Paediatric skull—suspected NAI
Normal anatomy
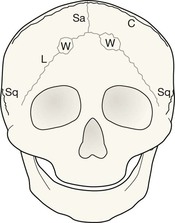
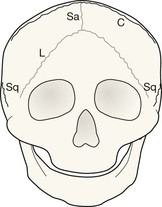
Infants and toddlers—normal accessory sutures
Evaluating the SXR in an infant or toddler presents unique problems. Diagnostic confusion between sutures and fractures may have serious consequences. A basic understanding of the locations and variable appearances of these sutures will help to reduce the likelihood of misdiagnosis4–8.
A basic classification of skull sutures in infants and toddlers
| Grouping | Notes | Sutures |
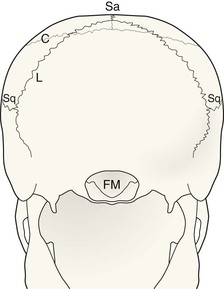
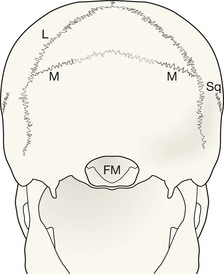
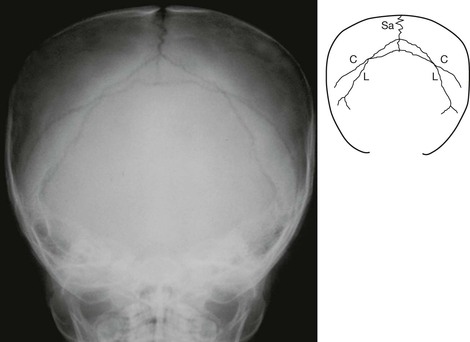
| The normal sutures | Visible on the SXR in all infants and toddlers – persisting in all adults | Sagittal, coronal, lambdoid, squamosal, and smaller sutures around the mastoid |
| A normal developmental suture | Visible on the SXR in all infants and many toddlers – but not in adults | Innominate |
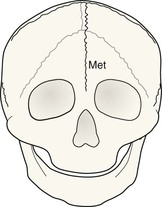
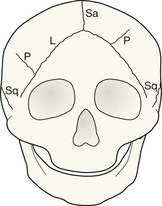
| The most common accessory sutures | Visible on the SXR in some infants and toddlers – occasionally persisting to adulthood | Metopic, accessory parietal, mendosal |
Normal accessory sutures and the radiographs on which they are seen
| Suture | Most commonly seen on | Notes |
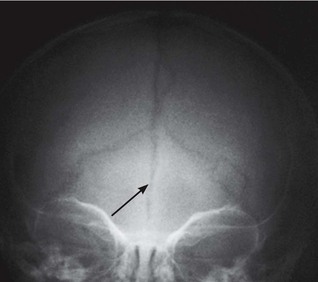
| Metopic suture | Frontal √ √ Towne’s √ |
The commonest accessory suture. It is also the one that most commonly persists in older children, and even in a few adults. |
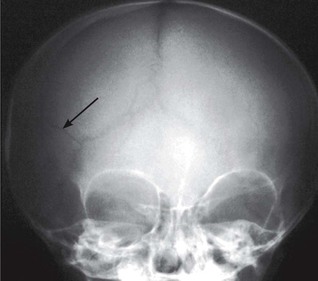
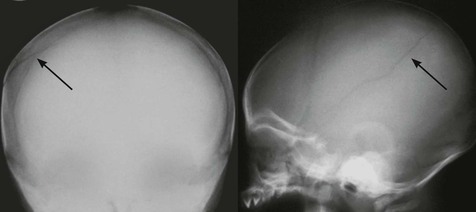
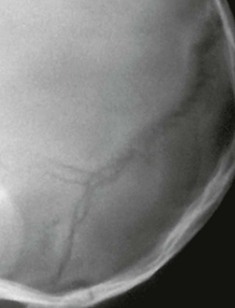
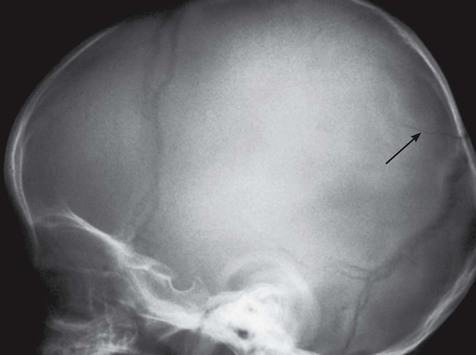
| Accessory parietal suture | Towne’s √ √ Frontal √ Lateral √ |
