[level-membership-for-dermatology-category]
New trends in dermatological treatment
Therapeutic advances have revolutionized the treatment of skin disease over the last 40 years. The 1960s saw the introduction of topical steroids, the 1970s the development of psoralen with ultraviolet A (PUVA), the 1980s retinoids, and the 1990s lasers and ciclosporin. The major advance of the ‘noughties’ was the biologics.
Atopic eczema
The topical immunomodulators (calcineurin inhibitors) tacrolimus (Protopic) and pimecrolimus (Elidel) are alternatives to topical steroids and do not cause skin atrophy (Fig. 1). The systemic immunosuppressors mycophenolate mofetil and methotrexate (the latter often used in psoriasis) may be beneficial in severe atopic eczema.

Bullous diseases
Intravenous immunoglobulin is used for severe pemphigus or mucous membrane pemphigoid. The biologic rituximab has been used in resistant cases (p. 33). Oral doxycycline may be effective in pemphigoid.
Cutaneous T cell lymphoma
The retinoid receptor agonist bexarotene (Targretin) is effective in some patients with cutaneous T cell lymphoma. Photophoresis, in which a lymphocyte-enriched blood fraction from the patient who has taken a psoralen is exposed to UVA outside the body and then re-infused, is sometimes effective, especially for the Sézary syndrome (p. 44).
Fungal infections
Terbinafine (Lamisil) cream, applied once or twice daily for 1 week, cures tinea pedis (Fig. 2). Pulse treatment with oral itraconazole (Sporanox), terbinafine (Lamisil) or fluconazole (Diflucan) has given cure rates of 80% for fungal infection of the toenails. Three-weekly pulses of terbinafine (Lamisil) given over 8 weeks produce a 90% cure rate for childhood tinea capitis (Fig. 3).


Hidradenitis suppurativa
Hidradenitis suppurativa (p. 65) is characterized by abscesses, sinuses and scars in the axillae and groin (Fig. 4) and is very difficult to treat. Acitretin is helpful in suitable patients, as can be the combination of the antibiotics clindamycin and rifampicin. Recently, infliximab infusion has been used with success (p. 33).

Hyperhidrosis
The injection of botulinum toxin A (Botox, Dysport) into the axillary or palmar skin will control excessive sweating in these areas (p. 65), but needs to be repeated every 9 months.
Leg ulcers
Larval therapy with sterile maggots (LarvE) can be used for managing sloughy leg ulcers (p. 72). Recombinant platelet-derived growth factor (becaplermin) is licensed for use in neuropathic ulcers, e.g. in diabetes. Tissue-engineered skin equivalents, e.g. Apligraf, can be effective in therapy-resistant wounds.
Psoriasis
The biologics have revolutionized the treatment of severe psoriasis (p. 19). Other systemic approaches to consider in difficult to manage cases where biologics may be contraindicated or have failed include the fumaric acid esters and mycophenolate mofetil.
Scabies
Ivermectin, a drug used to treat onchocerciasis (p. 61), may be effective for scabies, especially of the crusted (Norwegian) type (p. 118) and for use in institutional outbreaks.
Scleroderma
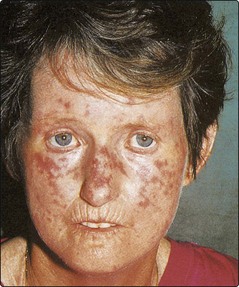
Topical calcipotriene (0.005%) has been shown to improve lesions of localized scleroderma (morphoea). Oral methotrexate is beneficial in certain types of morphoea, e.g. en coup de sabre. Systemic sclerosis (Fig. 5) can respond to photophoresis (see above) and PUVA.
Vitiligo
The Excimer 308-nm laser (Fig. 6) is effective in the treatment of localized areas of vitiligo affecting the cosmetically sensitive sites, e.g. the face.

Fig. 6 The Excimer 308-nm laser.
It can be used for treating localized areas of vitiligo, psoriasis or cutaneous T cell lymphoma.
New trends in dermatological treatment
| Disease | Topical therapy | Systemic therapy |
|---|---|---|
| Atopic eczema | Pimecrolimus, tacrolimus | Mycophenolate, methotrexate |
| Bullous disease | – | Immunoglobulin, rituximab, doxycycline |
| Cutaneous T cell lymphoma Erythema nodosum |
– – |
Bexarotene, photophoresis Thalidomide |
| Fungal infection | Terbinafine | Pulse itraconazole, terbinafine, fluconazole |
| Hand dermatitis | – | Alitretinoin |
| Hidradenitis suppurativa | – | Acitretin, clindamycin/rifampicin, infliximab |
| Hyperhidrosis | Botulinum toxin (intralesional) | – |
| Leg ulcer | Sterile larvae, skin equivalent | – |
| Psoriasis | – | Biologics, fumaric acid esters, mycophenolate mofetil |
| Scabies | – | Ivermectin |
| Scleroderma | Calcipotriene | Methotrexate, photophoresis |
| Skin cancer | Imiquimod (superficial basal cell carcinoma) | Dacarbazine/interferon-α (malignant melanoma) |
| Toxic epidermal necrolysis | – | Immunoglobulin |
| Vitiligo | – | Excimer laser |
[/level-membership-for-dermatology-category][not-level-membership-for-dermatology-category]
New trends in dermatological treatment
Therapeutic advances have revolutionized the treatment of skin disease over the last 40 years. The 1960s saw the introduction of topical steroids, the 1970s the development of psoralen with ultraviolet A (PUVA), the 1980s retinoids, and the 1990s lasers and ciclosporin. The major advance of the ‘noughties’ was the biologics.
Atopic eczema
The topical immunomodulators (calcineurin inhibitors) tacrolimus (Protopic) and pimecrolimus (Elidel) are alternatives to topical steroids and do not cause skin atrophy (Fig. 1). The systemic immunosuppressors mycophenolate mofetil and methotrexate (the latter often used in psoriasis) may be beneficial in severe atopic eczema.
Bullous diseases
Intravenous immunoglobulin is used for severe pemphigus or mucous membrane pemphigoid. The biologic rituximab has been used in resistant cases (p. 33). Oral doxycycline may be effective in pemphigoid.
Cutaneous T cell lymphoma
The retinoid receptor agonist bexarotene (Targretin) is effective in some patients with cutaneous T cell lymphoma. Photophoresis, in which a lymphocyte-enriched blood fraction from the patient who has taken a psoralen is exposed to UVA outside the body and then re-infused, is sometimes effective, especially for the Sézary syndrome (p. 44).
Fungal infections
Terbinafine (Lamisil) cream, applied once or twice daily for 1 week, cures tinea pedis (Fig. 2). Pulse treatment with oral itraconazole (Sporanox), terbinafine (Lamisil) or fluconazole (Diflucan) has given cure rates of 80% for fungal infection of the toenails. Three-weekly pulses of terbinafine (Lamisil) given over 8 weeks produce a 90% cure rate for childhood tinea capitis (Fig. 3).
[/not-level-membership-for-dermatology-category]
