Chapter 31 Orthotics
31.1 Casting (Includes serial casting; casting for burns)
OVERVIEW.
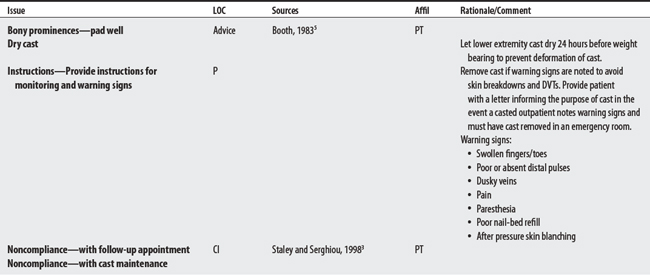
A cast is a rigid casing applied around a body part.1 Serial casting involves recasting over time and is used to treat contractures by affecting muscle length, soft tissue extensibility, and possibly affecting muscle spindle excitability. The applied load on soft tissue is low and duration is long (i.e., not a quick stretch). Casting of burns offers plastic deformation of connective tissue, biomechanical realignment of joint structures, and protection of exposed tendons, fragile skin, or wounds.
CONTRAINDICATIONS AND PRECAUTIONS
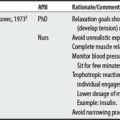
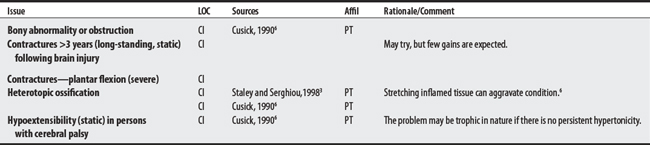
Serial Casting/Casting
F00-F99 MENTAL AND BEHAVIORAL DISORDERS

