Ovarian Cystectomy and Cystotomy
Any cystic mass of the ovary has the potential for malignancy. A frozen section should be performed when a conservative treatment plan has been selected. Cystectomy permits the cystic structure to be selectively removed while the residual ovarian tissue is preserved. Cystectomy may be performed for functioning cysts (follicular and corpus luteum), benign cystic teratomas, and endometriotic cysts.
The technique for cystectomy is similar for all of the preceding conditions. The ovary is stabilized with placement of a Babcock clamp on the utero-ovarian ligament (Fig. 22–1). If the procedure is performed by laparotomy, then 3-0 Vicryl traction sutures may be placed into the ovarian tissue outside of the cystic area. The stitches are clamped with mosquito clamps and held by an assistant. A 1 : 200 vasopressin solution is injected into the stretched-out capsule of the ovary, which overlies the cyst (Fig. 22–2). An incision is made into the capsule with an energy device (laser or electrosurgical) or knife (Figs. 22–3 and 22–4).
The incision between the cyst wall and the ovarian capsule provides a plane that can be dissected on either side of the initial incision (Figs. 22–5 and 22–6). The incision may be extended at will to facilitate separation of the cyst from the ovarian capsule (Fig. 22–7A, B). The dissection continues to completely circumscribe the ovary (Fig. 22–7C). Finally, the base of the cyst is clamped or coagulated, and the cyst is removed intact and sent to pathology (Fig. 22–7D). Any ovarian cyst other than an obvious corpus luteum cyst should be sent for frozen section. The remaining capsular tissue is folded upon itself, and no sutures are placed. Alternatively, the excess capsule may be trimmed away and the ovary closed with 4-0 Vicryl.
In some circumstances, particularly with endometriomas, difficulty may be encountered in stripping away the ovarian capsule from the cyst wall (Fig. 22–8). In these cases, the author has preferred to resect a portion of the ovary that includes approximately 50% of the cyst and then to vaporize the cyst lining from the inside. The technique is described as follows.
The utero-ovarian ligament is grasped with Babcock clamps. Stabilizing sutures of 3-0 Vicryl are placed into the periphery of the ovary outside the field of proposed resection (Fig. 22–9). A carbon dioxide (CO2) laser or other suitable energy device is selected to cut the ovary. Alternatively, 1 : 200 vasopressin can be injected and a knife utilized (Fig. 22–10). The cyst is opened linearly and drained (Fig. 22–11A–C). A hemisphere of ovary is cut away (Fig. 22–12). The interior lining of the cyst is then vaporized (Fig. 22–13). The char is irrigated away (Fig. 22–14A–C). The edges of the ovary are grasped and approximated by suturing the obliterated cyst wall together with 3-0 Vicryl and then approximating the wound margin with 3-0 or 4-0 Vicryl (Fig. 22–15). The reconstituted ovary now has been reduced to normal size (Fig. 22–16).
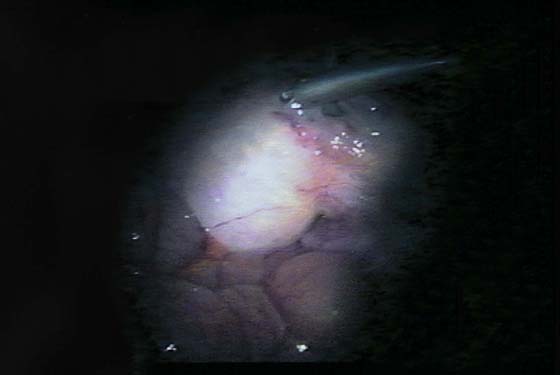
FIGURE 22–1 The ovary is enlarged by a benign cystic teratoma.
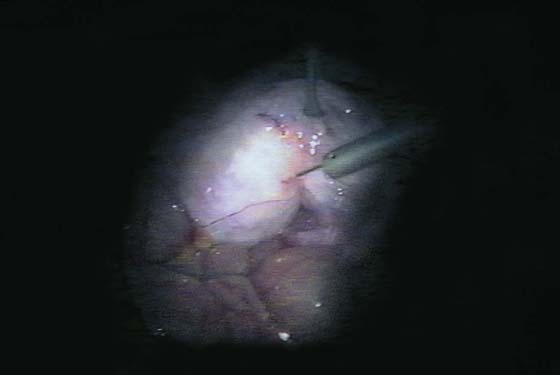
FIGURE 22–2 The cyst is injected with a 1 : 200 vasopressin solution before the cystectomy is begun.