May be complete or incomplete. Occurs in vertical, horizontal or oblique orientations. Most commonly vertical. |
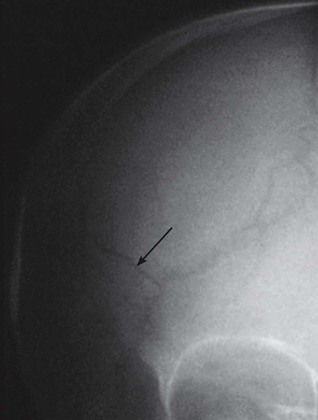
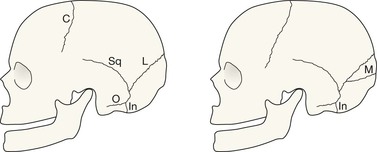
| Mendosal suture | Lateral √ √ Towne’s √ |
Extends posteriorly from the lambdoid suture on the lateral view. Passes medially on Towne’s view. |
| Innominate suture | Lateral √ √ | Sometimes classified as an accessory suture but best regarded as a normal developmental suture because it is always present in infants. As the child matures this suture disappears. |
The lateral SXR
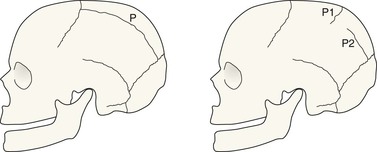
Accessory parietal sutures vary in position. This drawing does not correspond to any radiographic projection. It shows the general positions and direction of the more common incomplete accessory parietal sutures (P1 and P2) when looking down from above the cranium.

Analysis: suture recognition
The principal question: is it a suture or a fracture?4–8
When assessing suspected non-accidental injury (NAI) in young children, be very careful not to rush too swiftly to judgement. Observing an abnormality is important. An informed approach is then required when assigning a particular significance to the abnormality9–12.
Be aware …
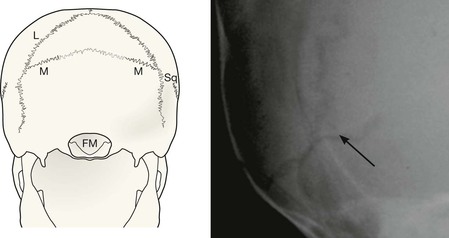
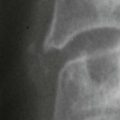
Suture recognition on the lateral view
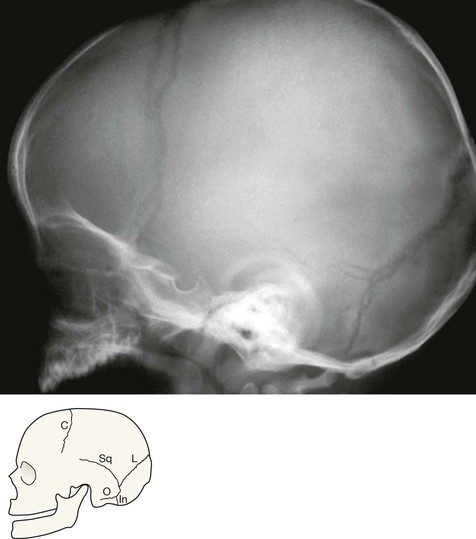
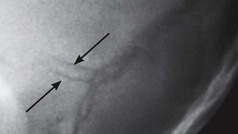
Lambdoid suture. As it nears the base of the skull (in the region of the mastoid bone) the suture appears to be complex. This seemingly tangled appearance is mainly caused by overlapping of the normal occipitomastoid sutures on the right and left sides. Don’t worry about this. Arising from the lambdoid suture there will be:
Suture recognition on the AP view