[level-membership-for-internal-medicine-category]
Chapter 10 Palliative medicine and symptom control
Introduction and general aspects
Palliative care is the active total care of patients who have advanced, progressive life-shortening disease. It is now recognized that palliative care should be based on needs not diagnosis: it is needed in many non-malignant diseases as well as in cancer (Box 10.1).
 Box 10.1
Box 10.1
Key components of a modern palliative care service
 Management should be based on needs not diagnosis: the symptom burden of non-malignant disease often equals that of cancer
Management should be based on needs not diagnosis: the symptom burden of non-malignant disease often equals that of cancer

 Rehabilitation for people with advanced disease
Rehabilitation for people with advanced disease

 Bereavement care for people with pathological grief problems
Bereavement care for people with pathological grief problems
 Telephone advice for other clinicians; disseminating palliative care knowledge
Telephone advice for other clinicians; disseminating palliative care knowledge
 Teaching for clinicians, from undergraduate level to postgraduate life-long learning
Teaching for clinicians, from undergraduate level to postgraduate life-long learning
Importance of early assessment
If palliative care is seen only as relevant for the end-of-life phase, patients who have non-malignant disease are denied expert help for complex symptoms. Timely management of physical and psychosocial issues earlier in the course of disease prevents intractable problems later (Box 10.2).
 Box 10.2
Box 10.2
Problems arising when specialist palliative care (SPC) is delayed until the end-of-life




Symptom control
This section outlines the medical aspects of symptom control. Good palliative care integrates these with appropriate non-pharmacological approaches, including anxiety management and rehabilitation (see p. 489).
Pain
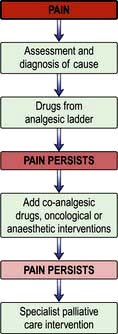
Pain is a feared symptom in cancer and at least two-thirds of people with cancer suffer significant pain. Pain has a number of causes, and not all pains respond equally well to opioid analgesics (Fig. 10.1). The pain is either related directly to the tumour (e.g. pressure on a nerve) or indirectly, for example due to weight loss or pressure sores. It may result from a co-morbidity such as arthritis. Emotional and spiritual distress may be expressed as physical pain (termed ‘opioid irrelevant pain’) or will exacerbate physical pain.
The term ‘total pain’ encompasses a variety of influences that contribute to pain:
 Biological: the cancer itself, cancer therapy (drugs, surgery, radiotherapy)
Biological: the cancer itself, cancer therapy (drugs, surgery, radiotherapy)
 Social: family distress, loss of independence, financial problems from job loss
Social: family distress, loss of independence, financial problems from job loss

 Spiritual: fear of death, questions about life’s meaning, guilt.
Spiritual: fear of death, questions about life’s meaning, guilt.
The WHO analgesic ladder
Most cancer pain can be managed with oral or commonly used transdermal preparations. The World Health Organization (WHO) cancer pain relief ladder guides the choice of analgesic according to pain severity (Fig. 10.2, Table 10.1).
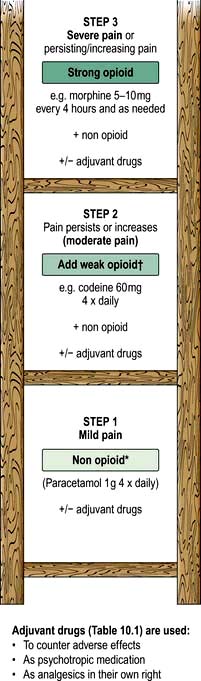
Figure 10.2 WHO analgesic ladder for cancer and other chronic pain. Step 2 can be omitted, going to morphine immediately. Adjuvant drugs are listed in Table 10.1. *Opioids include all drugs with an action similar to morphine, i.e. binding to endogenous opioid receptors. †Continue NSAID/paracetamol regularly when opioid started.
| Drugs | Indication |
|---|---|
|
NSAIDs, e.g. diclofenac |
Bone pain, inflammatory pain |
|
Anticonvulsants, e.g. gabapentin (600–2400 mg daily) or pregabalin (150 mg at start increasing up to 600 mg daily) |
Neuropathic pain |
|
Tricyclic antidepressants, e.g. amitriptyline (10–75 mg daily) |
Neuropathic pain |
|
Bisphosphonates, e.g. disodium pamidronate |
Metastatic bone disease |
|
Dexamethasone |
Neuropathic pain, inflammatory pain (e.g. liver capsule pain), headache from cerebral oedema due to brain tumour |
If regular use of optimum dosing (e.g. paracetamol 1 g × 4 daily for step 1) does not control the pain, then an analgesic from the next step of the ladder is prescribed. As pain is due to different physical aetiologies, an adjuvant analgesic may be needed in addition or instead, such as the tricyclic antidepressant amitriptyline for neuropathic pain (Table 10.1).
Strong opioid drugs




Side-effects
The most common side-effects are:
 Nausea and vomiting: this can usually be managed or prevented with antiemetics (such as metoclopramide). Some antiemetics can be combined with an opioid, e.g. haloperidol or metoclopramide; always check compatibility data.
Nausea and vomiting: this can usually be managed or prevented with antiemetics (such as metoclopramide). Some antiemetics can be combined with an opioid, e.g. haloperidol or metoclopramide; always check compatibility data.