G00-G99 DISEASES OF THE NERVOUS SYSTEM

I00-I99 DISEASES OF THE CIRCULATORY SYSTEM

L00-L99 DISEASES OF THE SKIN AND SUBCUTANEOUS TISSUE

M00-M99 DISEASES OF THE MUSCULOSKELETAL SYSTEM AND CONNECTIVE TISSUE

S00-T98 INJURY, POISONING, AND CERTAIN OTHER CONSEQUENCES OF EXTERNAL CAUSES

1 Eisenberg MG. Dictionary of rehabilitation. New York: Springer, 1995.
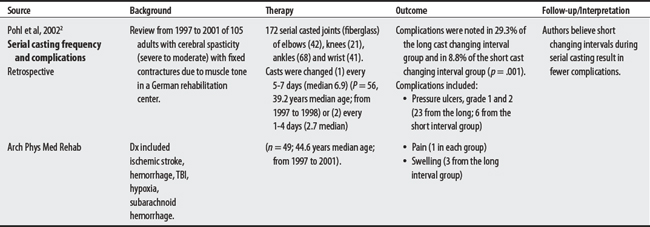
2 Pohl M, Ruckriem S, Mehrholz J, et al. Effectiveness of serial casting in patients with severe cerebral spasticity: a comparison study. Arch Phys Med Rehab. 2002;83(6):784-790.
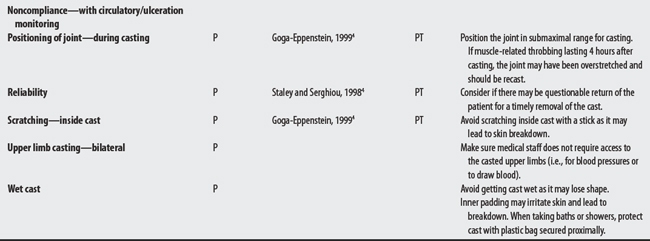
3 Staley M, Serghiou M. Casting guidelines, tips, and techniques: Proceedings from the 1997 American Burn Association PT/OT Casting workshop. J Burn Care Rehab. 1998;19(3):254-260.
4 Goga-Eppenstein P, Hill JP, Seifert TM, Yasukawa AM. Precautions and competency in cast application. In Casting protocols for the upper and lower extremities. The Rehabilitation Institute of Chicago Publication Series. Gaithersburg (MD): Aspen Publications; 1999.
5 Booth BJ, Doyle M, Montgamery J. Serial casting for the management of spasticity in the head-injured adult. Phys Ther. 1983;63(12):1960-1965.
6 Cusick BD. Progressive casting and splinting for lower extremity deformities in children with neuromotor dysfunction. Tucson (AZ): Therapy Skill Builders, 1990.
31.2 Orthotics
OVERVIEW.
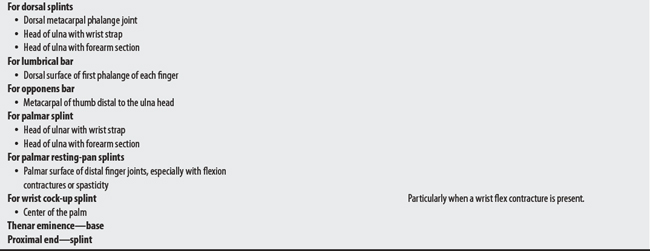
An orthosis is an external device that is worn on a body part to support, correct, or prevent deformities or to align body structures for improved function.1 Webster’s dictionary2 defines it as a straightening treatment for the maladjusted. The term splint varies in meaning and may refer to either a hand orthosis3 or a temporary external device.1 Some examples of orthoses include body jackets, hand splints, ankle foot orthoses, knee cages, elastic stockings, and corrective shoes.
SUMMARY.
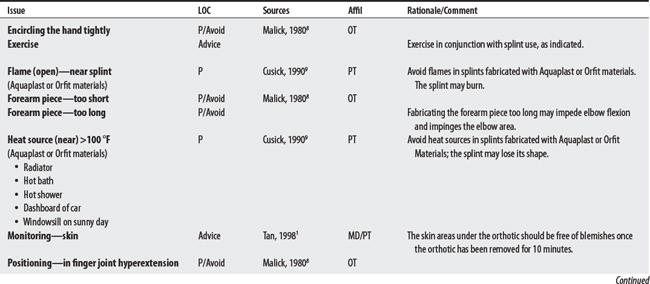
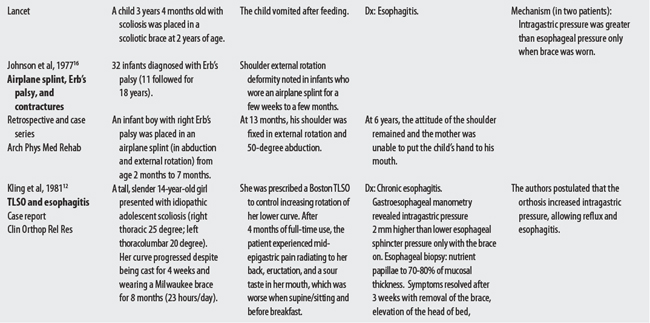
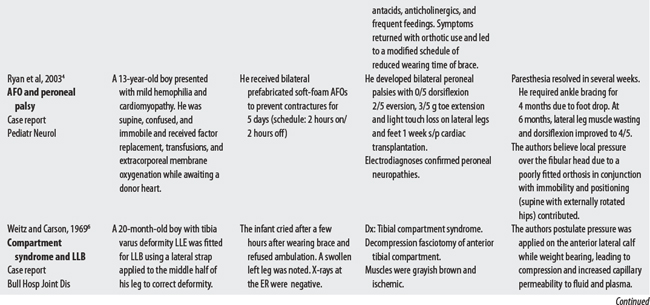
Concerns for spinal and lower and upper limb (including hand splints) orthotics are varied and depend in large part on the patient’s clinical presentation and involved body region. Skin monitoring is recommended in most, if not all, orthotic applications. In general, orthotic concerns include skin ulceration in insensate or poorly vascularized skin, skin allergies from splint materials, contracture promotion (e.g., using UE slings in persons with UMN lesions), worsened spasticity (e.g., using dynamic splints in persons with UMN lesions), and orthotics that either fail to adequately stabilize critical body segment (e.g., high cervical fracture) or fail to control a crucial movement component (e.g., deleterious rotational forces). In addition to pressure ulcer complications, pressure-related neuropathies4,5 and compartmental syndromes6 have been reported with orthotic use.
CONTRAINDICATIONS AND PRECAUTIONS
LOWER LIMB ORTHOTICS: GENERAL CONCERNS (INCLUDES SHOE ORTHOSES)
G00-G99 DISEASES OF THE NERVOUS SYSTEM

