8
Normal Anatomy and Flow During the Complete Examination
Epiaortic Imaging
 Introduction
Introduction
Epiaortic ultrasound (EAU) is an imaging modality whereby a handheld transducer is placed directly upon a surgically exposed aorta. EAU provides high-quality sonographic data depicting aortic anatomy and pathology. The use of ultrasound imaging directly applied to the surgical field predates the introduction of intraoperative transesophageal echocardiography (TEE).1,2 Epicardial ultrasound was used in the 1980s at The Mount Sinai Medical Center and at Columbia University College of Physicians and Surgeons in New York City to assess left ventricular function, 3 myocardial perfusion, 4 the presence of intracardiac air, 5 and mitral valve function after mitral valve repair. 6 In addition to epicardial ultrasound, EAU is a useful tool in the echocardiographer’s armamentarium to address clinical situations such as evaluating a diseased aorta in the face of aortic manipulation or instrumentation.
The most recent guidelines by the American Society of Echocardiography (ASE) and the Society of Cardiovascular Anesthesiologists (SCA) recommend five standard views. 7 Its ease of use, minimal time to perform, negligible complication rate, and high accuracy has made EAU an appealing tool. The guidelines recommend its use in patients at high risk for embolic events, but also speculated on more widespread use of EAU, given its favorable risk/benefit ratio.
 Indications
Indications
The initial impetus for the use of EAU stemmed from attempts to reduce the rate of perioperative stroke during cardiac surgery. The 2008 ASE/SCA guidelines for comprehensive intraoperative ultrasonographic examination recommend the use of EAU in patients with increased risk for embolic stroke, history of cerebrovascular disease, peripheral vascular disease, and patients in whom other imaging modalities demonstrate the presence of aortic atherosclerotic disease. 7 Risk factors for stroke in cardiac surgery include advanced age, female gender, proximal aortic atherosclerosis, calcified aorta, history of cerebrovascular disease, peripheral vascular disease, diabetes, hypertension, prior cardiac surgery, preoperative infection (including endocarditis), urgent surgery, greater than 2-hour cardiopulmonary bypass (CPB) time, intraoperative hemofiltration, and transfusion. EAU can identify diseased aortic segments containing atherosclerotic plaque, calcification, or thrombus that are at high risk for distal embolization. 8 Once these areas are identified, the surgical approach to the aorta may be altered or aborted to reduce this risk. 9 In addition to possible alterations in surgical strategy, the examination can provide information for stratification of a patient’s risk of complication from distal embolization.
 Stroke
Stroke
Stroke (cerebrovascular accident) is a potentially devastating complication of an otherwise successful cardiac operation. Although there are many types of cerebral injury after CPB, such as transient ischemic attack, delirium, and cognitive dysfunction, this chapter will focus on stroke. Stroke is defined by the World Health Organization as a “neurological deficit of cerebrovascular cause that persists beyond 24 hours or is interrupted by death within 24 hours.” Neurologic complications are the second most common causes of morbidity and mortality after cardiac surgery, second only to heart failure. Stroke can lead to delayed discharge from a long-term care facility, increased hospital stay, and increased mortality.10,11 The incidence of perioperative stroke varies in the literature, based on study design and the population examined.12–14 The stroke rate clearly increases with age, cardiovascular comorbidities, CPB time, and the complexity of the operation. In a published review of the Society of Thoracic Surgeons (STS) database from 2002 to 2006 examining over 700,000 CABG operations and over 100,000 mitral valve surgeries, the stroke rates were most common in combined mitral valve and coronary artery bypass grafting (CABG) and least common in isolated CABG ( Table 8-1).15–17
TABLE 8-1
Society of Thoracic Surgeons Stroke Rates for Coronary Artery Bypass Graft and Valve Surgery (2002-2006) ∗

∗Stroke rates as described by 2002-2006 Society of Thoracic Surgeons database. Most frequent cohort of patients to suffer stroke is the group that received mitral valve and coronary artery bypass graft (CABG) surgery. Smallest stroke risk was in the isolated CABG surgery group.
Data from Shahian DM, et al. The Society of Thoracic Surgeons 2008 cardiac surgery risk models: part 1—coronary artery bypass grafting surgery. Ann Thorac Surg. 2009;88:S2; O’Brien SM, et al. The Society of Thoracic Surgeons 2008 cardiac surgery risk models: part 2—isolated valve surgery. Ann Thorac Surg. 2009;88:S23; Shahian DM, et al. The Society of Thoracic Surgeons 2008 cardiac surgery risk models: part 3—valve plus coronary artery bypass graft surgery. Ann Thorac Surg. 2009;88:S43.
Additional risk factors are similar to those encountered for stroke in the general population. These include prior stroke, diabetes, female gender, renal failure, hypertension, atrial fibrillation, peripheral vascular disease, and others.18–22 Most relevant for our discussion is the risk of stroke conferred by severe atherosclerotic disease of the thoracic aorta, as screened by ultrasound as discussed earlier. Although there has been controversy regarding the importance of aortic atherosclerosis as a risk factor for primary strokes in the general population,23–34 it has now been strongly established in the cardiac surgery population that aortic plaque correlates with postoperative stroke incidence.9,35–42 The more extensive and complex the plaque burden, the higher the risk of postoperative stroke.
