CHAPTER 13 Patent Ductus Arteriosus
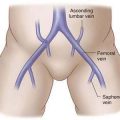
Step 1: Surgical Anatomy
Step 2: Preoperative Considerations
 Congestive heart failure in the premature infant population is the most common indication for surgical ductal closure. Whereas echocardiography may demonstrate the presence and approximate size of the patent ductus, the decision to intervene should be based on clinical symptoms of congestive heart failure (respiratory compromise caused by excessive pulmonary blood flow, failure to maintain consistent weight gain, compromise of systemic perfusion manifested as renal insufficiency, or necrotizing enterocolitis). Echocardiographic evidence of significant pulmonary volume overload, such as left atrial and left ventricular enlargement, and a chest radiograph showing cardiac enlargement and prominent pulmonary vasculature support the clinical findings.
Congestive heart failure in the premature infant population is the most common indication for surgical ductal closure. Whereas echocardiography may demonstrate the presence and approximate size of the patent ductus, the decision to intervene should be based on clinical symptoms of congestive heart failure (respiratory compromise caused by excessive pulmonary blood flow, failure to maintain consistent weight gain, compromise of systemic perfusion manifested as renal insufficiency, or necrotizing enterocolitis). Echocardiographic evidence of significant pulmonary volume overload, such as left atrial and left ventricular enlargement, and a chest radiograph showing cardiac enlargement and prominent pulmonary vasculature support the clinical findings.
 Because ductal patency is related to prostaglandin metabolism, medical closure is possible using the prostaglandin synthetase inhibitors indomethacin or other nonsteroidal anti-inflammatory drugs (NSAIDs). Only premature infants in the first week or two of life predictably respond to NSAID therapy, although the use of NSAIDs may be contraindicated because of renal insufficiency or concern about bleeding complications.
Because ductal patency is related to prostaglandin metabolism, medical closure is possible using the prostaglandin synthetase inhibitors indomethacin or other nonsteroidal anti-inflammatory drugs (NSAIDs). Only premature infants in the first week or two of life predictably respond to NSAID therapy, although the use of NSAIDs may be contraindicated because of renal insufficiency or concern about bleeding complications.


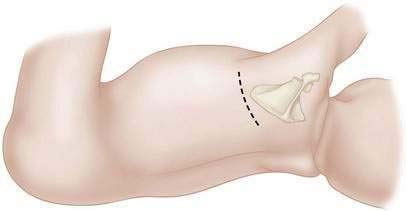
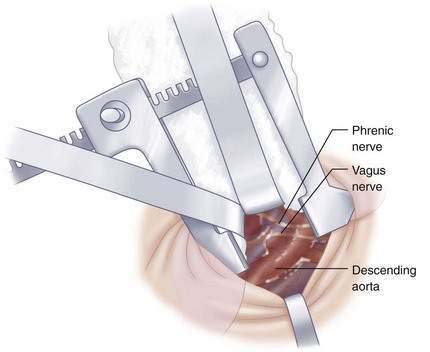
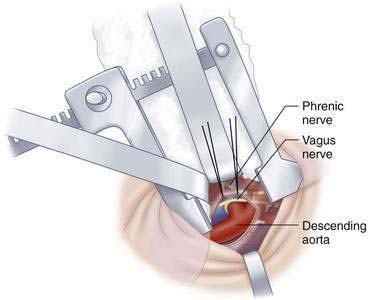
Step 3: Operative Steps




Step 4: Postoperative Care
Step 5: Pearls and Pitfalls
Gould DS, Montenegro LM, Gaynor JW, et al. A comparison of on-site and off-site patent ductus arteriosus ligation in premature infants. Pediatrics. 2003;112(6 Pt 1):1298-1301.
Hillman ND, Mavroudis C, Backer CL. Patent ductus arteriosus. In: Mavroudis C, Backer CL, editors. Pediatric cardiac surgery. 3rd ed. Philadelphia: Mosby; 2003:223-233.
Jacobs JP, Giroud JM, Quintessenza JA, et al. The modern approach to patent ductus arteriosus treatment: complementary roles of video-assisted thoracoscopic surgery and interventional cardiology coil occlusion. Ann Thorac Surg. 2003;76(5):1421-1427.
Moin F, Kennedy KA, Moya FR. Risk factors predicting vasopressor use after patent ductus arteriosus ligation. Am J Perinatol. 2003;20(6):313-320.
Rao PS. Percutaneous closure of patent ductus arteriosus: state of the art. J Invasive Cardiol. 2007;19(7):299-330.
Raval MV, Laughon MM, Bose CL, Phillips JD. Patent ductus arteriosus ligation in premature infants: who really benefits, and at what cost? J Pediatr Surg. 2007;42(1):69-75.
Schneider DJ, Moore JW. Patent ductus arteriosus. Circulation. 2006;114(17):1873-1882.
Zbar RI, Chen AH, Behrendt DM, et al. Incidence of vocal fold paralysis in infants undergoing ligation of patent ductus arteriosus. Ann Thorac Surg. 1996;61(3):814-816.