[level-membership-for-basic-science-category]
CHAPTER 70 Pancreas
The pancreas is the largest of the digestive glands and performs a range of both endocrine and exocrine functions. The major part of the gland is exocrine, secreting a range of enzymes involved in the digestion of lipids, carbohydrates and proteins. The endocrine function of the pancreas is derived from cells scattered throughout the substance of the gland: they take part in glucose homeostasis and are also involved in the control of upper gastrointestinal motility and function.
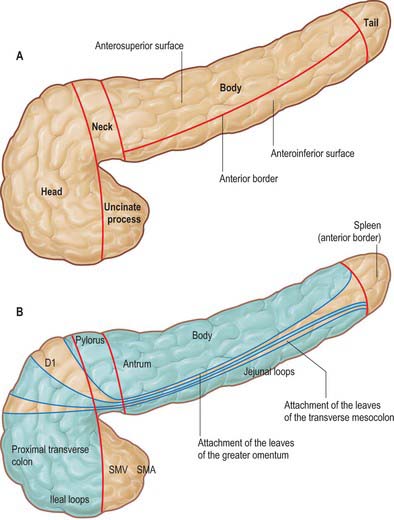
The pancreas is salmon pink in colour with a firm, lobulated smooth surface. The main portion is divided into four parts, head, neck, body and tail, purely on the basis of anatomical relations: there are only very minor functional or anatomical differences between each part (Figs 70.1 and 70.2). The pancreas also possesses one accessory lobe (the uncinate process), which is anatomically and embryologically distinct. In adults the pancreas measures between 12 and 15 cm long and is shaped as a flattened ‘tongue’ of tissue, thicker at its medial end (head) and thinner towards the lateral end (tail). With age, the amount of exocrine tissue tends to decline, as does the amount of fatty connective tissue within the substance of the gland, and this leads to a progressive thinning atrophy which is particularly noticeable on CT scanning. The pancreas lies within the curve of the first, second and third parts of the duodenum, and extends transversely and slightly upwards across the posterior abdominal wall to the hilum of the spleen, behind the stomach. It does not lie in one plane but is effectively ‘draped’ over the other structures in the retroperitoneum and the vertebral column and so forms a distinct shallow curve, of which the neck and medial body are the most anterior parts. Because of its flattened shape, the parts of the pancreas, particularly the body, are often referred to as having surfaces and borders.
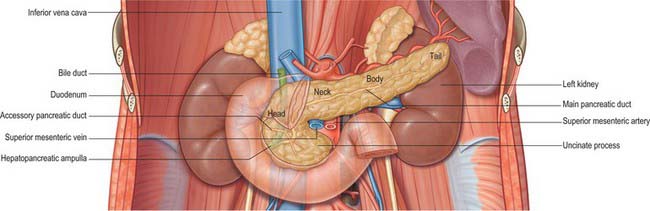

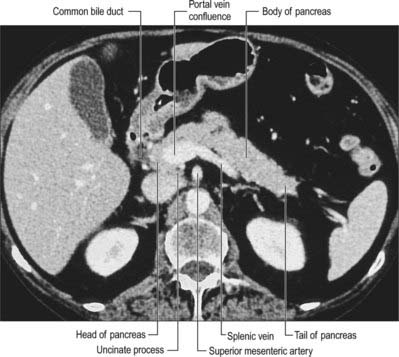
Fig. 70.2 Coronal reformat CT of the pancreas
(by courtesy of Dr Louise Moore, Chelsea and Westminster Hospital).
HEAD
The head of the pancreas lies to the right of the midline, anterior and to the right side of the vertebral column, within the curve of the duodenum. It is the thickest and broadest part of the pancreas but is still flattened in the anteroposterior plane. Superiorly it lies adjacent to the first part of the duodenum, but close to the pylorus the duodenum is on a short mesentery, and here the duodenum lies anterior to the upper part of the head. The duodenal border of the head is flattened and slightly concave, and is firmly adherent to the second part of the duodenum; occasionally a small part of the head is actually embedded in the wall of the second part of the duodenum. The superior and inferior pancreaticoduodenal arteries lie between the head and the duodenum in this area. The inferior border lies superior to the third part of the duodenum and is continuous with the uncinate process. Close to the midline, the head is continuous with the neck. The boundary between head and neck is often marked anteriorly by a groove for the gastroduodenal artery and posteriorly by a similar but deeper deep groove that contains the union of the superior mesenteric and splenic veins as they form the portal vein.