Possible mechanisms of stroke include arterial-to-arterial embolization of plaque or thrombus, embolization from intracardiac sources, or paradoxical embolization from venous to arterial circulations across intra- or extracardiac shunts.43–48 Other etiologic pathways include in situ arterial thrombosis that leads to critical obstruction of brain perfusion, as well as a low-flow state causing ischemic injury due to hypotension and reduced cardiac output. Air entrainment from open cardiovascular structures has been implicated in both stroke and more subtle neurologic impairments after cardiac surgery. 49 Stroke may also be caused by cerebral hemorrhage, decreased cerebral venous drainage, and as a sequela of prolonged seizure activity. Based on radiographic studies, it appears that embolization to the cerebral arterial system is the most common cause of stroke after cardiac surgery.50,51
Three common types of matter that embolize to cause neurologic injury are cholesterol-laden atheromas, particles of embolized thrombus, and entrained air. It is likely that the larger the embolic particle and the more frequent the occurrence of embolic events, the greater the risk and severity of neurologic injury.52,53 It is also thought that low-flow states augment the ischemic injury from embolized particles by failing to “wash out” the cerebral circulation of these obstructing particles.54–56
During cardiac surgery, the aorta is manipulated in several ways that may lead to plaque disruption and embolization. These include aortic clamp placement and removal, insertion of the aortic cannula, the antegrade cardioplegia vent, the proximal anastomosis of coronary grafts, as well as the aortotomy itself. Flow from the aortic cannula while on CPB may cause a “sandblasting effect” that may disrupt plaque downstream from the cannula.57,58
Several methods are used to detect and characterize the patient’s atheromatous burden within the ascending aorta. Preoperatively, plaque and calcification may be detected by means of radiologic scanning with computed tomography (CT) or magnetic resonance imaging (MRI). Intraoperatively, three methods are currently employed: direct surgical palpation of the aorta to feel for the hardness of calcification, TEE, and EAU. Several studies clearly demonstrate the superiority of TEE and EAU over surgical palpation. Surgical palpation is much less sensitive than ultrasound, considerably underestimating the atherosclerotic burden; EAU has the greatest sensitivity.59–67 In one study, Linden et al. examined 921 consecutive cardiac surgery patients. EAU revealed that 26% had plaque on the ascending aorta measuring more than 5 mm thick, but surgical palpation only detected 40% of these lesions. 30 Calcified areas the surgeon is able to feel may be stable plaques with a lower risk for embolization than the soft atheromas that may only be detectable by ultrasound. 68
Although the TEE probe may already be in place and its use does not interrupt the surgical flow, EAU offers several advantages over TEE for characterizing aortic plaque. Most surgical manipulation occurs in the region of the ascending aorta considered to be the “blind spot” of TEE. This is where the trachea and left mainstem bronchus interpose between the esophagus and aorta, causing disruption of ultrasound transmission. Thus, although parts of the ascending aorta can be visualized by TEE, 69 Konstadt et al. have shown that TEE is frequently unable to image the region of greatest interest of the ascending aorta. 70 Since EAU is placed closer to the area of interest, enabling higher transducer frequencies to be used, higher-quality images with fewer artifacts are possible.
Well-designed trials demonstrating a morbidity or mortality benefit to EAU are lacking, but an accumulating body of data indicates that in high-risk patients the use of EAU alters surgical management and that these changes may be beneficial.56,71–78 Some examples of modifications of surgical technique are off-pump (as opposed to on-pump) CABG, “no-touch” techniques, and alterations in the site of aortic manipulation and instrumentation (e.g., axillary cannulation).79–82 More radical surgical approaches may include aortic endarterectomy or aortic arch replacement, although these approaches may produce worse outcomes. 83
 Probes and Technique
Probes and Technique
The linear probe scans both the anterior aortic wall (near field) and the posterior aortic wall (far field) without the need for a transducer standoff. One drawback is that linear probes tend to have a large “footprint,” which refers to the large surface area of the probe itself. Thus, a linear probe may be difficult to maneuver in a small surgical field. Second, the entire left-to-right dimensions of the aorta may not fit in a single ultrasonographic window, creating a “tunneled” view, and the transducer may have to be repositioned rightward and leftward to acquire the entire cross-sectional picture of the aorta ( Fig. 8-1).
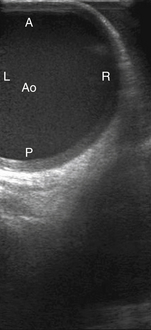
Figure 8-1 Epiaortic ultrasound image of tubular ascending aorta (Ao) using linear probe. A, Anterior; L, left lateral wall; P, posterior; R, right lateral wall.
The wedge-shaped images of the phased and matrix array transducers enable simultaneous imaging of the right and left aortic walls, and they also tend to have a smaller footprint, enabling greater maneuverability within the surgical field. The drawback of phased or matrix array transducers is the need for a standoff. Because of the wedge shape of the image, if the transducer is placed directly on the aorta, the anterior aortic wall (near field) will not be completely imaged; only a small section will be displayed while the rest will be outside the sector. To capture the near field in its entirety, the transducer is held at some distance away from the aorta (the standoff) ( Fig. 8-2). This requires addition of a medium that conducts ultrasound waves. Air cannot be used because it is a poor acoustic conductor. The standoff may be provided by a gel that can either be purchased as a pad or as gel already incorporated into the sterile cover wrapping surrounding the transducer tip. Another simple approach is to fill the sterile condom sheath with a column of saline, enabling the transducer to be held away from the aorta while transmitting ultrasound waves though the saline to the aorta. At our institution, we place sterile gel within the sterile sheath, fill the pericardial well with warm sterile saline, and hold the transducer immersed in the saline at a distance from the aortic wall so that the anterior wall of the aorta can be visualized in its entirety.
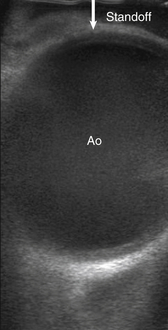
Figure 8-2 Epiaortic ultrasound of ascending aorta (Ao) with “standoff,” the distance held off image being interrogated by probe.
It is of great importance to maintain sterility when introducing the handheld transducer onto the surgical field. The probe is passed from the nonsterile area into a sterile condom sheath on the surgical field. Some institutions place a double sheath, exercising extra precaution. At our institution, we disinfect the transducers between cases and pass these probes into a sterile sheath from the field. It is important to note that different manufacturers recommend specific disinfection techniques for their probes; one must check with the manufacturer to identify the appropriate cleaning technique (see Chapter 29).
 Imaging Planes
Imaging Planes
The ascending aorta and arch should be systematically scanned throughout their entirety, paying particular attention to the sites of proposed aortic manipulation. Several papers have proposed standardized schemes for aortic scanning.7,84,85 To complete a comprehensive EAU examination from the sinotubular junction to the innominate artery and aortic arch, a minimum of five views are recommended. Usually, TEE allows for visualization of the proximal ascending aorta and distal aortic arch. 86
The ascending aorta should be evaluated in short and long axis in each of the proximal, mid-, and distal segments. In short axis with the ultrasound probe perpendicular to the aorta, the aorta should be measured from the near-field inner edge to the far-field inner edge of the aorta in each segment. Manipulation of the probe in perpendicular orientation as the probe is moved from proximal to distal allows for evaluation of all three portions of the ascending aorta. The proximal ascending aorta is demarcated by the beginning of the sinotubular junction, where it is common to see the aortic valve and right pulmonary artery. The mid–ascending aorta is defined by the part of the aorta that is juxtaposed with the right pulmonary artery ( Fig. 8-3). The distal ascending aorta is from the distal right pulmonary artery to the innominate artery. Movement farther distally will allow for examination of the proximal aortic arch, which is necessary if not clearly seen on TEE ( Fig. 8-4).

