Pelvis
Normal anatomy
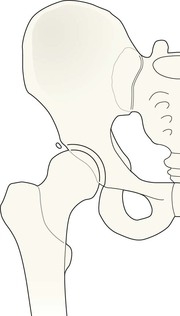
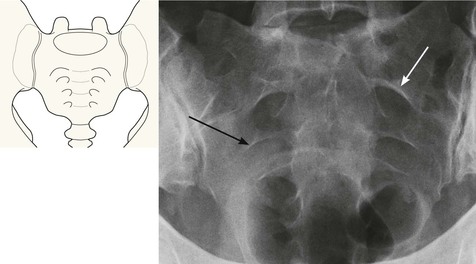
Normal AP view
The pelvis comprises three bone rings:
The robust sacro-iliac joints and the pubic symphysis are part of the main bone ring. The sacro-iliac joints are the strongest joints in the body and resist the normal vertical and anterior-posterior displacement forces; the pubic symphysis is the weakest link in the pelvic ring1–4.
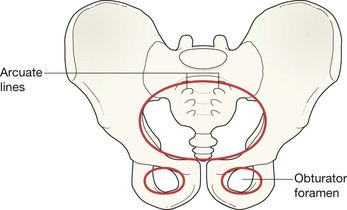
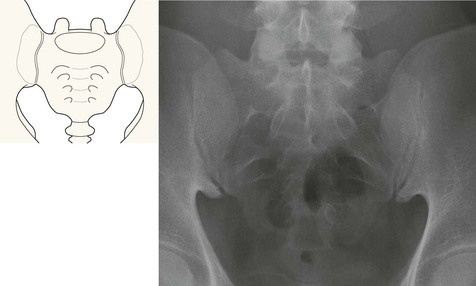
Arcuate lines are visible as smooth curved borders on the radiograph. They outline the roofs of the sacral formina.
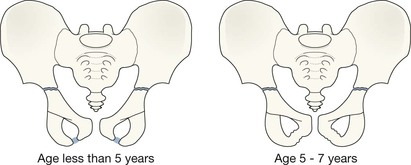
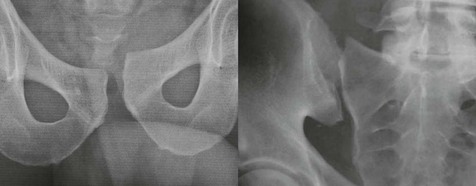
Developing skeleton: Synchondroses
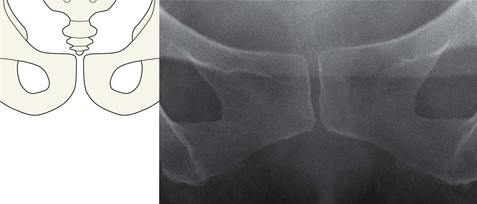
In children the synchondrosis (cartilaginous junction) between each ischial and pubic bone can sometimes appear confusing. In early childhood these unfused junctions may simulate fracture lines. Subsequently, between the ages of five and seven years, they may mimic healing fractures.
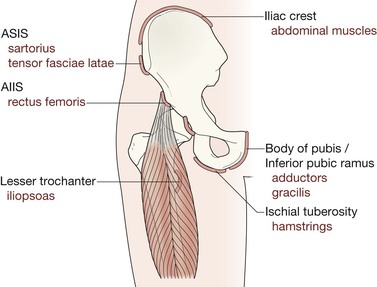
Developing skeleton: Pelvic bone apophyses5–7
In adolescents and young adults the pelvis shows several small secondary centres (the apophyses). These should be radiographically identical on the two sides.
Apophyses are secondary centres that contribute to the eventual shape, size, and contour of the bone but not to its length. These centres are traction epiphyses as muscles originate from or insert into them. They are vulnerable to severe and acute muscle contraction, and also to repetitive forceful muscle pulls when jumping, hurdling, turning suddenly, or—occasionally—when dancing.
Age of appearance and fusion of apophyses at the hip and pelvis (years)5,7
| Apophysis | First seen on radiograph | Fuses to skeleton |
| Innominate bone | ||
| AIIS | 13–15 | 16–18 |
| ASIS | 13–15 | 21–25 |
| Ischial tuberosity | 13–15 | 20–25 |
| Iliac crest | 13–15 | 21–25 |
| Femur | ||
| Lesser trochanter | 11–12 | 16–17 |
| Greater trochanter | 2–3 | 16–17 |
Note that some apophyses remain unfused and normal, but are still vulnerable into the early 20s, well after the growth of the long bones has been completed.
Analysis: the checklist
The AP radiograph
Assess:
1. The main pelvic ring. Scrutinise both the inner and outer contours.
2. The two small rings forming the obturator foramina.
3. The sacro-iliac joints. The widths should be equal.
6. The region of the acetabulum. This is a complex area and fractures at this site are easy to overlook3,8–10. Compare the injured with the uninjured side.
In adolescents and young adults presenting with hip pain but no history of a violent blow also assess:

Assessing the apophyses.
Normal. The important finding is that both sides of the pelvis, and both femora, are virtually identical in appearance.There is no significant difference at any site…particularly in the region of each ASIS and AIIS (p. 215).
Common fractures, high energy
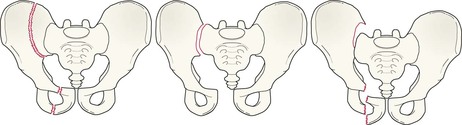
Fractures involving the main bone ring
A double break in the main pelvic ring is an unstable injury.