FIGURE 22–3 Carbon dioxide (CO2) laser trace spots are placed into the ovary to indicate the direction or extent of the incision. This may be done with a bipolar needle or by scoring the tissue with a shallow knife incision.
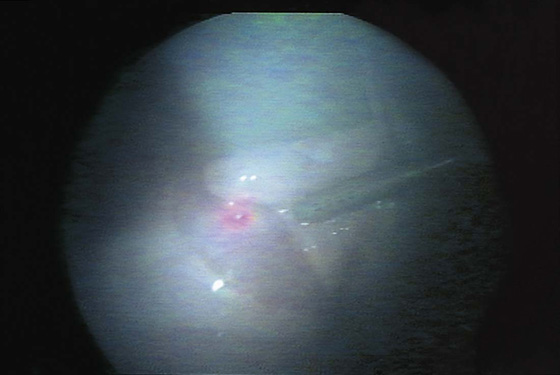
FIGURE 22–4 A cut has been created along the previously marked incision line. Note that the ovarian capsule partially retracts from the underlying cyst wall. A haze is created by the smoke of the energy source vapor.

FIGURE 22–5 An irrigating cannula dissects a space between the capsule and the cyst wall with pressurized saline injection.

FIGURE 22–6 Dissection of the cyst wall continues circumferentially around the ovary.