The anterior surface of the head (Fig. 70.3) is covered in peritoneum and is related to the origin of the transverse mesocolon.
NECK
The neck of the pancreas is approximately 2 cm wide and links the head and body. It is often the most anterior portion of the gland and is defined as the portion of the pancreas that lies anterior to the portal vein, which is closely related to the upper posterior surface (see Fig. 70.8). The lower part of the neck lies anterior to the superior mesenteric vein just before the formation of the portal vein. These are important relations during surgery for pancreatic cancer because malignant involvement of these vessels may make resection impossible. The anterior surface of the neck is covered with peritoneum and lies adjacent to the pylorus just inferior to the epiploic foramen. The gastroduodenal and anterior superior pancreaticoduodenal arteries descend in front of the gland in the region of the junction of the neck and head.
BODY
The anterosuperior surface of the pancreas makes up most of the anterior aspect of the gland close to the neck. Laterally, it narrows and lies slightly more superiorly to share the anterior aspect with the anteroinferior surface. It is covered by peritoneum, which runs anteroinferiorly from the surface of the gland to be continuous with the anterior, ascending layer of the greater omentum (see Fig. 64.4). The superior leaf of the transverse mesocolon is reflected and is continuous with the descending, posterior leaf of the greater omentum just above the anterior border and so forms virtually none of the covering of the anterosuperior surface. It is separated from the stomach by the lesser sac.
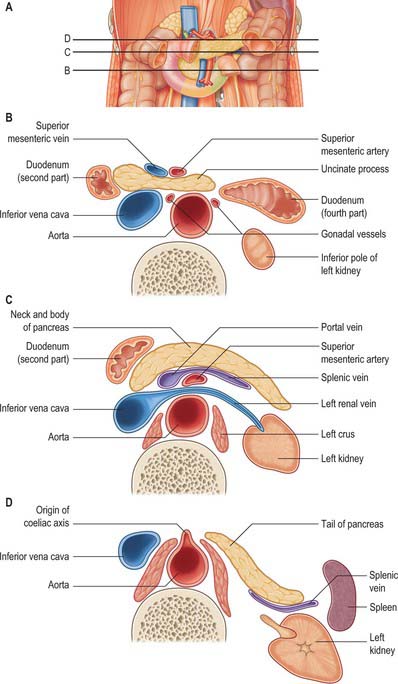
The posterior surface of the pancreas is devoid of peritoneum. It lies anterior to the aorta and the origin of the superior mesenteric artery, the left crus of the diaphragm, left suprarenal gland and the left kidney and renal vessels, particularly the left renal vein (Fig. 70.4). It is closely related to the splenic vein which lies between the posterior surface and the other posterior relations and runs from left to right forming anything from a shallow groove to a near enveloped ‘tunnel’ in the substance of the gland. The left kidney is also separated from the posterior surface by perirenal fascia and fat.
The inferior border of the pancreas separates the posterior from the anteroinferior surfaces. At the medial end of the inferior border, adjacent to the neck of the pancreas, the superior mesenteric vessels emerge from behind the gland. More laterally, the inferior mesenteric vein runs under the border to join the splenic vein on the posterior surface. This is a useful site of identification of the inferior mesenteric vein during left-sided colonic resections and on CT imaging.
UNCINATE PROCESS
The uncinate process of the pancreas extends from the inferior lateral end of the head of the gland (Fig. 70.5). Embryologically it is separate from the rest of the gland, and so it lies posterior to the superior mesenteric vein and occasionally the artery as they descend and run forward into the root of the ileal mesentery, in close contact with its anterior surface. Posteriorly it lies in front of the aorta, and inferiorly it lies on the upper surface of the third part of the duodenum. Tumours of the uncinate process do not cause obstruction to the common bile duct, but frequently compress the third part of the duodenum as a result of this close relationship.