Figure 8-3 Left, Epiaortic ultrasound (EAU) using linear probe of mid–ascending aorta (Ao) in short axis. Right, EAU using linear probe of mid–ascending aorta (Ao) in long axis. A, Anterior wall of aorta; L, left lateral wall of aorta; P, posterior wall of aorta; R, right lateral wall of aorta; RPA, right pulmonary artery; SVC, superior vena cava.
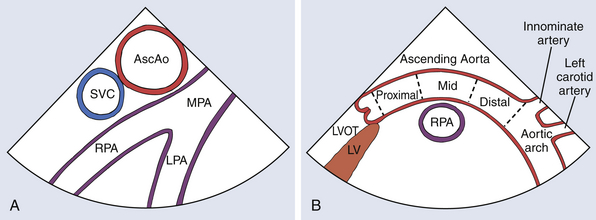
Figure 8-4 Epiaortic ultrasound diagram of short-axis view (A) and long-axis view (B) of ascending aorta (AscAo) and surrounding structures. LPA, Left pulmonary artery; LV, left ventricle; LVOT, left ventricular outflow tract; MPA, main pulmonary artery; RPA, right pulmonary artery; SVC, superior vena cava.
The long-axis views are obtained at 90 degrees from the short-axis views, in plane with the direction of blood flow within the ascending aorta. The proximal long-axis view should provide visualization of the sinus of Valsalva, sinotubular junction, and aortic valve. Continuation of the examination distally allows for examination of the mid–ascending aorta. Finally, the distal ascending aorta includes locating the innominate artery. The aortic arch, with origins of the left common carotid and left subclavian artery, should be located as a final part of the examination (see Fig. 8-4, B).
During the examination, atherosclerotic grading and diameter measurements should be performed. Particular attention should be paid to regions of the aorta likely to be manipulated by the surgeon. Abnormal pathology at risk for embolization (e.g., areas of atherosclerosis, mobile plaque, ulcerated plaque) should be communicated to the surgeon, which may alter the surgical plan. Other aortic pathology such as dissection flaps and intramural hematoma should be ruled out and, if present, communicated as well. Video clips and still images of the complete examination should be stored for future referral as dictated by institutional protocol.
 Atherosclerotic Plaque Grading
Atherosclerotic Plaque Grading
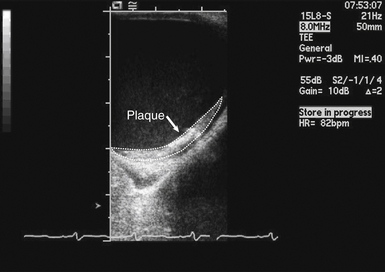
It is useful to have a grading system for atherosclerotic plaques that conveys plaque severity and extent of aortic disease. Having a standardized grading system offers several advantages. First, it provides a common language that can be understood across disciplines to accurately describe disease. This allows practitioners to clearly communicate informed decisions on how to best proceed with aortic manipulation or to argue against any manipulation at all. Second, it provides a descriptive platform of categorization for research purposes. Unfortunately, there is no current consensus on which grading system should be employed. The ASE/SCA guidelines for EAU examination list eight of many potential grading systems, which range in complexity from a two-grade scale up to a five-grade scale; all have much in common. They emerged from the use of grading in studies attempting to correlate plaque features with stroke risk. Some studies examined the perioperative period of cardiac surgery while others looked at the general stroke population. A scale may include a grade for a normal aorta or a minimally diseased low-risk aorta. Most scales define a size cutoff that defines a larger protruding plaque that indicates a substantially higher risk of stroke; this size definition has varied among different studies. Plaques with 5-mm-thick focal hyperechoic regions of the aortic layers intima to media and/or lesions with ulcerations, mobile structures, or lumen irregularities are defined as high-risk plaques. 87 In all studies, regardless of which size was used, the larger plaques above the cutoff were associated with higher stroke rates. The highest-risk lesions were “complex plaques,” features of which include ulcerations, heavy calcifications, adherent thrombus, and any plaque with a mobile component. Our institution uses the five-point grading system described by Katz et al. ( Table 8-2). However, until any one grading system is shown to be superior, any grading system is acceptable assuming it relates the important risk factors for plaques ( Fig. 8-5).
TABLE 8-2
Katz Grading System for Aortic Atheroma
| Grade | Description |
| 1 | Normal aorta to mild intimal thickening |
| 2 | Severe intimal thickening without protruding atheroma |
| 3 | Protruding atheroma <5 mm into lumen |
| 4 | Protruding atheroma ≥5 mm into lumen |
| 5 | Mobile atheroma |
From Katz ES, Tunick PA, Rusinek H, Ribakove G, Spencer FC, Kronzon I. Protruding aortic atheromas predict stroke in elderly patients undergoing cardiopulmonary bypass: experience with intraoperative transesophageal echocardiography. J Am Coll Cardiol. 1992;20:70-7.