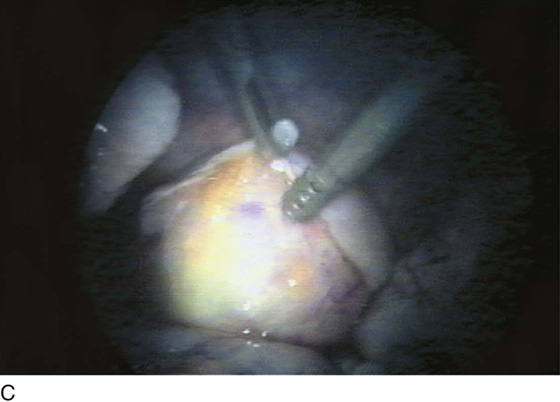

FIGURE 22–7 A. The initial incision is extended to facilitate mobilization of the cyst. B. When the incision extension has been completed, further hydrodissection continues. C. The cyst has been 90% separated from the ovarian wall. D. The cyst has been completely separated from the ovary and is being removed from the abdominal cavity. In this case, the second laparoscopic puncture incision is lengthened to create a microlaparotomy.
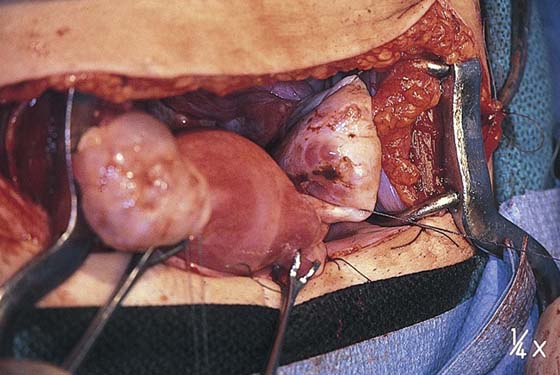
FIGURE 22–8 Bilateral, large endometriomas. The endometrial cysts are approximately as large as the uterus.
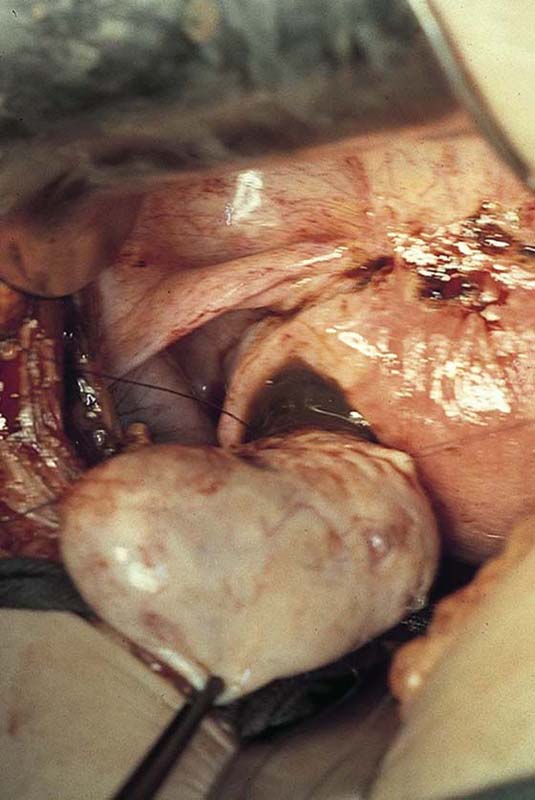
FIGURE 22–9 Stay sutures are placed into the ovary for traction.
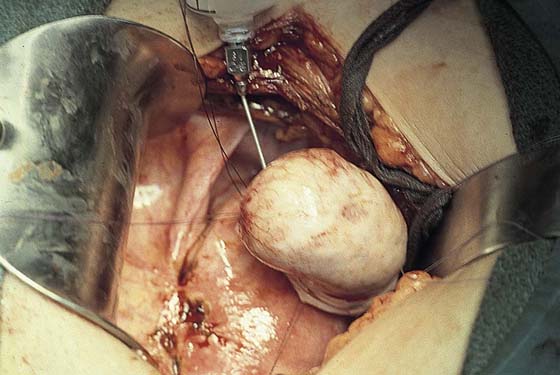
FIGURE 22–10 A 1 : 200 vasopressin solution is injected into the ovary for hemostasis before the cystic structure is opened.
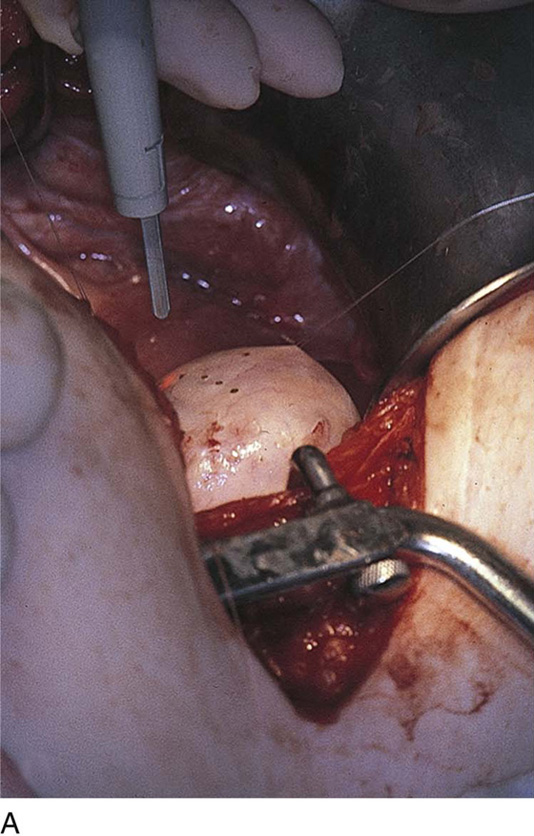
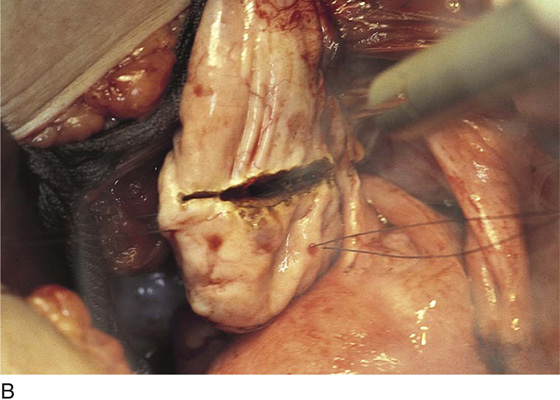
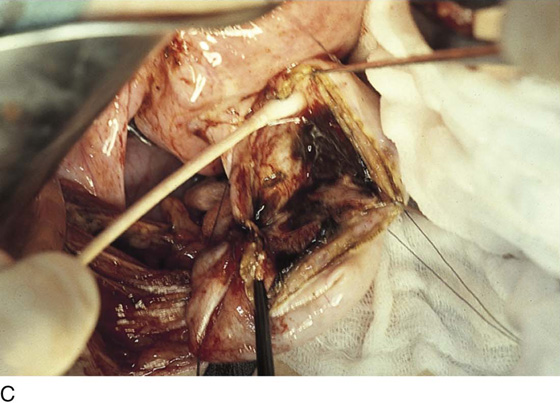
FIGURE 22–11 A. Laser trace spots (carbon dioxide [CO2] laser) made with a superpulse mode trace the extent of the incision to be made. B. As the incision cuts into the interior of the cyst, dark brown bloody fluid escapes from the ovary and is suctioned away from the field. C. Approximately half of the enlarged ovary is resected. The interior of the remaining half containing a portion of the interior cyst wall is irrigated to clean out any residual bloody contents.