PANCREATIC DUCTS
The exocrine pancreatic tissue drains into multiple small lobular ducts. The arrangement of the main ducts draining the pancreas is subject to some variation but the commonest arrangement is a single main and a single accessory duct (Fig. 70.6). This arrangement reflects the embryological development of the dorsal and ventral pancreatic ducts (see Ch. 73). The main duct is derived from the distal part of the dorsal duct in the body and tail but fuses with the more posteriorly placed ventral duct in the region where the dorsal bud fuses with the ventral bud (because the latter forms the posterior portion of the head of the pancreas and uncinate process). The accessory duct is the remnant of the duct of the dorsal pancreatic bud lying in the anterior pancreatic head after the principle part has joined with the ventral bud duct.
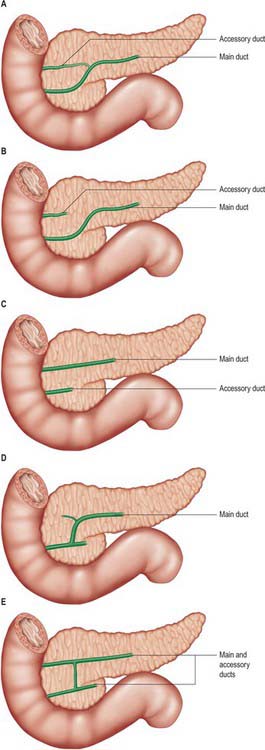
The main pancreatic duct (of Wirsung) usually runs within the substance of the gland from left to right. It tends to lie more towards the posterior than the anterior surface and is formed by the junction of several lobular (secondary) ducts in the tail. It increases in calibre as it runs within the body because it receives further lobular ducts which join it almost at right angles to its axis, forming a ‘herringbone pattern’. On ultrasound the duct can often be demonstrated, measuring approximately 3mm in diameter in the head, 2mm in the body, and 1mm in the tail in adults. As it reaches the neck of the gland it usually turns inferiorly and posteriorly towards the bile duct, which lies on its right side. The two ducts enter the wall of the descending part of the duodenum obliquely and unite in a short dilated hepatopancreatic ampulla (see Ch. 69).
The main and accessory pancreatic ducts demonstrate some variability in their anatomy reflecting variations in the development and fusion of the dorsal and ventral ducts (Fig. 70.6). One clinically important variation is ‘pancreas divisum’, where entirely separate drainage occurs for different portions of the pancreas and which may allow some forms of pancreatitis to affect only one portion of the gland.
VASCULAR SUPPLY AND LYMPHATIC DRAINAGE
Arteries
The pancreas has a rich arterial supply derived from the coeliac axis and superior mesenteric artery via both named vessels and multiple small un-named vessels (Fig. 70.7).
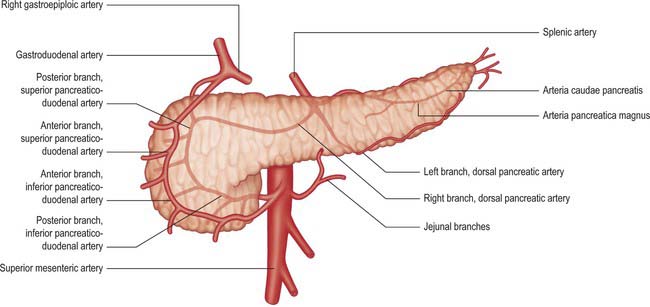
Superior pancreaticoduodenal artery
The superior pancreaticoduodenal artery is usually double. The anterior artery is a terminal branch of the gastroduodenal artery and descends in the anterior groove between the second part of the duodenum and head of the pancreas. It supplies branches to the head of the pancreas and anastomoses with the anterior division of the inferior pancreaticoduodenal artery. The posterior artery is usually a separate branch of the gastroduodenal artery arising at the upper border of the first part of the duodenum. It descends to the right, anterior to the portal vein and common bile duct, where the duct passes behind the first part of the duodenum. The artery next runs posterior to the head of the pancreas and crosses posterior to the common bile duct embedded in the head of the pancreas. It enters the duodenal wall and anastomoses with the posterior division of the inferior pancreaticoduodenal artery. The posterior superior artery supplies branches to the head of the pancreas and the first and second parts of the duodenum. (See Kimura 2000.)