If side-effects are intractable, a change of opioid is often helpful.
Gastrointestinal symptoms
Respiratory symptoms
Breathlessness
Breathlessness remains one of the most distressing and common symptoms in palliative care; causing the patient serious discomfort, it is highly distressing for carers to witness. Full assessment and active treatment of all reversible conditions, such as drainage of pleural effusions, or optimization of treatment of heart failure or chronic pulmonary disease is mandatory. In advanced cancer, breathlessness is often multifactorial in origin and many of the contributory factors are irreversible (e.g. cachexia), so a ‘complex intervention’ combining a number of different treatment strategies has the greatest impact. Aspects of breathlessness management are summarized in Box 10.3.
 Box 10.3
Box 10.3
Key points for successful management of breathlessness
 Start treatment early: patients who are likely to develop breathlessness should learn non-pharmacological approaches early in the disease course, before breathlessness has become severe.
Start treatment early: patients who are likely to develop breathlessness should learn non-pharmacological approaches early in the disease course, before breathlessness has become severe.

 Ensure management is rehabilitative (see p. 489): this increases physical fitness, hope, self-efficacy, and may enable patient and carer to achieve goals that once seemed impossible.
Ensure management is rehabilitative (see p. 489): this increases physical fitness, hope, self-efficacy, and may enable patient and carer to achieve goals that once seemed impossible.
 Integrate psychological, physical and social interventions, as with all palliative care.
Integrate psychological, physical and social interventions, as with all palliative care.
Breathlessness with panic and anxiety
Using a hand-held fan to alleviate breathlessness. For more on interventions for breathlessness, see http://www.cuh.org.uk/breathlessness.
Non-pharmacological approaches such as using a hand-held fan, pacing, prioritizing activities to avoid over-exertion, breathing training and anxiety management are helpful (Table 10.2). There is no evidence to suggest that oxygen therapy reduces the sensation of breathlessness in advanced disease and the hand-held fan should be used before oxygen for this purpose. Opioids, used orally or parenterally, can palliate breathlessness. If panic/anxiety is significant, a quick-acting benzodiazepine such as lorazepam (used sublingually for rapid absorption) may be useful.
Table 10.2 Key non-pharmacological interventions for breathlessness
| Intervention | Putative mechanism of action | Most useful |
|---|---|---|
|
Hand-held fan |
Cooling area served by 2nd and 3rd branches of trigeminal nerve |
Reducing length of episodes of SOB on exertion or at rest |
|
Reduces temperature of air flowing over nasal receptors, altering signal to brainstem respiratory complex and so changing respiratory pattern |
Gives patient and carer confidence to have an intervention they can use |
|
|
Exercise |
Stops spiral of disability developing |
Patients who are still quite mobile. |
|
Changes muscle structure: less lactic acid produced |
In patients who have not developed onset of SOB, reduce/defer symptoms by reducing deconditioning |
|
|
Anxiety reduction, e.g. CBT (needs skilled clinician to administer) or simple relaxation therapy |
Works on central perception of breathlessness reducing impact |
People with higher levels of anxiety at baseline (i.e. when first seen) |
|
Interrupting panic/anxiety cycle |
Patients willing to persevere with learning a new skill |
|
|
Carer support |
Reduces carer anxiety and distress which is part of ‘total’ anxiety–panic cycle |
Where carer is isolated, under extra pressures (e.g. looking after elderly parent, going through divorce) |
|
Breathing retraining |
Improve mechanical effectiveness respiratory system |
Chronic advanced respiratory disease and those with anxiety-related breathlessness |
|
Pacing (finding a balance between activity and rest to achieve aims) and prioritizing (deciding which daily activities are most necessary and focusing energy use on them) |
Avoids over-exertion which can lead to exhaustion, inactivity and subsequent deconditioning |
Patients who are able and willing to modify daily routines |
|
Neuromuscular electrical stimulation |
Increases muscle bulk, simulating effect of exercise |
Patients who live alone |
|
Those unable to get out to attend rehabilitation group |
||
|
People with a short prognosis |
||
|
People with co-morbidities that prevent exercise |
CBT, cognitive behavioural therapy; SOB, short of breath (breathlessness).
Other physical symptoms
Fatigue


