Chapter 43 Overview of Transtemporal Skull Base Surgery
OBJECTIVE
The modern era of neurotologic transtemporal skull base surgery began in 1961, when House introduced the operating microscope and multidisciplinary surgery for removal of acoustic neuromas. The conceptual advantage of this transtemporal technique was a wide exposure of the lesion with substantially less cerebellar retraction than the techniques available at that time, in addition to direct facial nerve preservation. With its low mortality rate and enhanced facial nerve preservation rate, House established the translabyrinthine procedure as a technique with which all other microsurgical approaches to the cerebellopontine angle are compared.1 The emphasis on functional preservation has increased over the years from the initial enthusiasm with ablative skull base approaches.2,3 As surgeons and patients are demanding better outcomes, such strategies as the fallopian bridge technique4 to avoid facial nerve mobilization, partial labyrinthine occlusion to preserve hearing,5–7 and endoscopic strategies8 to minimize incisions have decreased the morbidity of surgery.
Figure 43-1 presents an organizational framework for transtemporal surgery based on management of the otic capsule. The otic capsule is selected as the organizational center based on its function and location. Functionally, anatomic preservation of the otic capsule is the requirement for preservation of audiovestibular function (although exceptions to this principle are developing). Anatomically, the paired petrous pyramids encompass the center of lateral skull base exposure. The approaches presented in Figure 43-1 can be used individually; however, in certain cases, combinations of these approaches offer the ideal exposure.
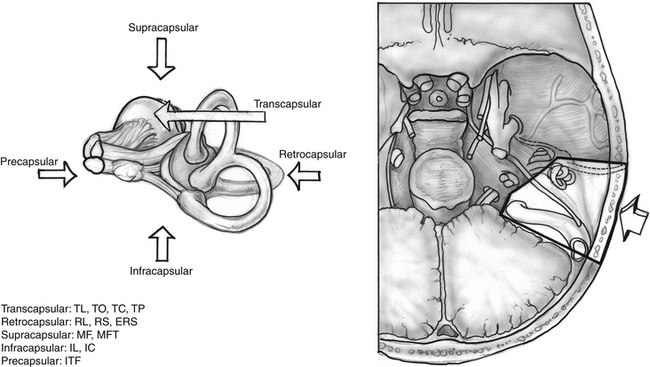
Approaches that traverse the otic capsule (transcapsular) permit wide exposure by sacrificing hearing: translabyrinthine (see Chapter 49), transcochlear (see Chapter 52), and transotic (see Chapter 51). The posterior approaches that spare the otic capsule (retrocapsular) provide varying degrees of cerebellopontine angle exposure with an opportunity for hearing preservation: retrolabyrinthine (see Chapter 36) and retrosigmoid (see Chapter 50). Superior approaches (supracapsular) permit unroofing the internal auditory canal with varying degrees of petrous apex exposure and an opportunity for hearing preservation: middle fossa (see Chapter 48) and middle fossa transpetrous (see Chapter 53).
Combined approaches permit the widest transtemporal exposure with varying opportunities for preservation of neurologic function: retrolabyrinthine petrosal (see Chapter 56), translabyrinthine petrosal (see Chapter 56), and transcochlear petrosal (see Chapter 56). The inferior approaches (infracapsular) permit minimally invasive access for drainage of cystic lesions of the petrous apex: infracochlear and infralabyrinthine (see Chapter 45). The anterior approaches (precapsular), such as the infratemporal fossa (see Chapter 54) techniques, permit exposure to the middle skull base, including the region of the foramen ovale, foramen spinosum, foramen lacerum, pterygoid space, and avenues to the nasopharynx and paranasal sinuses. These lateral approaches can be combined with facial disassembly and endoscopic sinus approaches in selected cases.
NOMENCLATURE
There has been a rapid expansion of terminology describing skull base surgical approaches. The techniques and their applications have evolved extensively. In the context of this rapid expansion of application and techniques, there has been a conflicting development of terminology for these approaches. Not only are various eponyms attached to the approaches, but also the same terms are used for different surgical techniques. Because of the potential conflict and debate over attribution, eponyms for the description of surgical approaches generally should be avoided. Instead, anatomic terminology should be selected. Considering transtemporal surgical approaches to the skull base, even this concept becomes confusing. Conceptually, most of these transtemporal approaches involve management of the petrous bone. These approaches have all rightfully been described as petrosal approaches in various modifications at different times. The terminology in Figure 43-1 is anatomically descriptive based on the structures of the otic capsule itself. Generally, we use the term petrosal approaches for combined posterior fossa and subtemporal surgical techniques that include division of the superior petrosal sinus (see Chapter 56).
COLLABORATION IN TRANSTEMPORAL SURGERY
Multidisciplinary transtemporal approaches for posterior fossa skull base neoplasms are an adjunct and not a substitute for standard neurosurgical techniques in managing these lesions. The neuro-otologist and neurosurgeon are truly cosurgeons in the management of these lesions, each having intimate familiarity with the other’s role.9 Many of the following chapters are coauthored by otolaryngologists and neurosurgeons reflecting the true collaborative nature of modern skull base surgery. Precise temporal bone management offers the operative team flexibility to tailor the management to a patient’s specific anatomic and functional needs.
1. Arriaga M. Anatomy of transtemporal surgery. In: Janecka I.P., Tiedemann K., editors. Skull Base: Anatomy, Biology and Technology. Philadelphia: Raven-Lippincott, 1997.
2. Sekhar L.N., Janecka I.P. Surgery of Cranial Base Tumors. New York: Raven Press; 1993.
3. Arriaga M.A., Janecka I.P. Facial translocation approach to the cranial base: The anatomical basis. Skull Base Surg. 1991;1:22-30.
4. Pensak M., Jackler R. Removal of jugular foramen tumors: The fallopian bridge technique. Otolaryngol Head Neck Surg. 1997;117:586-591.
5. Hirsch B.E., Cass S.P., Sekhar L.N., et al. Translabyrinthine approach to skull base tumors with hearing preservation. Am J Otol. 1993;14:533-543.
6. McElveen J.T., Wilkins R.H., Erwin A., et al. Modifying the translabyrinthine approach to preserve hearing during acoustic tumor surgery. J Laryngol Otol. 1991;105:34-37.
7. Arriaga M.A., Gorum M. Enhanced retrosigmoid exposure with posterior semicircular canal resection. Otolaryngol Head Neck Surg. 1996;115:46-48.
8. Zimmer L.A., Hirsch B.E., Kassam A., et al. Resection of a recurrent paraganglioma via an endoscopic transnasal approach to the jugular fossa. Otol Neurotol. 2006;27:398-402.
9. Arriaga M.A., Day J. Neurosurgery and Otolaryngology: Principles and Practice of Collaborative Surgery. Philadelphia: Lippincott; 1999.