Investigation into the use of various alternative descriptive means of classifying aortic atherosclerotic burden has been undertaken. One paper looked at the image frame in each segment with the greatest burden of atherosclerotic disease. They compared the plaque area by planimetry to the total aortic cross-sectional area. They then calculated the ratio of the two areas as an indicator of atherosclerotic burden. 88 Other groups have studied plaque echodensity through postprocessing analysis, attempting to discern its histopathology as fatty, fibrous, or calcific, followed by correlating their findings with thromboembolic outcomes.89,90 With the introduction of live three-dimensional (3D) ultrasound probes, there is potential to evaluate the true extent of atherosclerotic disease.91,92
 Normal Dimensions
Normal Dimensions
Normal ascending aortic dimensions have been obtained from a compilation of data across gender, body surface area, height, and age. These dimensions are measured by MRI, CT, helical CT, invasive angiography, and echocardiography.93–97Although some papers show no association, most studies have found ascending aorta diameter to increase with increasing age.93–97 The Framingham Heart Study showed that age was the most important determinant in aortic root size in men and women. This study found a cumulative aortic root measurement to vary widely with age, gender, and body size of individuals.97–100
According to the ASE recommendations for chamber quantification, the ascending aorta should be examined with two-dimensional (2D) echocardiography using four measurements. 101 These recommendations were written for TEE and transthoracic echocardiography, but they are applicable to epiaortic echocardiography as well. Although some clinicians use inner edge–to–inner edge techniques, normative data for echocardiography were obtained using leading edge to leading edge and thus should be favored. Measurements that should be taken are the aortic valve annulus, sinus of Valsalva, and sinotubular junction. A short-axis dimension of the ascending aorta may be useful for surgical planning as well. The measurement should be taken at the largest diameter, that is, during systole and as perpendicular to the aorta as possible. Biaggi et al. used echocardiography to determine normal ascending aortic dimensions in 64,686 patients. Using the leading edge–to–leading edge technique acquired at end-systole, the mean sinus of Valsalva measurement was 3.4 cm in men and 3.1 cm in women. The mean ascending aortic values using the right pulmonary artery as a landmark were 3.2 cm for men and 3.0 cm for women. 96 The aortic annulus is normally 2.2 cm in diameter ( Fig. 8-6). 102
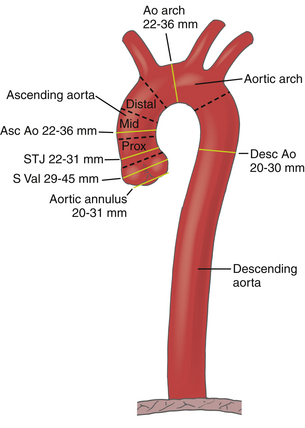
Figure 8-6 Diagram of normal aortic anatomy and dimensions from aortic valve to diaphragm. Ascending aorta (Asc Ao) is divided into three segments: proximal ascending aorta is from sinus of Valsalva (S Val) to pulmonary artery, mid–ascending aorta is demarcated by the part of aorta adjacent to pulmonary artery, distal ascending aorta is from pulmonary artery to innominate artery. Aortic arch (Ao arch) is from innominate artery to left subclavian artery, and descending aorta (Desc Ao) extends distal to subclavian artery to iliac bifurcation below diaphragm. Relevant dimensions provided on diagram. STJ, Sinotubular junction.
Aortic root dilation at the sinuses of Valsalva is defined by an aortic root diameter greater than the 95% confidence interval based on body surface area by age ( Fig. 8-7). 97 Roman et al. looked at 135 normal adults and found the absolute upper limits of normal for the sinus of Valsalva to be 4.0 cm for men and 3.6 cm for women, and the supraaortic ridge was 3.5 cm for men and 3.2 cm for women. A leading edge–to–leading edge technique at end-diastole was used. 97
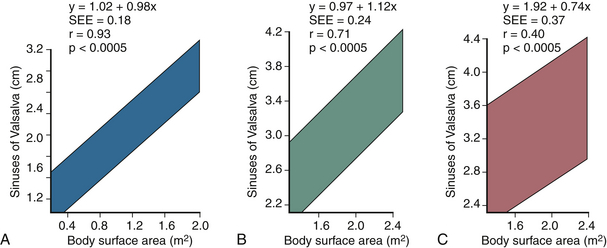
Figure 8-7 The 95% confidence interval to signify sinus of Valsalva dilation in (A) children and adolescents, (B) adults aged 20 to 39 years, and (C) adults aged 40 years or older. Figure depicts relationship of sinus of Valsalva to body surface area and age. (From Lang RM, Bierig M, Devereux RV, et al. Recommendations for chamber quantification: a report from the American Society of Echocardiography’s Guidelines and Standards Committee and the Chamber Quantification Writing Group, developed in conjunction with the European Association of Echocardiography, a branch of the European Society of Cardiology. J Am Soc Echocardiogr. 2005;18:1440-1463.)
 Doppler Interrogation of Ascending Aorta and Aortic Valve
Doppler Interrogation of Ascending Aorta and Aortic Valve
Use of EAU for Doppler interrogation of the aortic valve is limited. In some cases, color Doppler may be useful to diagnose the presence or absence of dissections and hematomas. 103 EAU has been used to guide aortic cannulation of patients with type A aortic dissections. In these cases, use of 2D EAU and color Doppler EAU helped identify true and false channels for successful arterial cannulation of the true lumen.104,105 One case report described the use of EAU to measure the gradient across a stenotic aortic valve when the Doppler insonation angle was unacceptable using TEE. 106
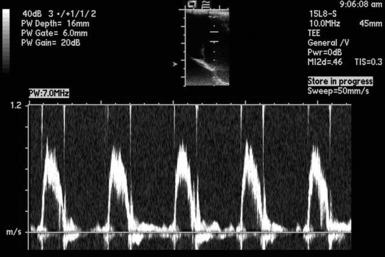
There are currently no guidelines recommending how to perform an EAU Doppler exam. It is difficult to obtain Doppler beam orientation parallel to aortic flow in many parts of the ascending aorta, because more frequently than not, the orientation of the ultrasound probe to flow in the aorta will be perpendicular ( Fig. 8-8). One must be careful to recognize that there is an element of error when the Doppler beam is not parallel to the direction of flow. The angle between the Doppler beam and the direction of flow within the aorta is called the insonation angle. It should be less than 30 degrees to maintain an error less than 15%.
 Summary
SummaryReferences
1. Wild, J. J., Crawford, H. D., Reid, J. M. Visualization of the excised human heart by means of reflected ultrasound of echography; preliminary report. Am Heart J. 1957; 54:903–906.
2. Johnson, M. L., Holmes, J. H., Spangler, R. D., Paton, B. C. Usefulness of echocardiography in patients undergoing mitral valve surgery. J Thorac Cardiovasc Surg. 1972; 64:922–934.
3. Dubroff, J. M., Wong, C. Y., et al. Left ventricular ejection fraction during cardiac surgery: A two-dimensional echocardiographic study. Circulation. 1983; 68:95–103.
4. Goldman, M. E., Mindich, B. P. Intraoperative cardioplegic contrast echocardiography for assessing myocardial perfusion during open heart surgery. J Am Coll Cardiol. 1984; 4:1029–1034.
5. Rodigas, P. C., Meyer, F. J., Haasler, G. B., et al. Intraoperative 2-dimensional echocardiography: ejection of microbubbles from the left ventricle after cardiac surgery. Am J Cardiol. 1982; 50:1130–1132.