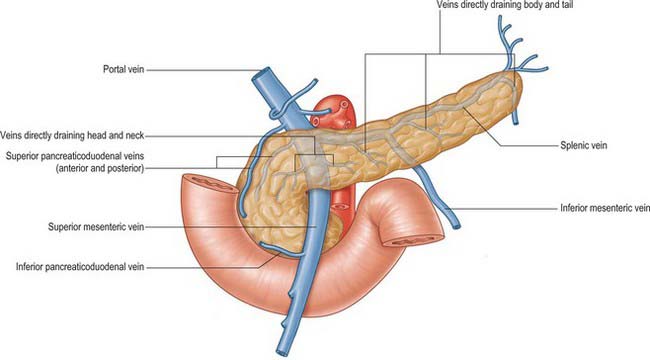
Veins
The venous drainage of the pancreas is primarily into the portal system (Fig. 70.8). The head and neck drain primarily via superior and inferior pancreaticoduodenal veins. The body and tail drain mostly via small veins that run directly into the splenic vein along the posterior aspect of the gland, or occasionally directly into the portal vein. The veins are numerous and short, features that may lead to troublesome bleeding during surgical mobilization of the head and neck of the gland. Small venous channels exist between all parts of the gland and the retroperitoneal veins, and ultimately drain into the lumbar veins: they may hypertrophy and become clinically significant in cases of portal hypertension.
Lymphatics
The lymphatic drainage of the pancreas is extensive; multiple groups of nodes may receive drainage from each region of the gland (see Fig. 65.12B) which in part explains the poor prognosis following resection of pancreatic tumours. Lymph capillaries commence around the pancreatic acini. The larger lymph vessels follow the arterial supply and drain into the lymph nodes around the pancreas and adjacent node groups. Lymphatics from the tail and body drain mostly into the pancreaticosplenic nodes, although some drain directly to pre-aortic nodes. Lymphatics from the neck and head drain more widely into nodes along the pancreaticoduodenal, superior mesenteric and hepatic arteries, and some also drain to the pre-aortic nodes and coeliac axis nodes. There is no evidence of lymphatic channels within the pancreatic islets.
PANCREATITIS AND PSEUDOCYST
In acute episodes, the profuse arterial and venous supply to the gland makes it particularly prone to haemorrhage. The extravasated blood collects in the retroperitoneal tissues because the neck and body of the gland lie largely in the loose connective tissue of the retroperitoneum. The pancreas lies anterior to the thoracolumbar and perirenal fasciae and the blood-stained fluid can track freely in the retroperitoneal tissues to appear in either the flanks (Grey–Turner’s sign), groins, or above the iliac crest where the iliac fascia is attached. Blood-stained fluid tracking laterally from the head of the pancreas may enter the lesser omentum and the ‘bare area’ of the liver, from where it may run forward into the falciform ligament and appear around the skin of the umbilicus (Cullen’s sign).
MICROSTRUCTURE
The pancreas is composed of two different types of glandular tissue. The main tissue mass is exocrine, in which pancreatic islets of endocrine cells are embedded (Figs 70.9–70.11).
