Arm Pain
This section deals with pain in the upper limb unrelated to joint pains. The majority of causes of arm pain are related to either neurological or vascular lesions. Musculoskeletal causes of arm pain are covered in the chapter on Joint Disorders (p. 267).
Causes
Cervical Lesions
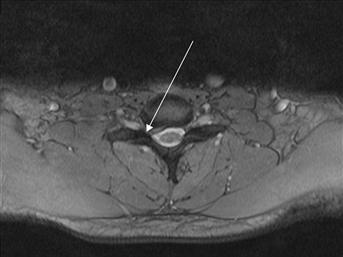
Figure 4 A trans-axial image showing a right-sided acute disc bulge at C6–C7 level, which is compressing the C7 nerve root in the exit foramen (arrow).
The patient will experience pain in the right arm radiating into the middle finger (dermatomal distribution of C7) and weakness of extension of the elbow (weak triceps-myotomal distribution of C7). There will be a reduced or absent triceps reflex.
Brachial Plexus
Vascular Lesions
History
Symptoms of cervical lesions include: pain and stiffness in the neck; pain radiating down the arm. Cervical cord compression may occur.
Cervical spondylosis represents ‘wear and tear’ of the cervical spine. It is common over the age of 60 years. Acute disc lesions usually occur in the younger patient. A careful history is needed to exclude trauma.
Brachial plexus lesions refer pain down the arm and may result from localised lesions, e.g. a cervical rib causing extrinsic compression will affect T1 and cause wasting of the small muscles of the hands and paraesthesia in the dermatomal distribution, i.e. the inner aspect of the upper arm.
Subclavian artery stenosis will result in ‘claudication’ in the arm, i.e. pain brought on by exercise, relieved by rest, due to inadequate blood flow. A history of cardiac problems, e.g. AF or widespread arterial disease, will suggest embolism or thrombosis. A sudden onset of a painful, swollen, cyanotic limb will suggest axillary vein thrombosis. Pain radiating into the left arm brought on by exercise and related to central chest pain and pain radiating into the neck suggests myocardial ischaemia. Pain associated with occupation, e.g. writing, word-processing (keyboard occupations), suggests repetitive strain injury. A history of diabetes mellitus, renal failure, liver failure, alcohol abuse, vitamin B12 deficiency, drugs, e.g. phenytoin or vincristine, suggests peripheral neuropathy.
Pain, paraesthesia in the thumb, index and middle finger, which is worse in bed at night and relieved by hanging the arm out of bed, would suggest carpal tunnel syndrome. The latter may be associated with pregnancy, rheumatoid arthritis, myxoedema, anterior dislocation of the lunate, gout, acromegaly, amyloidosis and arteriovenous fistula at the wrist created for haemodialysis.
Localised bone pain may be due to primary or secondary tumours. The latter are most common and may result from a primary in the breast, bronchus, thyroid, prostate or kidney. Pathological fractures may occur. With compartment syndrome, there may be a history of crush injury, vascular injury or vascular surgery. Chronic compartment syndrome may result from unusual exertion, e.g. weight-lifting.
Examination
A full neurological examination should be carried out, looking for cervical lesions, brachial plexus lesions or carpal tunnel syndrome. There may be limitation in movements of the cervical spine. The limbs should be examined for swelling, e.g. axillary vein thrombosis, when there will be cyanosis and dilated veins. Examine for signs of ischaemia and feel for pulses. The classical signs of an ischaemic limb, i.e. pain, pallor, pulselessness, paraesthesia, ‘perishing cold’ and paralysis, may be present. Occupation will suggest repetitive strain injury and there will usually be little to find on examination. Horner’s syndrome (ptosis, miosis, enophthalmos and anhidrosis) suggests Pancoast’s tumour. With bone tumours, there will be localised swelling and tenderness. With compartment syndrome, there will be a swollen tender compartment in the forearm, paraesthesia and paralysis. Pulses may be normal initially; later they are reduced or absent.
General Investigations
■ FBC, ESR
WCC ↑ infection, e.g. osteomyelitis or cervical spine TB. ESR ↑ infection and malignancy.
■ CRP
Infection/inflammatory cause.
■ Cervical spine X-ray
Cervical spondylosis, bony metastases, cervical spine fractures.
■ CXR
Malignancy resulting in bone secondary. Pancoast’s tumour (apical lung tumour spreading to involve brachial plexus). Cervical rib (13 ribs).




