[level-membership-for-emergency-medicine-category]
2.2 Paediatric basic life support
Paediatric versus adult basic life support
Anatomy and physiology
Preparation and equipment
Basic life support sequence
A ‘SAFE’ approach
Airway
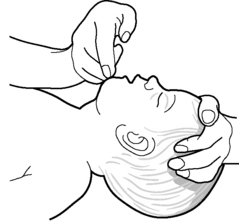
Open and maintain the airway
Three manoeuvres will assist in opening and maintaining the airway (Figs 2.2.1, 2.2.2 and 2.2.3), which is most commonly obstructed by the child’s tongue.


Circulation
Chest compressions
The technique of providing ECC varies with the patient’s age.




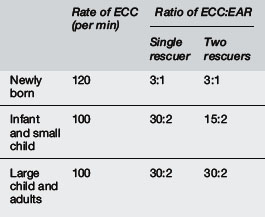
Compression to ventilation ratio
For a lone rescuer, external cardiac compressions should be combined with expired air resuscitation in a ratio of 30 compressions to 2 ventilations for all age groups (except neonates – see below). Healthcare providers performing two-rescuer BLS should use a ratio of 15 compressions to 2 ventilations for all infants and children (see Table 2.2.1). Note that the ratio of 30:2 is utilised in adults regardless of the number of rescuers.
Relief of foreign body airway obstruction
FBAO management in the unresponsive patient
The sequence of response for an unresponsive, apnoeic patient with FBAO is as follows:
 Open the airway using chin lift or jaw thrust. Look inside the mouth and remove any visible foreign body. Do not perform a blind finger sweep because of the risk of damaging palatal tissues or pushing a foreign body further into the airway.
Open the airway using chin lift or jaw thrust. Look inside the mouth and remove any visible foreign body. Do not perform a blind finger sweep because of the risk of damaging palatal tissues or pushing a foreign body further into the airway.
 If rescue breaths are still unsuccessful, perform a sequence of five back blows and five chest thrusts.
If rescue breaths are still unsuccessful, perform a sequence of five back blows and five chest thrusts.

For management in the emergency department setting see inhaled FB (Chapter 6.2).


FBAO management in the unresponsive child


Advanced Life Support Group. Advanced paediatric life support: The practical approach, 4th rev. ed. BMJ Publishing Group: London, 2004.
3 Australian Resuscitation Council Guidelines. sections 12 and 13 http://www.resus.org.au/; December 2010
Biarent D., Bingham R., Eich C., et al. European Resuscitation Council Guidelines for Resuscitation. Section 6: Paediatric life support. Resuscitation. 2010;81(10):1364-1368.
International Liaison Committee (ILCOR). Consensus on Science with Treatment Recommendations for Pediatric and Neonatal Patients: Pediatric Basic and Advanced Life Support. Pediatrics. 117(5), 2005.
Kleinman M.E., de Caen A.R., de Chameides L., et al. Part 10: Pediatric basic and advanced life support: 2010 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations. Circulation. 2010;16(Suppl 2):S466-515.
Richmond S., Wyllie J. European Resuscitation Council Guidelines for Resuscitation. Section 7: Resuscitation of babies at birth. Resuscitation. 2010;8(10):1389-1399.
[/level-membership-for-emergency-medicine-category][not-level-membership-for-emergency-medicine-category]
2.2 Paediatric basic life support
