[level-membership-for-opthalmology-category]13.1
Non-Proliferative Diabetic Retinopathy
Clinical Features:
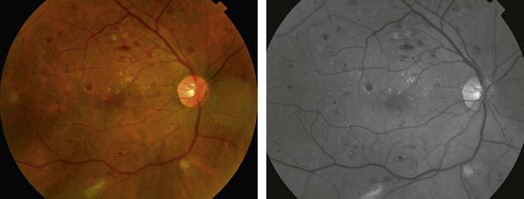
In the early stages, non-proliferative diabetic retinopathy (NPDR) is typically asymptomatic. Retinal manifestations of DR are caused by a microangiopathy that manifests itself as microaneurysms; the hallmarks of NPDR are intraretinal hemorrhages, cotton wool spots, hard exudates, and, in some eyes, macular edema (Fig. 13.1.1). Venous beading and intraretinal microvascular abnormalities may happen in severe NPDR. NPDR is sub-classified as mild, moderate or severe based on the presence and severity of these findings.
OCT Features:
Although OCT scanning is not needed for the diagnosis of any form of DR, OCT findings of DR are well characterized on OCT. However, small intraretinal hemorrhages seen in the early stages of diabetes may not be detectable on even high resolution line scans. Microaneurysms appear as hyper-reflective foci, mostly within the outer half of the retina, usually spanning more than one retinal layer. They typically have an inner homogenous lumen with moderate reflectivity surrounded by a hyper-reflective rim. Hyporeflectivity around the microaneurysm is usually associated with leakage on fluorescein angiography. Microaneurysm closure may be associated with resolution of hyper-reflectivity or by a smaller lumen with heterogenous hyper-reflectivity (Figs 13.1.2 to 13.1.4).
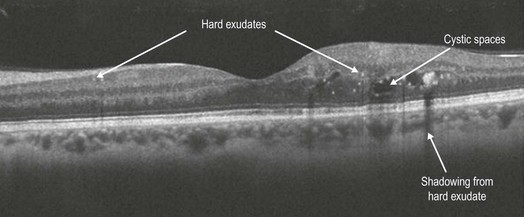
Figure 13.1.2 OCT line scan in a diabetic shows hyper-reflective clusters most likely representing hard exudates between the inner plexiform and the inner nuclear layer.
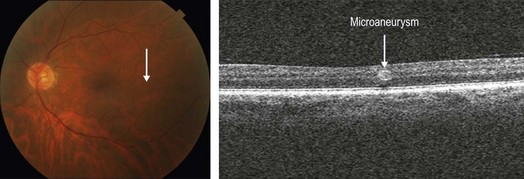
Figure 13.1.3 Photo and OCT line scan through a microaneurysm (white line) showing a discrete, well demarcated area of hyper-reflectivity characteristic of diabetic microaneurysms.
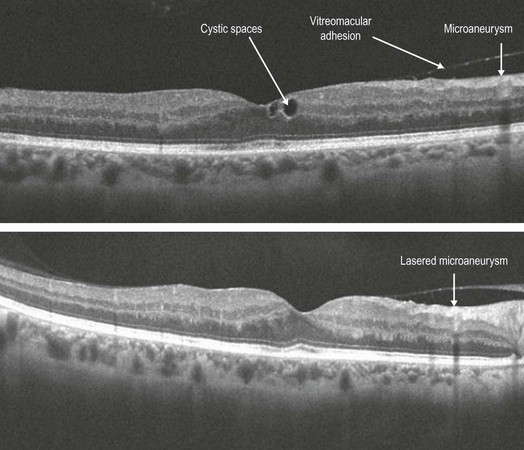
Figure 13.1.4 The upper image is a line scan through a microaneurysm showing an inner retinal discrete microaneurysm spanning several layers with a hyper-reflective border and relatively hypo-reflective lumen (arrow). The image below shows a post-focal laser OCT line scan through the same microaneurysm showing shrinkage and hyper-reflectivity throughout the now occluded lumen.
Cotton wool spots appear as areas of moderate hyper-reflectivity within the nerve fiber layer. Larger cotton wool spots show shadowing. Hard exudates are also seen as small, relatively well demarcated hyper-reflective clusters usually deeper within the retina and may span multiple layers. Another OCT parameter seen in diabetic patients is presence of hyper-reflective foci within the outer retina on OCT scanning, especially in diabetic macular edema (Fig. 13.1.2). These hyper-reflective foci probably represent a variety of microstructural pathologies including microaneurysms and hard exudates. The baseline amount of hyper-reflective foci seems to correlate positively with HbA1c values.
[/level-membership-for-opthalmology-category][not-level-membership-for-opthalmology-category]13.1
Non-Proliferative Diabetic Retinopathy
Clinical Features:
In the early stages, non-proliferative diabetic retinopathy (NPDR) is typically asymptomatic. Retinal manifestations of DR are caused by a microangiopathy that manifests itself as microaneurysms; the hallmarks of NPDR are intraretinal hemorrhages, cotton wool spots, hard exudates, and, in some eyes, macular edema (Fig. 13.1.1). Venous beading and intraretinal microvascular abnormalities may happen in severe NPDR. NPDR is sub-classified as mild, moderate or severe based on the presence and severity of these findings.
[/not-level-membership-for-opthalmology-category]