Sacral fractures1,11
Often very difficult to detect. The arcuate lines of the sacral foramina need to be carefully assessed, comparing one side with the other.
These fractures are overlooked in as many as 70% of cases. Many sacral fractures are undisplaced, and overlying bowel gas can also obscure these fractures. Additionally, other injuries are often present and these can distract the unwary so that the sacrum is initially overlooked.
A lateral compression force can cause a vertical compression fracture of the sacrum together with accompanying oblique fractures of the pubic rami.

Reminder: the normal sacrum.
The roof of each foramen (arrows) is smooth—no step, no irregularity.
These smooth curved roofs are often termed the “arcuate lines”.


Common fractures, low energy
Simple fall in the elderly
Fracture of a pubic ramus or pubic rami. A single fracture of the superior pubic ramus is the commonest pelvic fracture following a fall.


Injury to the coccyx
History: Fell on buttocks and the coccyx is tender. In practice the radiograph of a normal coccyx may appear angulated and very abnormal. In any case, the radiographic findings do not affect management. Radiography is unnecessary.
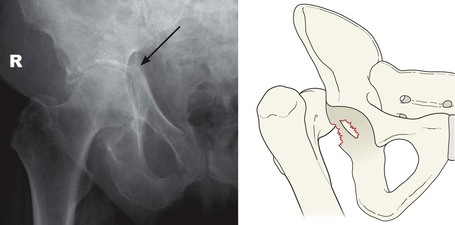
Apophyseal avulsion in the young5,7,12
These fractures are most commonly caused by repeated or sudden muscle contraction. Avulsions occur during or just after adolescence and not during childhood. Some avulsions can occur during the early 20s when fusion to the main skeleton has yet to occur (see p. 215). Very occasionally a direct blow to an apophysis rather than muscle contraction is the cause of the injury.
Recognition of an apophyseal injury on the plain radiograph will help to avoid additional unnecessary tests and/or inappropriate treatment. Treatment of these injuries is invariably conservative: rest and pain relief.
The most common sites5,7 of apophyseal avulsion are the ischial tuberosity, the ASIS, the AIIS, and the iliac crest.
Sports injuries: specific avulsions5–7
The pelvic apophyses are particularly vulnerable during numerous activities: eg soccer, American football, gymnastics, dance, jumping… ie during any activity that involves rapid acceleration or deceleration, or a sudden change of direction.
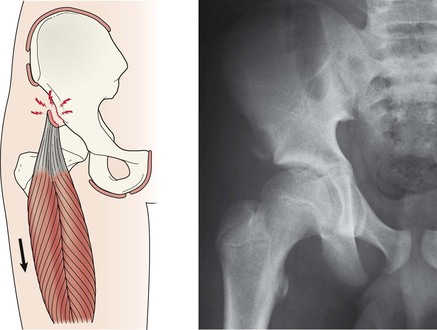
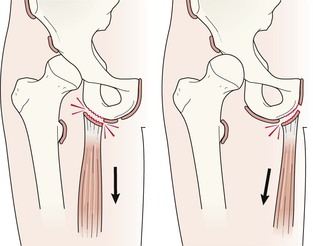
An adductor muscle avulsive injury to the apophysis at the pubic symphysis is fairly common in athletes. Radiologically the pubis on the affected side is irregular, and this can extend to involve the inferior pubic ramus.
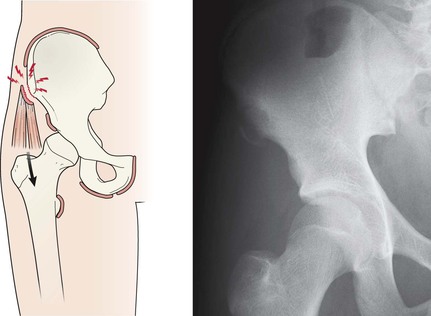
Avulsion of the lesser trochanter apophysis can occur during vigorous sports, and also when kicking.
“Hip Pointers” are contusions to the iliac crest. Contusions alone do not show major radiographic changes. Avulsion of the lateral part of this apophysis—or entire displacement—has been reported6.
Sometimes, in an athletic individual, the radiograph will show that more than one apophysis is injured.
History: young athlete with pain in the region of the ischium or the symphysis.
Suspect an apophyseal injury.


Pitfalls
In adults: Sacral fracture or sacro-illiac joint disruption may be hidden because of patient rotation or by overlying bowel gas.
In children: A normal os acetabuli or an impingement effect (see p. 226) may be misinterpreted as an acute fracture fragment.