[level-membership-for-radiology-category] Antrectomy with gastroduodenostomy









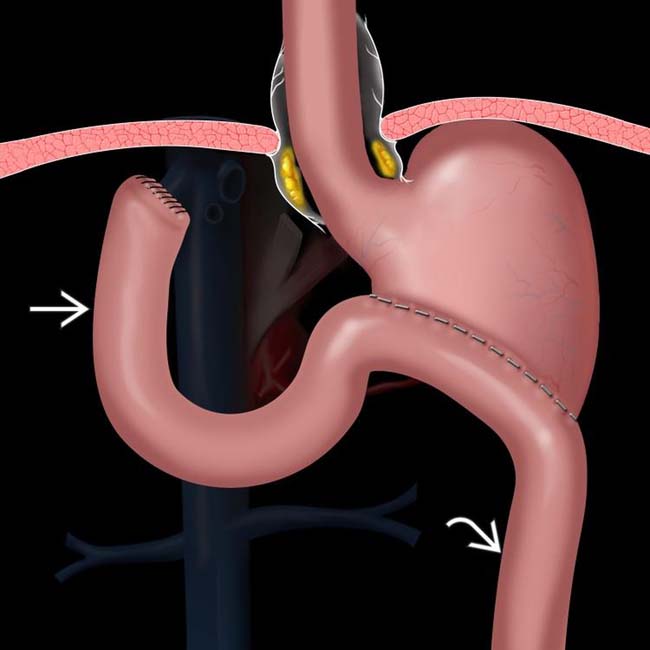
 , composed of the duodenum and a variable length of jejunum, carries pancreaticobiliary secretions toward the stomach, while the efferent limb
, composed of the duodenum and a variable length of jejunum, carries pancreaticobiliary secretions toward the stomach, while the efferent limb  carries fluid and food downstream.
carries fluid and food downstream.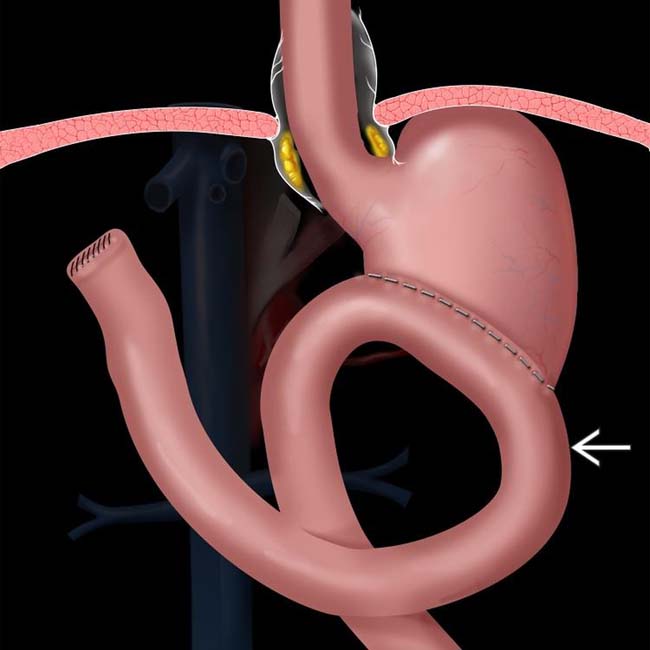
 enters the anastomosis from a left-to-right direction. This procedure is intended to reduce the prevalence of bile gastritis.
enters the anastomosis from a left-to-right direction. This procedure is intended to reduce the prevalence of bile gastritis.
 . At surgery, a phytobezoar was removed, which corresponded to the shape and size of the gastric remnant.
. At surgery, a phytobezoar was removed, which corresponded to the shape and size of the gastric remnant.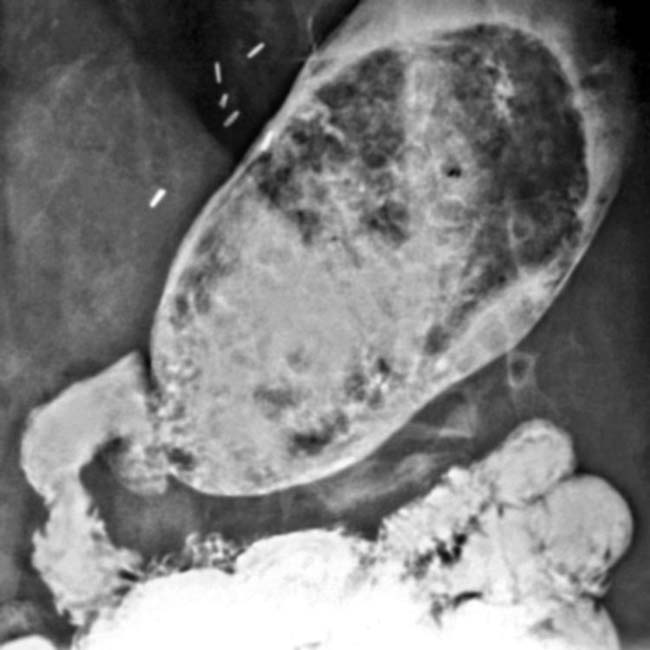
IMAGING
General Features
• Many to most fluoroscopic exams of esophagus, stomach, and duodenum are now performed for patients who have surgically altered anatomy