6. Goldman, M. E., Mindich, B. P., Teichholz, L. E., et al. Intraoperative contrast echocardiography to evaluate mitral valve operations. J Am Coll Cardiol. 1984; 4:1035–1040.
7. Glas, K. E., et al. Guidelines for the performance of a comprehensive intraoperative epiaortic ultrasonographic examination: recommendations of the American Society of Echocardiography and the Society of Cardiovascular Anesthesiologists; endorsed by the Society of Thoracic Surgeons. J Am Soc Echocardiogr. 2007; 20:1227–1235.
8. Bucerius, J., Gummert, J. F., Borger, M. A., et al. Stroke after cardiac surgery: a risk factor analysis of 16. 184 consecutive adult patients. Ann Thorac Surg. 2003; 75:472–478.
9. Djaiai, G., Ali, M., Borger, M. A., et al. Epiaortic scanning modified planned intraoperative surgical management but not cerebral embolic load during coronary artery bypass surgery. Anesth Analg. 2008; 106:1611–1618.
10. Roach, G. W., Kanchuger, M., Mangano, C. M., et al. Adverse cerebral outcomes after coronary bypass surgery. N Engl J Med. 1996; 335:1857–1863.
11. McKhann, G. M., et al. Encephalopathy and stroke after coronary artery bypass grafting; incidence, consequences, and prediction. Arch Neurol. 2002; 59:1422–1428.
12. Anyanwu, A. C., Filsoufi, F., Salzberg, S. P., Bronster, D. J., Adams, D. H. Epidemiology of stroke after cardiac surgery in the current era. J Thorac Cardiovasc Surg. 2007; 134:1121–1127.
13. Coffey, C. E., Massey, E. W., Roberts, K. B., Curtis, S., Jones, R. H., Pryor, D. B. Natural history of cerebral complications of coronary artery bypass graft surgery. Neurology. 1983; 33(11):1416–1421.
14. Breuer, A. C., et al. Central nervous system complications of coronary artery bypass graft surgery: prospective analysis of 421 patients. Stroke. 1983; 14(5):682–687.
15. Shahian, D. M., et al. The Society of Thoracic Surgeons 2008 cardiac surgery risk models: part 1–coronary artery bypass grafting surgery. Ann Thorac Surg. 2009; 88:S2.
16. O’Brien, S. M., et al. The Society of Thoracic Surgeons 2008 cardiac surgery risk models: part 2–isolated valve surgery. Ann Thorac Surg. 2009; 88:S23.
17. Shahian, D. M., et al. The Society of Thoracic Surgeons 2008 cardiac surgery risk models: part 3–valve plus coronary artery bypass graft surgery. Ann Thorac Surg. 2009; 88:S43.
18. Stamou, S. C., Hill, P. C., Dangas, G., et al. Stroke after coronary artery bypass; incidence, predictors, and clinical outcomes. Stroke. 2001; 32:1508–1513.
19. Hogue, C. W., Jr., Barzilai, B., Pieper, K. S., et al. Sex differences in neurological outcomes and mortality after cardiac surgery; a Society of Thoracic Surgery National Database report. Circulation. 2001; 103:2133–2137.
20. Charlesworth, D. C., Likosky, D. S., Marrin, C. A. S., et al. Development and validation of a prediction model for strokes after coronary artery bypass grafting. Ann Thorac Surg. 2003; 76:436–443.
21. Puskas, J. D., Winston, A. D., Wright, C. E. Stroke after coronary artery operation: incidence, correlates, outcome, and cost. Ann Thorac Surg. 2000; 69:1053–1056.
22. McKhann, G. M., Goldsborough, M. A., Borowicz, L. M., Jr. Predictors of stroke risk in coronary artery bypass patients. Ann Thorac Surgery. 1997; 63:516–521.
23. Amarenco, P., Duyckaerts, C., Tzourio, C., Henin, D., Bousser, M. G., Hauw, J. J. The prevalence of ulcerated plaques in the aortic arch in patients with stroke. N Engl J Med. 1992; 326:221–225.
24. Amarenco, P., Cohen, A., Tzourio, C., et al. Atherosclerotic disease of the aortic arch and the risk of ischemic stroke. N Engl J Med. 1994; 331:1474–1479.
25. Amarenco, P., Hienzlef, O., Lucas, C., et al. The French Study of the Aortic Plaques in Stroke Group. Atherosclerotic disease of the aortic arch as a risk factor for recurrent ischemic stroke. N Engl J Med. 1996; 334:1216–1221.
26. Di Tullio, M. R., Russo, C., Jin, Z., Sacco, R. L., Mohr, J. P., Homma, S. Aortic arch plaques and risk of recurrent stroke and death. Circulation. 2009; 119:2376–2382.
27. Tunick, P. A., Perez, J. L., Kronzon, I. Protruding atheromas in the thoracic aorta and systemic embolization. Ann Intern Med. 1991; 115:423–427.
28. Karalis, D. G., Chandrasekaran, K., Victor, M. F., Ross, J. J., Mintz, G. S. Recognition and embolic potential of intraaortic atherosclerotic debris. J Am Coll Cardiol. 1991; 17:73–78.
29. Tunick, P. A., Rosenzweig, B. P., Katz, E. S., Freedberg, R. S., Perez, J. L., Kronzon, I. High risk for vascular events in patients with protruding aortic atheromas: a prospective study. J Am Coll Cardiol. 1994; 23:1085–1090.
30. Ferrari, E., Vidal, R., Chevallier, T., Baudouy, M. Atherosclerosis of the aorta and aortic debris as a marker of poor prognosis: benefit of oral anticoagulants. J Am Coll Cardiol. 1999; 33:1317–1322.
31. Tunick, P. A., Ambika, C. N., Goodkin, G. M., et al. Effect of treatment on the incidence of stroke and other emboli in 519 patients with severe thoracic aortic plaque. Am J Cardiol. 2002; 90:1320–1325.
32. Russo, C. Kin z, Rundek T, Homma S, Sacco RL, Di Tullio MR. Atherosclerotic Disease of the Proximal Aorta and the Risk of Vascular Events in a Population-Based Cohort; The Aortic Plaques and Risk of Ischemic Stroke (APRIS) Study. Stroke. 2009; 40:2313–2318.