Exocrine pancreas
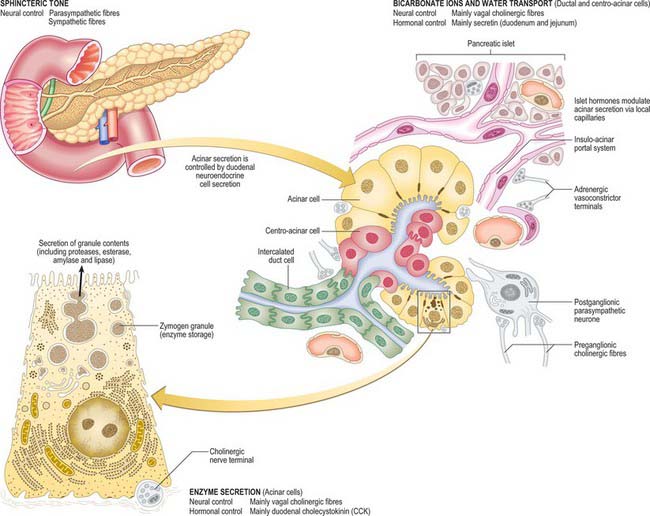
The exocrine pancreas isa branched acinar gland, surrounded and incompletely lobulated by delicate loose connective tissue. It is formed of pyramidal, secretory cells arranged mainly as spherical clusters, or acini. A narrow intercalated, intralobular duct originates within each secretory acinus, lined initially by flattened or cuboidal centro-acinar cells. These small ductules form branching links which run within and between adjacent acini, explaining why structurally distinct intralobular pancreatic ducts are infrequent (see Kerr 1999, for details). More distally, these are replaced by taller cuboidal and eventually columnar epithelium in the larger interlobular ducts. The latter are surrounded by loose connective tissue of the septa, containing smooth muscle and autonomic nerve fibres. Neuroendocrine cells are present amongst the columnar ductal cells and mast cells are numerous in the surrounding connective tissue.
Acinar cells of the exocrine pancreas have a basal nucleus and, in their basal cytoplasmic domain, abundant rough endoplasmic reticulum which results in their basophilic staining characteristics. Dense secretory zymogen granules stain deeply with eosin in the apical region. A prominent supranuclear Golgi complex is surrounded by large, membrane-bound granules containing the proteinaceous constituents of pancreatic secretion, including enzymes which are only active after release. Ganglionic neurones and cords of undifferentiated epithelial cells are also found within the acini. The structure of the exocrine pancreas and its functional regulation are summarized in Fig. 70.9.
Pancreatic stellate cells, PaSCs, are one of several resident cells in the exocrine pancreas. They are regulated by autocrine and paracrine stimuli and share many features with their hepatic counterparts. PaSCs are myofibroblast-like cells and are found in the periacinar space, where their long cytoplasmic processes encircle the base of the acinus, and in perivascular and periductal regions of the pancreas. They have been implicated as key players in the pathobiology of the major disorders of the exocrine pancreas, including chronic pancreatitis and pancreatic cancer (Bishr Omary et al 2007).
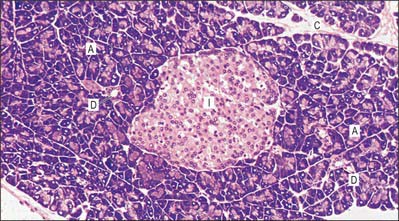
Endocrine pancreas
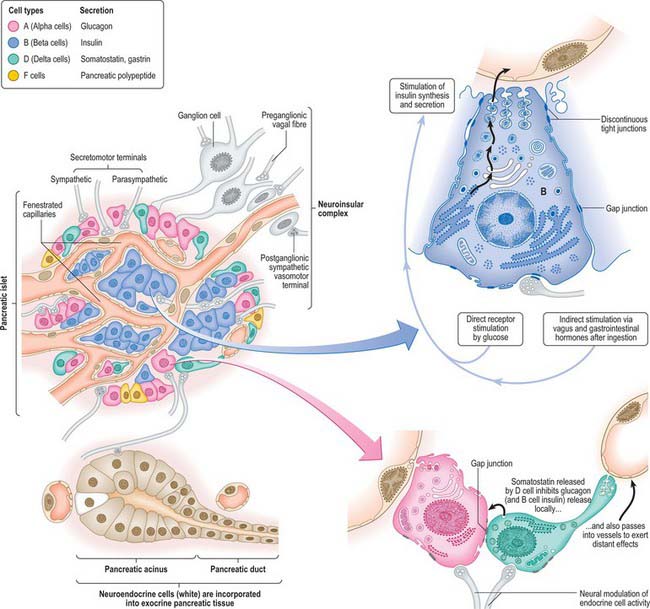
The endocrine pancreas consists of pancreatic islets of Langerhans, composed of spherical or ellipsoid clusters of cells embedded in the exocrine tissue. The human pancreas may contain more than a million islets, usually most numerous in the tail. An islet is a mass of polyhedral cells, each in close proximity to fenestrated capillaries and a rich autonomic innervation. Specialized staining procedures or immunohistochemical techniques are necessary to distinguish the three major types of cell, designated alpha, beta and delta. Their general organization is shown in Fig. 70.11.
