displacement of the Ilia on the Sacrum
Comment
Many cases of acute low back pain that are not correctly identified evolve into a chronic spinal problem with significant disability at the muscular level (Table 9-4). Muscular fixation alone can be the cause of spinal joint dysfunction.
| Diagnosis | Site of Complaint |
|---|---|
| Quadratus lumborum syndrome | Gluteal region, anterior iliac spine, greater trochanter of femur |
| Gluteus maximus or medius syndrome | Sacral and gluteal region, lateral hip |
| Gluteus minimus syndrome | Lateral hip, thigh, and calf |
| Chronic lumbar strain (spinal erector muscles) | Laterally to ribs, caudally toward lumbosacral junction |
| Piriformis syndrome | Sacroiliac region; posterior hip, thigh, calf; possibly sole of foot |
Adapted from Brier SR: Primary care orthopedics, St Louis, 1999, Mosby.
PROCEDURE

PROCEDURE

PROCEDURE
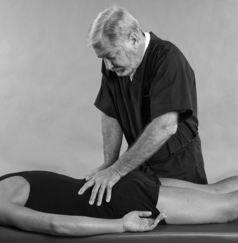
PROCEDURE

GAPPING TEST
PROCEDURE

PROCEDURE

PROCEDURE


KNEE-TO-SHOULDER TEST
PROCEDURE

PROCEDURE

LEWIN-GAENSLEN TEST
PROCEDURE

PROCEDURE

SACROILIAC RESISTED-ABDUCTION TEST
HIP-ABDUCTION STRESS TEST
Assessment for Generalized Abductor Muscular Weakness or Sprain or Subluxation of the Sacroiliac Joint
PROCEDURE

SMITH-PETERSEN TEST
Assessment for Sacroiliac Joint Involvement versus Lumbosacral Spine Involvement
Comment
ORTHOPEDIC GAMUT 9-16 INTERNATIONAL ASSOCIATION FOR THE STUDY OF PAIN DIAGNOSTIC CHARACTERISTICS FOR PATIENTS WITH SACROILIAC SYNDROME MUST POSSESS ALL OF THE FOLLOWING CHARACTERISTICS
PROCEDURE

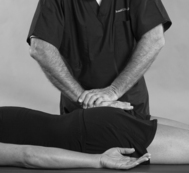
SQUISH TEST
Assessment for Posterior Sacroiliac Ligament Damage
ORTHOPEDIC GAMUT 9-20 PELVIC RING
The double fractures of the pelvic ring occur in three forms:
ORTHOPEDIC GAMUT 9-21 YOUNG AND BURGESS PELVIC FRACTURE CLASSIFICATION