33. Petty, G. W., Khandheria, B. K., Meissner, I., et al. Population-Based Study of the Relationship Between Atherosclerotic Aortic Debris and Cerebrovascular Ischemic Events. Mayo Clin Proc. 2006; 81(5):609–614.
34. Meissner, I., Khandheria, B. K., Sheps, S. G., et al. Atherosclerosis of the Aorta: Risk Factor, Risk Marker, or Innocent Bystander; A Prospective Population-Based Transesophageal Echocardiography Study. J Am Coll Cardiol. 2004; 44:1018–1024.
35. Wolman, R. L., Nussmeier, N. A., Aggarwal, A., et al. Cerebral Injury after Cardiac Surgery; Identification of a Group at Extraordinary Risk. Stroke. 1999; 30:514–522.
36. Hartman, G. S., Yao, F. S. F., Bruefach, M., III., et al. Severity of Aortic Atheromatous Disease Diagnosed by Transesophageal Echocardiography Predicts Stroke and Other Outcomes Associated With Coronary Artery Surgery: A prospective Study. Anesth Analg. 1996; 83:701–708.
37. Linden, J. V. D., Hadjinikolaou, L., Bergman, P., Lindblom, D. Postoperative Stroke in Cardiac Surgery Is Related to the Location and Extent of Atherosclerotic Disease in the Ascending Aorta. J Am Coll Cardiol. 2001; 38:131–135.
38. Katz, E. S., Tunick, P. A., Rusinek, H., Ribakove, G., Spencer, F. C., Kronzon, I. Protruding Aortic Atheromas Predict Stroke in Elderly Patient’s Undergoing Cardiopulmonary Bypass: Experience With Intraoperative Transesophageal Echocardiography. J Am Coll Cardiol. 1992; 20:70–77.
39. Davila-Roman, V. G., Murphy, S. F., Nickerson, N. J., Kouchoukos, N. T., Schechtman, K. B., Barzilai, B. Atherosclerosis of the Ascending Aorta Is an Independent Predictor of Long-Tern Neurologic Events and Mortality. J Am Coll Cardiol. 1999; 33:1308–1316.
40. John, R., Choudhri, A. F., Weinberg, A. D. Ting w, Rose EAU, Smith CR, OZ MC. Multicenter Review of Preoperative Risk Factors for Stroke After Coronary Bypass Grafting. Ann Thorac Surg. 2000; 69:30–36.
41. Hogue, C. W., Jr., Murphy, S. F., Schechtman, K. B., Davila-Roman, V. G. Risk Factors For Early Or Delayed Stroke After Cardiac Surgery. Circulation. 1999; 100:642–647.
42. Gardner, T. J., Horneffer, P. J., Manolio, T. A., et al. Stroke following coronary artery bypass grafting: a ten-year study. Ann Thorac Surg. 1985; 40(6):574–581.
43. Doty, J. R., Wilentz, R. E., Salazar, J. D., Hruban, R. H., Cameron, D. E. Atheroembolism in Cardiac Surgery. Ann Thorac Surg. 2003; 75(4):1221–1226.
44. Thurlbeck, W. M., Castleman, B. Atheromatous emboli to the kidneys after aortic surgery. N Engl J Med. 1957; 257(10):442–447.
45. Freedberg, R. S., Tunick, P. A., Kronzon, I. Emboli in transit: the missing link. J Am Soc Echocardiogr. 1998; 11(8):826–828.
46. Ezzeddine, M. A., Primavera, J. M., Rosand, J., Hedley-Whyte, E. T., Rordorf, G. Clinical characteristics of pathologically proved cholesterol emboli to the brain. Neurology. 2000; 54:1681–1683.
47. Cross, S. S. How common is cholesterol embolism? J Clin Pathol. 1991; 44:859–861.
48. Fukumoto, Y., Tsutsui, H., Tsuchihashi, M., Masunoto, A., Takeshita, A. Cholesterol Embolism Study (Chest) Investigators: The Incidence and Risk Factors of Cholesterol Embolization, A Complication of Cardiac Catheterization: A Prospective Study. J Am Coll Cardiol. 2003; 42:211–216.
49. Hammon, J. W., Jr., Stump, D. A., Kon, N. D., et al. Risk factors and Solutions for the Development of Neurobehavioral Changes after Coronary Bypass Grafting. Ann Thorac Surg. 1997; 63(6):1613–1618.
50. Ascione, R., Reeves, B. C., Chamberlain, M. H., Ghosh, A. K., Lim, K. H., Angelini, G. D. Predictors of Stroke in the Modern Era of Coronary Artery Bypass Grafting: A Case Control Study. Ann Thorac Surg. 2002; 74(2):474–480.
51. Likosky, D. S., Marrin, C. A. S., Caplan, L. R., et al. Determination of Etiologic Mechanism of Strokes Secondary to Coronary Artery Bypass Graft Surgery. Stroke. 2003; 34:2830–2834.
52. Blauth, C. I. Macroemboli and Microemboli During Cardiopulmonary Bypass. Ann Thorac Surg. 1995; 59:1300–1303.
53. Abu-Omar, Y., Balacumaraswami, L., Matthews, P. M., Taggart Solid, D. P., Cerebral, Gaseous. Microembolization during Off-Pump, On-Pump, and Open Cardiac Surgery Procedures. J Thorac Cardiovasc Surg. 2004; 127:1759–1765.
54. Schreiber, S., Serdaroglu, M., Schreiber, F., Skalej, M., Heinze, H. J., Goertler, M. Simultaneous Occurrence and Interaction of Hypoperfusion and Embolism in a Patient with Severe Middle Cerebral Artery Stenosis. Stroke. 2009; 40(7):e478–e480. [(epub)].
55. Sedlaczek, O., Caplan, L., Hennerici, M. Impaired Washout—Embolism and Ischemic Stroke: Further Examples and Proof of Concept. Cerebrovasc Dis. 2005; 19(6):396–401.
56. Caplan, L. R., Hennerici, M. Impaired Clearance of Emboli (Washout) is an Important Link Between Hypoperfusion, Embolism, and Ischemic Stroke. Arch Neurol. 1998; 55(11):1475–1482.
57. Swaminathan, M., Grocott, H. P., Mackensen, G. B., Podgoreanu, M. V., Glower, D. D., Matthew, J. P. The “Sandblasting Effect of Aortic Cannula on Arch Atheroma During Cardiopulmonary Bypass. Anesth Analg. 2007; 104(6):1350–1351.