Innervation of endocrine pancreas
The innervation of the endocrine islets is almost exclusively from the parasympathetic system. Fine branches ramify among the cells and form plexuses around the islets. Fibres frequently synapse with acinar cells before innervating the islets, suggesting a close linkage between neural control of exocrine and endocrine components. Many fibres enter the islets with the arterioles. Parasympathetic ganglia lie in the connective tissue within and between lobules, and in the former case are frequently associated with islet cells, forming neuroinsular complexes. Both alpha and beta cells are involved in these neuroinsular complexes. Three types of nerve terminal are seen in islets. Cholinergic terminals have agranular vesicles with a diameter of 30–50 nm, adrenergic terminals have dense-cored vesicles with a diameter of 30–50 nm and a third, uncharacterized, type have dense-cored vesicles with a diameter of 60–200 nm (Smith & Porte 1976).
No selective link with any one type of insular cell has been found. Sometimes more than one type of terminal contacts a single cell and some of the chemical synapses between axon terminals and islet cells show narrow areas in the synaptic clefts suggesting an electrical synapse or gap junction. Such junctions also occur between islet cells, and electrical coupling of nerve supply to a functional network of islet cells may occur (Orci 1974).
Bishr Omary M, Lugea A, Lowe AW, Pandol SJ. The pancreatic stellate cell: a star on the rise in pancreatic diseases. J Clin Invest. 2007;117:50-59.
Kerr JB. Atlas of Functional Histology, Chapter 14. London: Mosby, 1999.
Kimura W. Surgical anatomy of the pancreas for limited resection. J Hepatobiliary Pancreat Surg. 2000;7:473-479.
Nagai H. Configurational anatomy of the pancreas: its surgical relevance from ontogenetic and comparative-anatomical viewpoints. J Hepatobiliary Pancreat Surg. 2003;10:48-56.
Orci L. A portrait of a pancreatic B-cell. Diabetologia. 1974;10:163-187.
Smith PH, Porte DJr. Neuropharmacology of the pancreatic islets. Annu Rev Pharmacol Toxicol. 1976;16:269-285.
[/level-membership-for-basic-science-category][not-level-membership-for-basic-science-category]
CHAPTER 70 Pancreas
The pancreas is the largest of the digestive glands and performs a range of both endocrine and exocrine functions. The major part of the gland is exocrine, secreting a range of enzymes involved in the digestion of lipids, carbohydrates and proteins. The endocrine function of the pancreas is derived from cells scattered throughout the substance of the gland: they take part in glucose homeostasis and are also involved in the control of upper gastrointestinal motility and function.
