Leg Pain
This section deals with causes of pain arising from local lesions within the leg, or referred into the leg. Pain in the leg is a common complaint and the majority of cases are of vascular or orthopaedic origin. Joint problems are dealt with in the section on Joint disorders (p. 267).
History
Traumatic
Obvious history of trauma.
Inflammatory
History of joint swelling, stiffness, limitation of movement. Pain on walking. There may be an obvious history of rheumatoid arthritis with signs elsewhere, e.g. the hands. Reiter’s disease – conjunctivitis, urethritis. Ankylosing spondylitis – stiffness of the spine, especially in the morning; hip and knee involvement.
Infective
Cellulitis may arise from puncture wounds, e.g. insect bites or in a lymphoedematous leg. The patient presents with pain, redness, tenderness, malaise and fever. Myositis may occur in association with collagen diseases, e.g. scleroderma, dermatomyositis. Osteomyelitis is rare but more common in childhood. History of immunosuppression or diabetes. Recent history of infection elsewhere. Pain aggravated by movement. Swelling and redness of the affected area. Septic arthritis presents with a red, hot, tender, painful joint. More common in children. In adults, enquire about a history of steroid therapy or diabetes.
Degenerative
Osteoarthritis presents with pain, stiffness and deformity. The pain is often worse on starting walking and then improves. Baker’s cyst presents with a lump behind the knee. The patient may complain of pain and swelling of the calf if the cyst ruptures. With meniscal lesions, there is usually a history of twisting the knee, e.g. playing football. The knee may lock.
Vascular
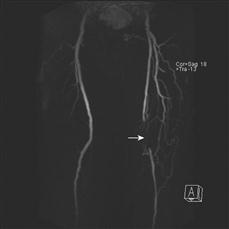
Deep venous thrombosis presents with painful swelling of the leg. There may be a history of the contraceptive pill, prolonged immobilisation, recent surgery, malignancy. Acute arterial occlusion results in sudden onset of severe pain in the affected limb. The patient is unable to move the leg and complains that the leg feels cold. With intermittent claudication, there is pain on walking, relieved by rest. It may affect the calf, thigh or buttock. Rest pain in the foot may occur with advanced arterial disease. The pain is often worse in bed at night and the patient obtains relief by hanging the foot out of bed.
Neurological
Pain down the back of the leg (sciatica) often made worse by coughing, movement or straining. The patient may also complain of backache with painful spasm in the back muscles. There are restricted movements of the spine. Neurogenic claudication results from central spinal canal stenosis. Symptoms improve with flexion, as this increases the diameter of the canal. Therefore, patients find it easier to cycle than walk and easier to walk upstairs than downstairs. With neurogenic claudication, the claudication distance becomes progressively shorter with each bout of pain during one walk but not with vascular claudication. It also takes the pain of neurogenic claudication longer to settle than the pain of vascular claudication. The two forms of claudication may co-exist, making diagnosis difficult.
Metabolic
Gout presents as acute severe pain with redness and swelling of a joint. There may be a history of previous episodes. History of trauma, surgery, infection, diuretics, polycythaemia, leukaemia, cytotoxic therapy or immunosuppressive therapy.
Neoplastic
Osteogenic sarcoma usually presents in men between 20 and 40 years old. There is usually swelling around the knee, the commonest sites of the tumour being the lower femur or upper tibia. The patient often complains of bone pain, swelling or cough due to lung secondaries. Pain or pathological fractures may be due to secondary deposits. These may occur from the breast, lung, thyroid, prostate or kidney. Check for symptoms related to these or previous surgery for malignancy.
Other
Polymyalgia rheumatica usually occurs in elderly women. There is aching, morning stiffness in proximal muscles and often associated arthritis. Cramp is painful muscle spasm. The patient often complains of severe pain in the legs, especially at night or after exercise. It may occur with salt depletion, myopathy or muscle ischaemia. It is common in chronic renal failure.
Examination
Traumatic
Pain, loss of function, tenderness, deformity, crepitus, abnormal mobility. Check for associated nerve and vascular injuries.
Inflammatory
Pain in joints, swelling, tenderness, loss of movement, fixed deformities, disturbances of gait. Signs of rheumatoid arthritis elsewhere. Reiter’s disease – conjunctivitis, urethritis. Ankylosing spondylitis – stiffness of the spine, reduced thoracic excursion, fixed kyphotic spine, hyperextended neck.
Infective
In acute cellulitis, there is redness and tenderness over the affected area. Inguinal lymphadenopathy may be present. With acute osteomyelitis, there is tenderness and heat over the site of infection. With myositis, there is tenderness and wasting of the muscles. There may be other signs of collagen diseases, e.g. polyarteritis nodosa, SLE, scleroderma or dermatomyositis. In septic arthritis, there is a hot, tender, painful, swollen joint and all movements are painful. Surrounding muscle spasm is present.
Degenerative
In osteoarthritis, there is deformity, synovial thickening, bony enlargement due to osteophytes, effusion, loss of movement and fixed deformities. Baker’s cyst presents as a swelling in the popliteal fossa. If it has ruptured there is pain and swelling of the calf. Meniscal lesions present with swelling of the knee and tenderness over the joint line in the early phase. Later, there may be a continued effusion with wasted quadriceps and a positive McMurray sign.
Vascular
Deep vein thrombosis presents with pain, tenderness, swelling and heat, usually over the calf. There is ankle oedema. With iliofemoral thrombosis, there may be phlegmasia alba dolens (white leg) or phlegmasia cerulea dolens (painful blue leg). Acute ischaemia presents with the five Ps: pain, pallor, pulselessness, paraesthesia and paralysis. Check for atrial fibrillation. With intermittent claudication, examine for absent pulses. Buerger’s test.
Neoplastic
There is usually a hot, tender swelling around the knee joint in either the lower femur or upper tibia. Examine the chest for lung metastases. With secondary deposits, check the lung, breast, thyroid, prostate and kidney.
Neurological
Lordosis, limited straight leg raising, restricted back movements. Reduced reflexes in the lower limb. Areas of absent sensation.
Metabolic
With gout, there will be a tender, red, swollen joints with limitation of movement. Check for gouty tophi elsewhere.
Other
Polymyalgia rheumatica presents with tenderness over muscles and arthritis. Occasionally there is associated giant cell arteritis.
Examine the temporal artery for tenderness. With cramp, there may be signs of chronic renal failure.
General Investigations
■ FBC, ESR
Hb ↓ anaemia of chronic disease, e.g. rheumatoid arthritis, collagen disease. WCC ↑ infection, e.g. osteomyelitis, septic arthritis. ESR ↑ inflammation, e.g. rheumatoid arthritis, malignancy, polymyalgia rheumatica.
■ CRP
↑ infection/inflammatory disease.
■ U&Es
Chronic renal failure. Renal involvement in collagen disease.
■ LFTs
Alkaline phosphatase ↑ in liver secondaries.
■ Rheumatoid factor
Rheumatoid arthritis.
■ Blood glucose
Diabetes – neuropathy, peripheral vascular disease.
■ Local X-rays
Fractures. Osteoarthritis. Rheumatoid arthritis. Chronic osteomyelitis. Tumours.
■ Lumbosacral spine X-ray
Disc lesions. Osteophytes. Narrowing of joint spaces. Lordosis.