58. Hamano, K., Ikeda, Y., Okada, H., et al. Atheromatous Plaque in the Distal Aortic Arch Creating the Potential for Cerebral Embolism During Cardiopulmonary bypass. Jpn Circ J. 2001; 65(3):161–164.
59. Mackensen, G. B., Ti, L. K., Phillips-Bute, B. G., et al. Cerebral embolization during cardiac surgery: Impact of aortic atheroma burden. Br J Anaesth. 2003; 91:656.
60. Sharony, R., Bizekis, C. S., Kanchuger, M., et al. Off-pump coronary artery bypass grafting reduces mortality and stroke in patients with atheromatous aortas: A case control study. Circulation. 9(suppl I), 2003. [II-115].
61. Arrowsmith, J. E., Grocott, H. P., Reves, J. G., et al. Central nervous system complications of cardiac surgery. Br J Anaesth. 2000; 84:378.
62. Davila-Roman, V. G., Phillips, K. J., Daily, B. B., Davila, R. M., Kouchoukos, N. T., Barzilai, B. Intraoperative Transesophageal Echocardiography and Epiaortic Ultrasound for Assessment of Atherosclerosis of the Thoracic Aorta. J Am Coll Cardiol. 1996; 28:942–947.
63. Marshall, W. G., Jr., Barzilai, B., Kouchoukos, N. T., Saffitz, J. Intraoperative Ultrasonic Imaging of the Ascending Aorta. Ann Thorac Surg. 1989; 48(3):339–344.
64. Royse, C., Royse, A., Blake, D., Grigg, L. Screening the Thoracic Aorta for Atheroma: A Comparison of Manual Palpation, Transesophageal and Epiaortic Ultrasonography. Ann Thorac Cardiovasc Surg. 1998; 4(6):347–350.
65. Ohteki, H., Itoh, T., Natsuaki, M., Minato, N., Suda, H. Intraoperative Ultrasonic Imaging of the Ascending Aorta in Ischemic Heart Disease. Ann Thorac Surg. 1990; 50(4):539–542.
66. Wareing, T. H., Davila-Roman, V. G., Barzilai, B., Murphy, S. F., Kouchoukos, N. T. Management of the severely atherosclerotic ascending aorta during cardiac operations. a strategy for detection and treatment. J Thorac Cardiovasc Surg. 1992; 103(3):453–462.
67. St Amand, M. A., Murkin, J. M., Menkis, A. H., et al. Aortic atherosclerotic plaque identified by epiaortic scanning predicts cerebral embolic load in cardiac surgery. Can J Anaesth. 1997; 44:A7.
68. Cohen, A., Tzourio, C., Bertran, B., Chauvel, C., Bousser, M. G., Amarenco Aortic Plaque Morphology, P., Events, Vascular. A Follow-Up Study in Patients With Ischemic Stroke; FAPS Investigators. French Study of Aortic Plaques in Stroke. Circulation. 1997; 96:3838–3841.
69. Konstadt, S. N., Reich, D. L., Kahn, R., et al. Transesophageal echocardiography can be used to screen for ascending aortic atherosclerosis. Anesth Analg. 1995; 81:225–228.
70. Konstadt, S. N., Reich, D. L., Quintana, C., Levy, M. The ascending aorta: how much does transesophageal echocardiography see? Anesth Analg. 1994; 78:240–244.
71. Hangler, B. H., Nagele, G., Danzmayr, M., et al. Modification of surgical technique for ascending aortic atherosclerosis: impact on stroke reduction in coronary artery bypass grafting. J Thorac Cardiovasc Surg. 2003; 126:391–400.
72. Barzilai, B., Marshall, W. G., Jr., Saffitz, J. E., Kouchoukos, N. Avoidance of embolic complications by ultrasonic characterization of the ascending aorta. Circulation. 1989; 80(3 Pt 1):1275–1279.
73. Trehan, N., Mishra, M., Kasliwal, R., Mishra, A. Reduced neurological injury during CABG in patients with mobile aortic atheromas: a five-year follow-up study. Ann Thorac Surg. 2000; 70:1558–1564.
74. Djaiani, G., Ali, M., Borger, M. A., et al. Epiaortic Scanning Modifies planned Intraoperative Surgical Management But Not Cerebral Embolic Load During Coronary Artery Bypass Surgery. Anesth Analg. 2008; 106:1611–1618.
75. Gold, J. P., Torres, K. E., Maldarelli, W., Zhuravlev, I., Condit, D., Wasnick, J. Improving Outcomes in Coronary Surgery: The Impact of Echo-Directed Aortic Cannulation and Perioperative Hemodynamic Management in 500 Patients. Ann Thorac Surg. 2004; 78:579–585.
76. Davila-Roman, V. G., Barzilai, B., Wareing, T. H., Murphy, S. F., Kouchoukos, N. T. Intraoperative Ultrasonographic Evaluation of the ascending aorta in 100 Consecutive Patients Undergoing Cardiac Surgery. Circulation. 1991; 84(suppl 5):11147–11153.
77. Ribakove, G. H., Katz, E. S., Galloway, A. C., et al. Surgical Implications of Transesophageal Echocardiography to Grade the Atheromatous Aortic Arch. Ann Thorac Surg. 1992; 53(3):758–761.
78. Trehan, N., Mishra, M., Dhole, S., Mishra, A., Karlekar, A., Kohli, V. N. Significantly Reduced Incidence of Stroke During Coronary Artery Bypass Grafting Using Transesophageal Echocardiography. Eur J Cardiothorac Surg. 1997; 11(2):234–242.
79. Kapetanakis, E. I., Stamou, S., Dullum, M. K. C., et al. The Impact of Aortic Manipulation on Neurologic Outcomes After Coronary Artery Bypass Surgery: A Risk-Adjusted Study. Ann Thorac Surg. 2004; 78:1564–1571.
80. Royse, A. G., Royse, C. F., Ajani, A. E. Reduced Neuropsychological Dysfunction Using Epiaortic Echocardiography and the Exclusive Y. Graft. Ann Thorac Surg. 2000; 69:1431–1438.
81. Dijk, D. V., Jansen, E. W. L., Hijman, R., et al. Cognitive Outcome After Off-Pump and On-Pump Coronary Artery Bypass Graft Surgery. JAMA. 2002; 287:1405–1412.