Surgical Procedures



• Billroth 2 (B2) procedure











Complications
• Recurrent or new carcinoma











• Anastomotic leak













































 and delayed and decreased filling of the efferent limb.
and delayed and decreased filling of the efferent limb.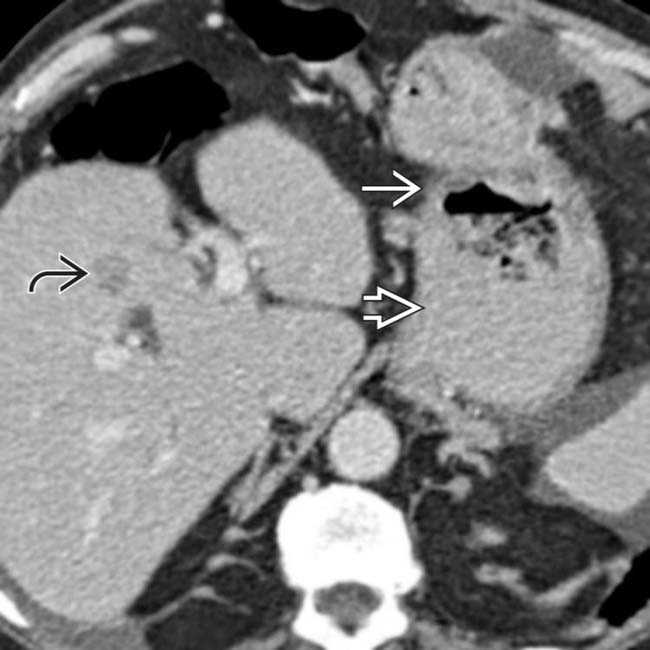
 near the gastroenteric anastomosis
near the gastroenteric anastomosis  , due to gastric carcinoma. Liver metastases are evident
, due to gastric carcinoma. Liver metastases are evident  .
.
 from lymphatic metastases.
from lymphatic metastases.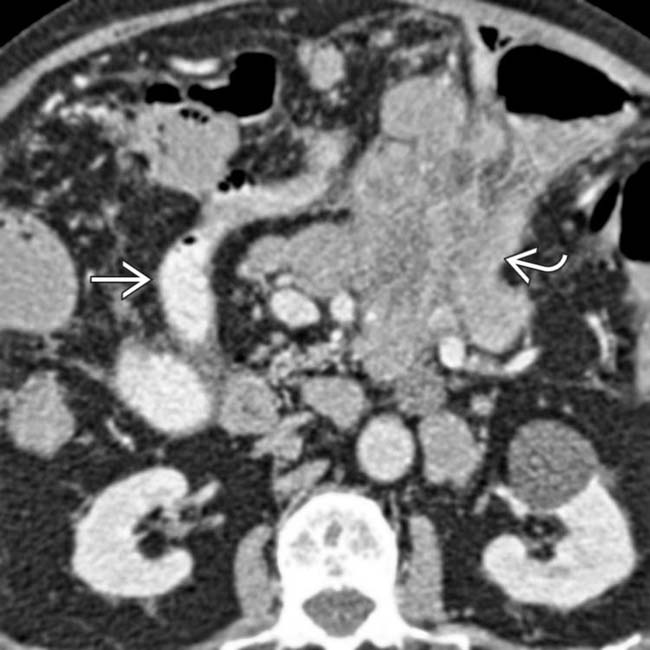
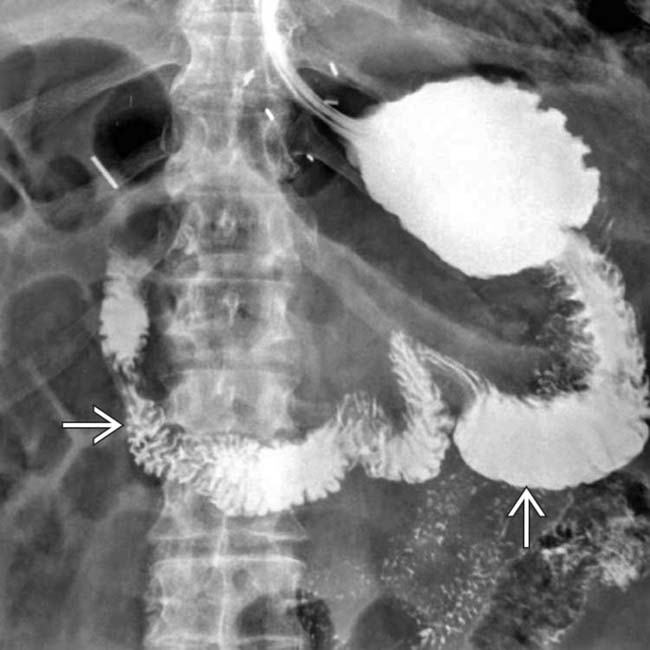
 . The contrast-filled lumen of the afferent limb is seen
. The contrast-filled lumen of the afferent limb is seen  . Gastric cancer occurs with increased frequency following this type of ulcer surgery, usually 15 or more years later.
. Gastric cancer occurs with increased frequency following this type of ulcer surgery, usually 15 or more years later.
 within the distended gastric remnant
within the distended gastric remnant  .
.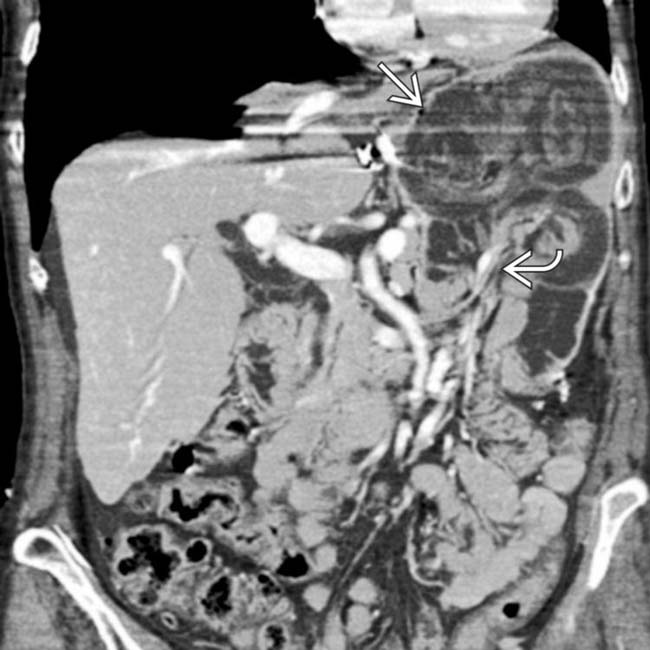
 with invagination of bowel, mesenteric fat, and vessels
with invagination of bowel, mesenteric fat, and vessels  into the gastric remnant (intussuscipiens). This is a rare complication but may result in bowel obstruction and ischemia.
into the gastric remnant (intussuscipiens). This is a rare complication but may result in bowel obstruction and ischemia.[/level-membership-for-radiology-category][not-level-membership-for-radiology-category] Antrectomy with gastroduodenostomy
, composed of the duodenum and a variable length of jejunum, carries pancreaticobiliary secretions toward the stomach, while the efferent limb carries fluid and food downstream. enters the anastomosis from a left-to-right direction. This procedure is intended to reduce the prevalence of bile gastritis.. At surgery, a phytobezoar was removed, which corresponded to the shape and size of the gastric remnant.IMAGING
General Features
• Many to most fluoroscopic exams of esophagus, stomach, and duodenum are now performed for patients who have surgically altered anatomy
Surgical Procedures
• Billroth 2 (B2) procedure
Complications
• Recurrent or new carcinoma
 Patients who have had partial gastrectomy for gastric cancer have high risk of recurrent tumor
Patients who have had partial gastrectomy for gastric cancer have high risk of recurrent tumor
Patients who have had partial gastrectomy for gastric cancer have high risk of recurrent tumor
Buy Membership for Radiology Category to continue reading. Learn more here
[/not-level-membership-for-radiology-category]
