Intestinal Obstruction
Mechanical obstruction of the bowel may be simple (one-point obstruction) or closed loop (obstruction at two points enclosing a segment of bowel). If the bowel is viable, the obstruction is termed non-strangulating. If the arterial blood supply is compromised, strangulating obstruction occurs with subsequent infarction of the bowel. Intestinal obstruction is a common surgical emergency.
History
Small bowel
Central abdominal colicky pain. Vomiting – food, bile, faeculent, depending upon the level of obstruction. Distension – degree depends on level of obstruction. There may be very little distension with high small bowel obstruction. It may be gross with low small bowel obstruction. Constipation. There may be a history of abdominal surgery to suggest adhesive obstruction. The patient may be aware of a hernia.
Large bowel
Central (right colon to two-thirds of the way along the transverse colon) or lower abdominal colicky pain (remainder of the colon). Constipation. Vomiting is a late feature with large bowel obstruction. Abdominal distension. There may be a previous history of change in bowel habit and bleeding PR to suggest carcinoma. A long history of constipation (years) and abdominal distension suggest Hirschsprung’s disease. Development of a constant severe pain suggests infarction.
Adynamic obstruction
Carefully check the drug history. Patients on anticoagulants may have retroperitoneal haemorrhage. Precipitating cause may be obvious, e.g. recent surgery or spinal fracture. The abdominal distension may be painless but uncomfortable. Vomiting, constipation. The elderly immobilised in bed are especially vulnerable.
Examination
Small bowel
Observe for scars. Exclude obstructed incisional hernia. Check hernial orifices. It is easy to miss a small femoral hernia in an obese patient. Distended tympanitic abdomen usually non-tender. High-pitched tinkling obstructed bowel sounds. Pyrexia, tachycardia and localised tenderness suggest impending infarction. A palpable mass in the right iliac fossa may suggest Crohn’s disease or caecal carcinoma (obstructing the ileocaecal valve and causing small bowel obstruction). Carry out a digital rectal examination.
Large bowel
Distended tympanitic abdomen, which may be very tense. Obstructed bowel sounds. Rectum may be empty on examination PR unless obstruction is due to faecal impaction. A mass may be palpable to suggest an obstructing carcinoma. A palpable, tense, tender caecum suggests closed loop obstruction with a competent ileocaecal valve. Caecal perforation may be imminent.
Adynamic obstruction
Abdominal distension. Tense tympanitic abdomen. Absent bowel sounds. Evidence of previous surgery, trauma, retroperitoneal haemorrhage and peritonitis, fractures.
General Investigations
■ Hb, FBC
Hb ↓ malignancy. WCC ↑ infection, infarcted bowel.
■ U&Es and creatinine
Dehydration. Hypokalaemia leading to paralytic ileus.
■ Clotting screen
May be abnormal with retroperitoneal haemorrhage, especially if patient on anticoagulants.
■ AXR
Distended loops of bowel in central abdomen. Proximal small bowel shows lines closely together completely crossing the lumen of the bowel (valvulae conniventes) (Fig. 36). These get progressively further apart until there are none seen in the terminal ileum. Gas in the biliary tree (gallstone ileus). Large bowel obstruction – distended bowel with air-fluid levels at the periphery of the abdomen. Sigmoid volvulus – distended loop of bowel, the shape of a ‘coffee bean’, arising out of the pelvis on the left side.
■ Sigmoidoscopy
Tumour at rectosigmoid. Sigmoid volvulus may be decompressed by careful insertion of sigmoidoscope. Biopsy – carcinoma, absence of ganglion cells in Hirschsprung’s disease.
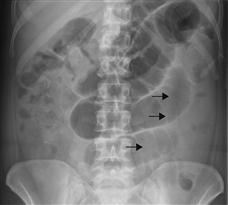
Figure 36 Small bowel obstruction.
Distended loops of small bowel are visible in the central abdomen. These are identifiable as small bowel as the valvulae conniventes (arrows) cross the entire lumen of the bowel.