The pancreas is salmon pink in colour with a firm, lobulated smooth surface. The main portion is divided into four parts, head, neck, body and tail, purely on the basis of anatomical relations: there are only very minor functional or anatomical differences between each part (Figs 70.1 and 70.2). The pancreas also possesses one accessory lobe (the uncinate process), which is anatomically and embryologically distinct. In adults the pancreas measures between 12 and 15 cm long and is shaped as a flattened ‘tongue’ of tissue, thicker at its medial end (head) and thinner towards the lateral end (tail). With age, the amount of exocrine tissue tends to decline, as does the amount of fatty connective tissue within the substance of the gland, and this leads to a progressive thinning atrophy which is particularly noticeable on CT scanning. The pancreas lies within the curve of the first, second and third parts of the duodenum, and extends transversely and slightly upwards across the posterior abdominal wall to the hilum of the spleen, behind the stomach. It does not lie in one plane but is effectively ‘draped’ over the other structures in the retroperitoneum and the vertebral column and so forms a distinct shallow curve, of which the neck and medial body are the most anterior parts. Because of its flattened shape, the parts of the pancreas, particularly the body, are often referred to as having surfaces and borders.
Fig. 70.2 Coronal reformat CT of the pancreas
(by courtesy of Dr Louise Moore, Chelsea and Westminster Hospital).
HEAD
The head of the pancreas lies to the right of the midline, anterior and to the right side of the vertebral column, within the curve of the duodenum. It is the thickest and broadest part of the pancreas but is still flattened in the anteroposterior plane. Superiorly it lies adjacent to the first part of the duodenum, but close to the pylorus the duodenum is on a short mesentery, and here the duodenum lies anterior to the upper part of the head. The duodenal border of the head is flattened and slightly concave, and is firmly adherent to the second part of the duodenum; occasionally a small part of the head is actually embedded in the wall of the second part of the duodenum. The superior and inferior pancreaticoduodenal arteries lie between the head and the duodenum in this area. The inferior border lies superior to the third part of the duodenum and is continuous with the uncinate process. Close to the midline, the head is continuous with the neck. The boundary between head and neck is often marked anteriorly by a groove for the gastroduodenal artery and posteriorly by a similar but deeper deep groove that contains the union of the superior mesenteric and splenic veins as they form the portal vein.
The anterior surface of the head (Fig. 70.3) is covered in peritoneum and is related to the origin of the transverse mesocolon.
NECK
The neck of the pancreas is approximately 2 cm wide and links the head and body. It is often the most anterior portion of the gland and is defined as the portion of the pancreas that lies anterior to the portal vein, which is closely related to the upper posterior surface (see Fig. 70.8). The lower part of the neck lies anterior to the superior mesenteric vein just before the formation of the portal vein. These are important relations during surgery for pancreatic cancer because malignant involvement of these vessels may make resection impossible. The anterior surface of the neck is covered with peritoneum and lies adjacent to the pylorus just inferior to the epiploic foramen. The gastroduodenal and anterior superior pancreaticoduodenal arteries descend in front of the gland in the region of the junction of the neck and head.
BODY
The anterosuperior surface of the pancreas makes up most of the anterior aspect of the gland close to the neck. Laterally, it narrows and lies slightly more superiorly to share the anterior aspect with the anteroinferior surface. It is covered by peritoneum, which runs anteroinferiorly from the surface of the gland to be continuous with the anterior, ascending layer of the greater omentum (see Fig. 64.4). The superior leaf of the transverse mesocolon is reflected and is continuous with the descending, posterior leaf of the greater omentum just above the anterior border and so forms virtually none of the covering of the anterosuperior surface. It is separated from the stomach by the lesser sac.
The posterior surface of the pancreas is devoid of peritoneum. It lies anterior to the aorta and the origin of the superior mesenteric artery, the left crus of the diaphragm, left suprarenal gland and the left kidney and renal vessels, particularly the left renal vein (Fig. 70.4). It is closely related to the splenic vein which lies between the posterior surface and the other posterior relations and runs from left to right forming anything from a shallow groove to a near enveloped ‘tunnel’ in the substance of the gland. The left kidney is also separated from the posterior surface by perirenal fascia and fat.
The inferior border of the pancreas separates the posterior from the anteroinferior surfaces. At the medial end of the inferior border, adjacent to the neck of the pancreas, the superior mesenteric vessels emerge from behind the gland. More laterally, the inferior mesenteric vein runs under the border to join the splenic vein on the posterior surface. This is a useful site of identification of the inferior mesenteric vein during left-sided colonic resections and on CT imaging.