FIGURE 22–12 The excised cyst is examined and sent to pathology.
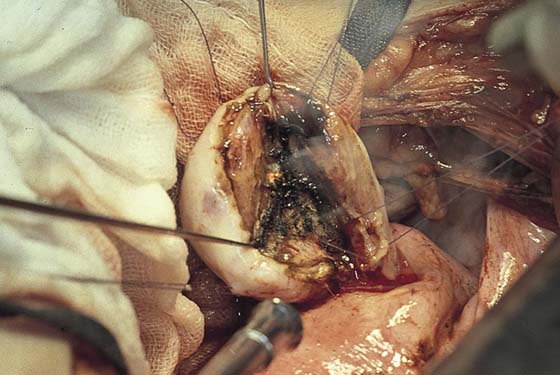
FIGURE 22–13 The carbon dioxide (CO2) laser is targeted to the interior of the remaining half of the ovary. The lining of the endometrioma is vaporized.
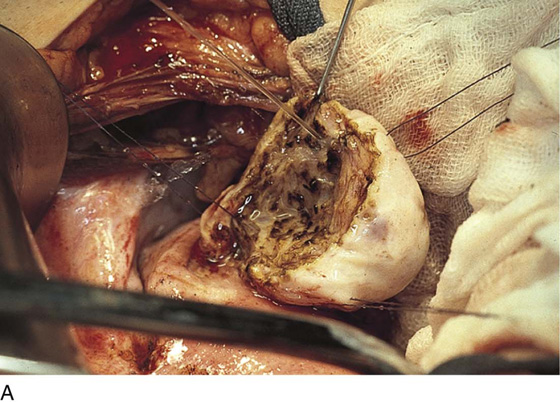

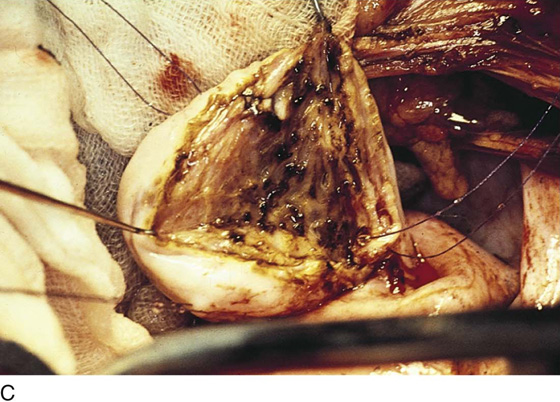
FIGURE 22–14 A. The char is irrigated with copious amounts of sterile normal saline injected under pressure. B. A saline-soaked cotton-tipped applicator further facilitates removal of devitalized tissue. C. The remaining ovarian tissue without cyst wall is ready for closure.
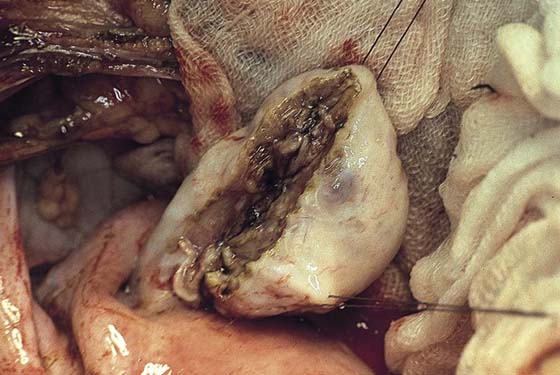
FIGURE 22–15 The cyst cavity is obliterated as 4-0 Vicryl sutures bring the opposing walls together. The vaporized surfaces will naturally adhere to each other.
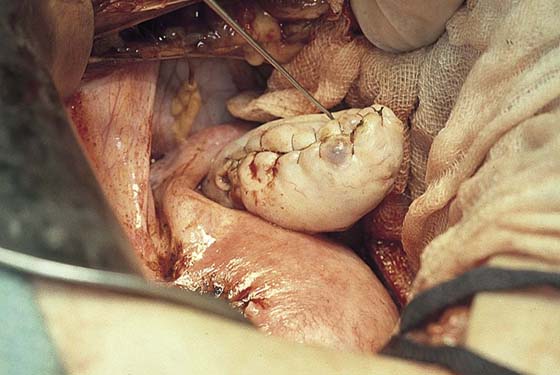
FIGURE 22–16 The capsule of the ovary is closed with a 4-0 Vicryl running suture. The net effect of the operation is elimination of the cyst with restoration of a normal-sized ovary.






