229 Paget’s disease
Salient features
History
• Ask the patient whether there is an increase in hat size
• Joint pain (from osteoarthritis secondary to bone disease)
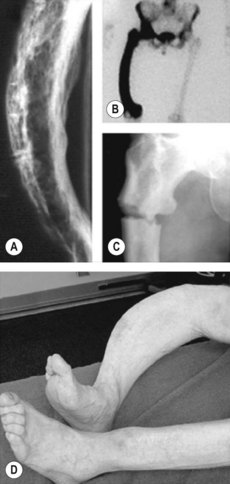
• Painless bowing of the bone can be the first symptom
• Fractures with minimal trauma
• Nerve entrapment syndromes including paraparesis and radioculopathy when the spine is affected.
Examination
Remember: Paget’s disease is a remodelling disease of isolated areas of the skeleton.
Questions
What are complications of Paget’s disease?
• Basilar invagination can lead to a ‘Tam O’Shanter’ deformity
• Cord compression from basilar invagination
• Narrowing of basal foramina, producing cranial nerve lesions, especially deafness, and occasionally compression of the medulla oblongata or upper spinal cord
Advanced-level questions
What is the basic defect in bone metabolism?
Increased osteoclastic activity resulting in bone resorption and increased osteoblastic activity.
What are the radiological manifestations of this disease?
• Skull: ‘honeycomb’ appearance with underlying osteoporosis circumscripta, ‘cottonwool’ appearance
• Pelvis: thickening of the iliopectineal line ‘brim-sign’, enlargement of ischial and pubic bones
• Long bones: increased trabeculation and localized bone enlargement
• Vertebra: sclerotic margins giving a ‘picture frame’ appearance.
Remember: A bone scan is more sensitive than a radiograph in determining the extent of disease.
What factors have been implicated in the aetiology of Paget’s disease?
• Slow viral infection: measles syncytial virus, paramyxovirus (canine distemper)
• Genetic factors: mutations have been identified in at least four genes. The most important of these is SQSTM1, encoding sequestosome 1, a scaffold protein in the nuclear factor NF-κB signalling pathway. Patients with SQSTM1 mutations have severe Paget’s disease of bone and a high degree of penetrance with increasing age
• Other potential triggers include deficiency of dietary calcium and repetitive mechanical loading of the skeleton.