I00-I99 DISEASES OF THE CIRCULATORY SYSTEM











PROCEDURAL CONCERNS









PROCEDURAL CONCERNS


Helmet (Cranial Orthosis)
F00-F99 MENTAL AND BEHAVIORAL DISORDERS


Semirigid Plastic Collar with Chin and Occipital Piece*
S00-T98 INJURY, POISONING, AND CERTAIN OTHER CONSEQUENCES OF EXTERNAL CAUSES

Custom Cervical Bivalve
S00-T98 INJURY, POISONING, AND CERTAIN OTHER CONSEQUENCES OF EXTERNAL CAUSES

Philadelphia Collar with Thoracic Extensions (CTO)
M00-M99 DISEASES OF THE MUSCULOSKELETAL SYSTEM AND CONNECTIVE TISSUE

Two or Four Poster with Thoracic Extensions (CTO)
S00-T98 INJURY, POISONING, AND CERTAIN OTHER CONSEQUENCES OF EXTERNAL CAUSES



PROCEDURAL CONCERNS

Corsets (Flexible Spinal Orthosis)
J00-J99 DISEASES OF THE RESPIRATORY SYSTEM

L00-L99 DISEASES OF THE SKIN AND SUBCUTANEOUS TISSUE

M00-M99 DISEASES OF THE MUSCULOSKELETAL SYSTEM AND CONNECTIVE TISSUE

S00-T98 INJURY, POISONING, AND CERTAIN OTHER CONSEQUENCES OF EXTERNAL CAUSES



Body Jackets
G00-G99 DISEASES OF THE NERVOUS SYSTEM







1 Tan JC. Practical manual of physical medicine and rehabilitation: diagnostics, therapeutics, and basic problems. St. Louis: Mosby, 1998.
2 Webster’s third new international dictionary. Springfield (MA: Merriam-Webster, 1981.
3 Linden CA, Trombly CA. Orthoses: kinds and purposes. In Trombly CA, editor: Occupational therapy for physical dysfunction, ed 4, Baltimore (MD): Williams & Wilkins, 1995.
4 Ryan MM, Darras BT, Soul JS. Peroneal neuropathy from ankle-foot orthosis. Pediatr Neurol. 2003;29(1):72-74.
5 Fischer AQ, Strasburger J. Footdrop in the neonate secondary to use of footboards. J Pediatr. 1982;101:1003-1004.
6 Weitz EM, Carson G. The anterior tibial compartment syndrome in a twenty month old infant. Bull Hosp Joint Dis. 1969;30(1):16-20.
7 Helm PA, Kevorkian CG, Lushbaugh M, et al. Burn injury: rehabilitation management in 1982. Arch Phys Med Rehab. 1982;63:6-16.
8 Malick MH. Manual on static hand splinting. Pittsburgh (PA): Harmarville Rehabilitation, 1980.
9 Cusick BD. Progressive casting and splinting for lower extremity deformities in children with neuromuscular dysfunction. Tucson (AZ): Therapy Skill Builders, 1990.
10 Miner LJ, Nelson VS. Upper limb orthoses. In: Redford JB, Basmajian JV, Trautman P, editors. Orthotics: clinical practice and rehabilitation technology. New York: Churchill-Livingstone, 1995.
11 Gryboski JD, Kocoshis SA, Seashore JH, et al. “Body-brace” oesophagitis, a complication of kyphoscoliosis therapy. Lancet. 1978;2(8087):449-451.
12 Kling TF, Drennan JC, Gryboski JD. Esophagitis complicating scoliosis management with the Boston thoracolumbosacral orthosis. Clin Orthop Rel Res. 1981;159:208-210.
13 Liew SC, Hill DA. Complication of hard cervical collars in multi-trauma patient. Aust N Z J Surg. 1994;64(2):139-140.
14 Bussell M, Merritt J, Fenwick L. Spinal orthoses. In: Redford JB, Basmajian JV, Trautman P, editors. Orthotics: Clinical practice and rehabilitation technology. New York: Churchill-Livingstone, 1995.
15 Pomerantz F, Durand E. Spinal orthosis. Delisa JA, editor. Physical medicine and rehabilitation: principles and practice, vol 2. Philadelphia: Lippincott Williams & Wilkins, 2005.
16 Johnson EW, Alexander MA, Koenig WC. Infantile Erb’s palsy (Smellie’s palsy). Arch Phys Med Rehab. 1977;58(4):175-178.