Loss of function, disability and rehabilitation



Extending palliative care to people with non-malignant disease
The principles of palliative care can be applied throughout medical practice so that all patients, irrespective of care setting (home, hospital or hospice) receive appropriate care from the staff looking after them and have access to SPC services for complex issues. Some principles are outlined in Box 10.4. Patients who have chronic non-malignant disease such as organ failures (heart, lung and kidney), degenerative neurological disease and HIV infection:
 have a similar or greater symptom burden than people with cancer
have a similar or greater symptom burden than people with cancer
 may live longer with these difficulties
may live longer with these difficulties
 benefit from a palliative care approach with access to SPC for complex problems.
benefit from a palliative care approach with access to SPC for complex problems.
 Box 10.4
Box 10.4
Key points in palliative care






Patients who have non-malignant disease may have very close relationships with their usual team, and an integrated approach is essential to allow optimization of disease-directed medication as well as palliation. People with non-malignant disease may live for years with a difficult illness and so their palliative care needs to differ in some respects from those of cancer patients (Table 10.3). However, symptom management is largely transferable, with some exceptions and extra complexities as outlined below.
Table 10.3 Differences between palliative care for people with malignant and non-malignant diseases
| Cancer | Non-malignant disease |
|---|---|
|
Standard treatment regimens even in advanced disease |
Advanced disease often needs bespoke pharmacological interventions, which may interact with palliative drugs. Close teamwork is essential to avoid adversely affecting outcomes, e.g. in use of opioids and many other drugs |
|
Relatively new diagnosis (weeks to months) |
Usually many years of illness with loss of social networks, employment and practical support |
|
Sudden death is rare (although it can happen, e.g. pulmonary embolus, neutropenic sepsis) |
Sudden death is relatively frequent as a result of cardiovascular/diabetic complications (e.g. in chronic kidney disease) |
|
Cancer and associated problems are the main morbidities |
Co-morbidities due to disease or treatment often cause most problems and shape end-of-life care |
|
Prognosis is usually predictable |
Prognosis difficult to determine: many ‘near death experiences’, admissions and recoveries occur |
|
Support from SPC services is often started early in the disease course |
Main support may be from a medical unit, e.g. dialysis unit |
|
Standard hospice services (e.g. day therapy) often suit treatment patterns well |
Standard hospice service may not be offered (clinician ignorance) or may not be feasible (e.g. for dialysis patient attending hospital 3 days a week) |
Heart failure
There are special considerations with respect to cardiac medication in advanced disease:




Chronic respiratory disease
Chronic obstructive pulmonary disease (COPD)
Because of the risk of dependency, falls and memory problems, non-pharmacological approaches to anxiety are more appropriate than benzodiazepines (Table 10.2). Short-acting benzodiazepines should be reserved for severe panic episodes.
Other chronic respiratory diseases
Other chronic respiratory illnesses that often require palliative care include:
 Diffuse parenchymal lung disorders (interstitial lung disease) (ILD): this has a trajectory similar to cancer with rapidly developing breathlessness and cough. The breathlessness of ILD is particularly frightening but may respond well to opioids: early access to hospice services is particularly relevant to help with symptom control and anxiety.
Diffuse parenchymal lung disorders (interstitial lung disease) (ILD): this has a trajectory similar to cancer with rapidly developing breathlessness and cough. The breathlessness of ILD is particularly frightening but may respond well to opioids: early access to hospice services is particularly relevant to help with symptom control and anxiety.


Renal disease


Neurological disease


Motor neurone disease
Motor neurone disease is usually rapidly progressive, often requiring hospice support. Percutaneous endoscopic gastrostomy (p. 222) feeding may be required. In addition, if ventilatory failure develops, nocturnal non-invasive ventilation may be offered. Patients and their carers need to understand:




Care of the dying
FURTHER READING
Department of Health. End of Life Care Strategy: promoting high quality care for all adults at the end of life. London: Department of Health; 2008:16 July.
General Medical Council. Treatment and Care Towards the End of Life: good practice in decision making. London: General Medical Council; 2010.
Marie Curie Palliative Care Institute Liverpool (MCPCIL) in collaboration with the Clinical Standards Department of the Royal College of Physicians (RCP). National Care of the Dying Audit – Hospitals (NCDAH) Round 2, 2008–9. Supported by the Marie Curie Cancer Care and the Department of Health End of Life Care Programme; 2009.
Do not attempt resuscitation (DNAR) orders
• The resuscitation status of every patient should be discussed by senior doctors at the time of admission and the decision documented in the notes.
• Many hospitals have specific DNAR forms. Deciding a person’s resuscitation status is a careful balance of risk versus benfit. The patient’s co-morbidities and pre-morbid quality of life should be taken into account.
• Involve the patient and family in this discussion, and explain the medical reasoning behind the decision. If the patient requests that CPR is not performed in the event of cardio-pulmonary arrest, those wishes should be respected.
An end-of-life tool: the Liverpool Care Pathway
The Liverpool Care Pathway (LCP) is a four-stage end-of-life tool designed to transfer the standard of hospice care of the dying into the hospital (Box 10.5). Now adapted for any setting, it is the most commonly used pathway for care of the dying in the UK and in several other countries. There have been no trials comparing effectiveness of any end-of-life care pathways against usual care without a pathway, but serial UK national hospital audits have been able to assess and monitor the level of care documented against the standards set in the LCP.
 Box 10.5
Box 10.5



