Chapter 9 Paediatrics
General Paediatrics
Physiological changes at birth
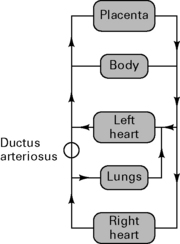
Neonatal physiology
CVS
Respiratory
Renal
CNS
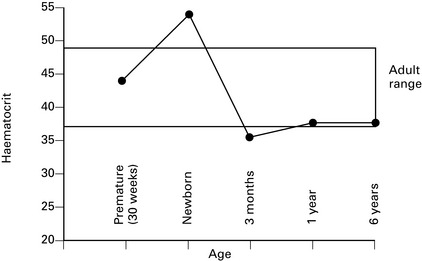
Blood
Temperature
General anaesthesia
Preoperative fasting
CONSENSUS GUIDELINE ON PERIOPERATIVE FLUID MANAGEMENT IN CHILDREN, V1.1
Association of Paediatric Anaesthetists of Great Britain and Ireland 2007
Executive summary
| Body weight | Daily fluid requirement |
|---|---|
| 0–10 kg | 4 mL/kg per h |
| 10–20 kg | 40 mL/h + 2 mL/kg per h above 10 kg |
| >20 kg | 60 mL/h + 1 mL/kg per h above 20 kg |
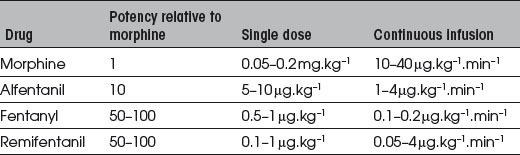
Analgesia in neonates
Regional techniques
Spinal cord ends at L3; dura ends at S4.
Epidural
Table 9.2 Maximum dosages of bupivacaine, levobupivacaine and ropivacaine in neonates and children
| Single bolus injection | Continuous postoperative infusion | |
|---|---|---|
| Maximum dosage | Maximum infusion rate | |
| Neonates | 2 mg.kg−1 | 0.2 mg.kg−1.h−1 |
| Children | 2.5 mg.kg−1 | 0.4 mg.kg−1.h−1 |
GUIDELINES ON THE PREVENTION OF POSTOPERATIVE VOMITING (POV) IN CHILDREN
The Association of Paediatric Anaesthetists of Great Britain and Ireland, Spring 2007
Children at high risk of POV
What anaesthetic factors affect POV in children?
Recommendations for prevention of POV in children
Congenital diaphragmatic hernia
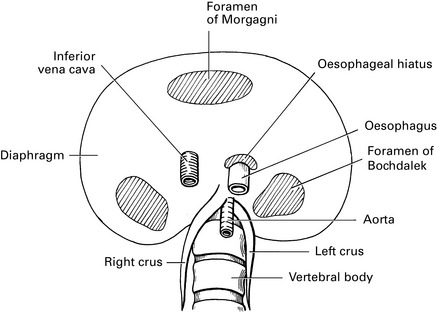
Sequelae
Symptoms depend upon degree of hypoplasia:

(Dilute in equal volume of 10% glucose prior to i.v. administration.)
General anaesthesia
Hypertrophic pyloric stenosis
Resuscitate preoperatively with normal saline 0.9% to correct acid–base balance and dehydration:

 mismatch prolonging gas induction.
mismatch prolonging gas induction.Al-Rawi O., Booker P.D. Oesophageal atresia and tracheo-oesophageal fistula. Contin Edu Anaesth, Crit Care Pain. 2007;7:15-19.
American Society of Anesthesiologists’ Task Force on Preoperative Fasting. Practice guidelines for preoperative fasting and the use of pharmacologic agents to reduce the risk of pulmonary aspiration: application to healthy patients undergoing elective procedures. Anesthesiology. 1999;90:896-905.
Association of Paediatric Anaesthetists of Great Britain and Ireland. APA consensus guideline on perioperative fluid management in children, v1.1. APAGBI, London, 2007. www.apagbi.org.uk.
Association of Paediatric Anaesthetists of Great Britain and Ireland. Guidelines on the prevention of post-operative vomiting in children. APAGBI, London, 2007. www.apagbi.org.uk.
Bingham B. Paediatric anaesthesia: past, present and future. Anaesthesia. 2003;58:1194-1196.
Fell D., Chelliah S. Infantile pyloric stenosis. BJA CEPD Rev. 2001;1:85-88.
Gormley S.M., Crean P.M. Basic principles of anaesthesia for neonates and infants. BJA CEPD Rev. 2001;1:130-134.
Holliday M.A., Segar W.E. The maintenance need for water in parenteral fluid therapy. Pediatrics. 1957;19:823-832.
King H., Booker P.D. Congenital diaphragmatic hernia in the neonate. Contin Edu Anaesth, Crit Care Pain. 2005;5:171-174.
Lönnqvist P.A., Morton N.S. Postoperative analgesia in infants and children. Br J Anaesth. 2005;95:59-68.
Marsh D.F., Hodkinson B. Remifentanil in paediatric anaesthetic practice, Anaesthesia. 2009;64:301-308.
Rowney D.A., Doyle E. Epidural and subarachnoid block in children. Anaesthesia. 1998;53:980-1001.
Paediatric Cardiology
Anaesthesia for congenital cardiovascular disease
General anaesthesia
General aims
Monitoring
Greenley W.J., Kern F.H. Anesthesia for pediatric cardiac surgery. In: Miller R.D., editor. Anesthesia. Edinburgh: Churchill Livingstone; 1994:1811-1850.
Javorski J.J., Burrows F.A. Pediatric cardiac anesthesia. Curr Opin Anaesth. 1995;8:62-67.
Long T.J. Pediatric cardiology and cardiac surgery update. Curr Opin Anaesth. 1997;10:221-226.