82. Cleveland, J. C., Jr., Shroyer, A. L. W., Chen, A. Y., Peterson, E., Grover, F. L. Off-Pump Coronary Artery Bypass Grafting Decreases Risk-Adjusted Mortality and Morbidity. Ann Thorac Surg. 2001; 72:1282–1289.
83. Stern, A., Tunick, P. A., Culliford, A. T., et al. Protruding aortic arch atheromas: risk of stroke during heart surgery with and without aortic arch endarterectomy. Am Heart J. 1999; 138(4 Pt 1):746–752.
84. Eltzschig, H. K., Kallmeyer, I. J., Mihaljevic, T., Alapati, S., Shernan, S. K. A practical approach to a comprehensive epicardial and epiaortic echocardiographic examination. J Cardiothorac Vasc Anesth. 17(4), 2003. [442-429].
85. Royse, A., Royse, C. A Standardized intraoperative Ultrasound Examination of the Aorta and Proximal Coronary Arteries. Interact Cardiovasc Thorac Surg. 2006; 5:701–704.
86. Glas, K., Swaminathan, M., Reeves, S., et al. Guidelines for the performance of a comprehensive intraoperative epiaortic ultrasonographic examination: recommendations of the American Society of Echocardiography and the Society of Cardiovascular Anesthesiologists; Endorsed by the Society of Thoracic Surgeons. Anesth Analg. 2008; 106:1376–1384.
87. Sekoranja, L., Vuille, C., Bianchi-Demicheli, F., et al. Thoracic aortic plaques, transesophageal echocardiography and coronary artery disease. Swiss Med Wkly. 2004; 134:75–78.
88. MacKenson, G. B., et al. The Perioperative Outcomes Research Group and Cardiothoracic Anesthesiology Research Endeavors (C. A. R. E. ) Investigators of the Duke Heart Center. Preliminary report on the interaction of apolipoprotein E polymorphism with aortic atherosclerosis and acute nephropathy after CABG. Ann Thorac Surg. 2004; 78:520–526.
89. Barzilai, B., Saffitz, J. E., Miller, J. G., Sobel, B. E. Quantitative Ultrasound Characterization of the Nature of Atherosclerotic Plaques in Human Aorta. Circ Res. 1987; 60:459–463.
90. Nohara, H., Shida, T., Mukohara, N., Obo, H., Higami, T. Ultrasonic Plaque Density of Aortic Atheroma and Stroke in Patients Undergoing On-Pump Coronary Bypass Surgery. Ann Thorac Cardiovasc Surg. 2004; 10:235–240.
91. Bainbridge, D. T., Murkin, J. M., Menkis, A., Kiaii, B. The Use of 3D Epiaortic Scanning to Enhance Evaluation of Atherosclerotic Plaque in the Ascending Aorta: A Case Series. Heart Surg Forum. 2004; 7(6):E636–E639.
92. Bainbridge, D. 3-D Imaging for Aortic Plaque Assessment. Semin Cardiothorac Vasc Anesth. 2005; 9(2):163–165.
93. Hager A, Kaemmerer H, Rapp-Bernhardt U, et al. Diameters of the thoracic aorta throughout life as measured with helical computed tomography. J Thorac Cardiovasc Surg 123(6): 1060–1066.
94. Wolak, A., Gransar, H., Thomson, E. J., Friedman, J. D., et al. Aortic size assessment by noncontrast cardiac computed tomography: normal limits by age, gender, and body surface area. JACC Cardiovasc Imaging. 2008; 1(2):200–209.
95. O’Rourke, M., Farnsworth, A., O’Rourke, J. Aortic dimensions and stiffness in normal adults. JACC Cardiovasc Imaging. 2008; 1(6):749–751.
96. Biaggi, P., Matthews, F., Braun, J., Rousson, V., Kaufmann, P. A., Jenni, R. Gender, age, and body surface area are the major determinants of ascending aorta dimensions in subjects with apparently normal echocardiograms. J Am Soc Echocardiogr. 2009; 22:720–725.
97. Roman, M. J., Devereux, R. B., Kramer-Fox, R., O’Loughlin, J. Two-dimensional echocardiographic aortic root dimensions in normal children and adults. Am J Cardiol. 1989; 64:507–512.
98. Vasan, R. S., Larson, M. G., Benjamin, E. J., Levy, D. Echocardiographic reference values for aortic root size: the Framingham Heart Study. J Am Soc Echocardiogr. 1995; 8(6):793–800.
99. Vasan, R. S., Mg, Larson, Levy, D. Determinants of echocardiographic aortic root size. The Framingham Study. Circulation. 91(3), 1995. [734-30].
100. Erbel, R., Alfonso, F., Boileau, C., et al. Diagnosis and management of aortic dissection. Eur Heart J. 2001; 22:1642–1681.
101. Lang, R. M., Bierig, M., Devereux, R. V., et al. Recommendations for chamber quantification: a report from the American Society of Echocardiography’s Guidelines and Standards Committee and the Chamber Quantification Writing Group, developed in conjunction with the European Association of Echocardiography, a branch of the European Society of Cardiology. J Am Soc Echocardiogr. 2005; 18:1440–1463.
102. Kazui, R., Izumoto, H., Yoshioka, K., et al. Dynamic morphologic changes in the normal aortic annulus during systole and diastole. J Heart Valve Dis. 2006; 15:617–621.
103. Demertzis, S., Casso, G., Torre, T., et al. Direct epiaortic ultrasound scanning for the rapid confirmation of intraoperative aortic dissection. Interact Cardiovasc Thorac Surg. 2008; 7:725–726.
104. Inoue, Y., Takahashi, R., Ueda, T., et al. Synchronized epiaortic two-dimensional and color Doppler echocardiographic guidance enables routine ascending aortic cannulation in type A acute aortic dissection. J Thorac Cardiovasc Surg. 2011; 141:354–360.
105. Seki, T., Maruyama, R., Inoue, Y., et al. Ascending aorta cannulation in Stanford type a acute aortic dissection. Kyobu Geka. 2012; 65:184–188.
106. Edrich, T., Shernan, S. K., Smith, B., et al. Usefulness of intraoperative epiaortic echocardiography to resolve discrepancy between transthoracic and transesophageal measurements of aortic valve gradient–a case report. Can J Anesth. 2003; 50:293–296.