BNF. Guidance on prescribing: prescribing in palliative care. British National Formulary. London: BMJ Group and RPS Publishing http://bnf.org/bnf/bnf/current
Goldstein NE, Fischberg D. Update in palliative medicine. Ann Intern Med. 2008;148:135–140.
Twycross R, Wilcock A. Palliative Care Formulary, 4th edn. Nottingham: Palliativebooks.com; 2011.
[/level-membership-for-internal-medicine-category][not-level-membership-for-internal-medicine-category]
Chapter 10 Palliative medicine and symptom control
Introduction and general aspects
Palliative care is the active total care of patients who have advanced, progressive life-shortening disease. It is now recognized that palliative care should be based on needs not diagnosis: it is needed in many non-malignant diseases as well as in cancer (Box 10.1).
Box 10.1
Key components of a modern palliative care service
Management should be based on needs not diagnosis: the symptom burden of non-malignant disease often equals that of cancer
Rehabilitation for people with advanced disease
Bereavement care for people with pathological grief problems
Telephone advice for other clinicians; disseminating palliative care knowledge
Teaching for clinicians, from undergraduate level to postgraduate life-long learning
Importance of early assessment
If palliative care is seen only as relevant for the end-of-life phase, patients who have non-malignant disease are denied expert help for complex symptoms. Timely management of physical and psychosocial issues earlier in the course of disease prevents intractable problems later (Box 10.2).
Box 10.2
Problems arising when specialist palliative care (SPC) is delayed until the end-of-life
Symptom control
This section outlines the medical aspects of symptom control. Good palliative care integrates these with appropriate non-pharmacological approaches, including anxiety management and rehabilitation (see p. 489).
Pain
Pain is a feared symptom in cancer and at least two-thirds of people with cancer suffer significant pain. Pain has a number of causes, and not all pains respond equally well to opioid analgesics (Fig. 10.1). The pain is either related directly to the tumour (e.g. pressure on a nerve) or indirectly, for example due to weight loss or pressure sores. It may result from a co-morbidity such as arthritis. Emotional and spiritual distress may be expressed as physical pain (termed ‘opioid irrelevant pain’) or will exacerbate physical pain.
The term ‘total pain’ encompasses a variety of influences that contribute to pain:
Biological: the cancer itself, cancer therapy (drugs, surgery, radiotherapy)
Social: family distress, loss of independence, financial problems from job loss
Spiritual: fear of death, questions about life’s meaning, guilt.
The WHO analgesic ladder
Most cancer pain can be managed with oral or commonly used transdermal preparations. The World Health Organization (WHO) cancer pain relief ladder guides the choice of analgesic according to pain severity (Fig. 10.2, Table 10.1).
Figure 10.2 WHO analgesic ladder for cancer and other chronic pain. Step 2 can be omitted, going to morphine immediately. Adjuvant drugs are listed in Table 10.1. *Opioids include all drugs with an action similar to morphine, i.e. binding to endogenous opioid receptors. †Continue NSAID/paracetamol regularly when opioid started.
| Drugs | Indication |
|---|---|
|
NSAIDs, e.g. diclofenac |
Bone pain, inflammatory pain |
|
Anticonvulsants, e.g. gabapentin (600–2400 mg daily) or pregabalin (150 mg at start increasing up to 600 mg daily) |
Neuropathic pain |
|
Tricyclic antidepressants, e.g. amitriptyline (10–75 mg daily) |
Neuropathic pain |
|
Bisphosphonates, e.g. disodium pamidronate |
Metastatic bone disease |
|
Dexamethasone |
Neuropathic pain, inflammatory pain (e.g. liver capsule pain), headache from cerebral oedema due to brain tumour |
If regular use of optimum dosing (e.g. paracetamol 1 g × 4 daily for step 1) does not control the pain, then an analgesic from the next step of the ladder is prescribed. As pain is due to different physical aetiologies, an adjuvant analgesic may be needed in addition or instead, such as the tricyclic antidepressant amitriptyline for neuropathic pain (Table 10.1).
Strong opioid drugs
Side-effects
The most common side-effects are:
Nausea and vomiting: this can usually be managed or prevented with antiemetics (such as metoclopramide). Some antiemetics can be combined with an opioid, e.g. haloperidol or metoclopramide; always check compatibility data.
If side-effects are intractable, a change of opioid is often helpful.
