Chapter 14 Nervous System
Nervous System – Anatomy and Physiology
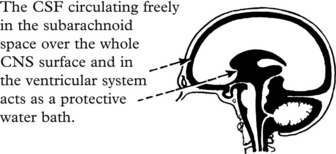
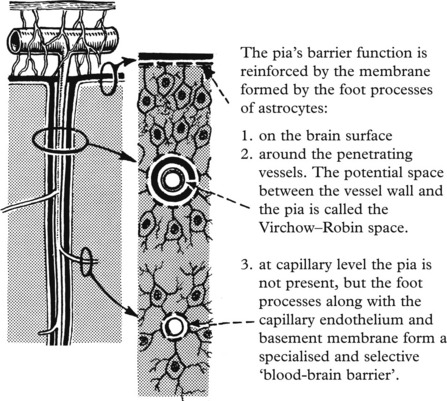
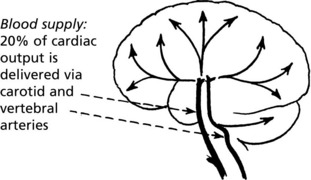
Considerations of anatomy and physiology have important applications to diseases of the central nervous system (CNS), particularly their effects and spread.
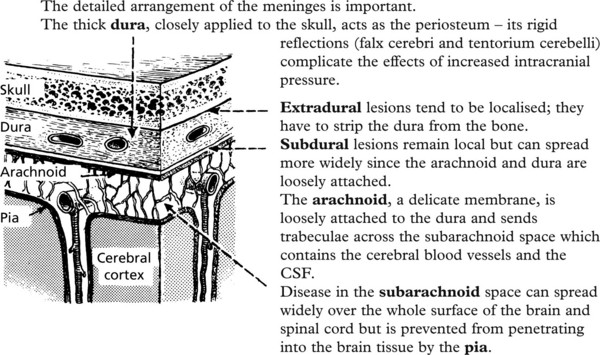
The anatomy of the various coverings is important.
The skull and vertebrae form a rigid compartment protecting the delicate CNS tissues.


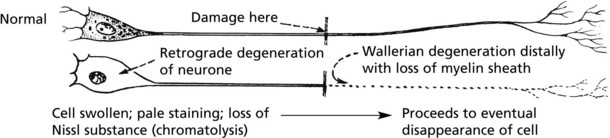
Neuronal Damage
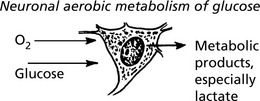
NEURONES are sensitive to damage by a wide variety of agents including anoxia, hypoglycaemia, virus infections and intracellular metabolic disturbances (e.g. associated with vitamin B deficiencies).
There are two main types, depending on the rapidity of the changes.



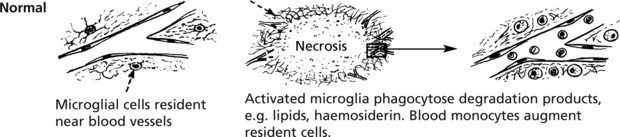
Glial Reactions
The glial cells react vigorously in many diseases of the CNS.



Increased Intracranial Pressure
INCREASED INTRACRANIAL PRESSURE (ICP) occurs in two main circumstances:
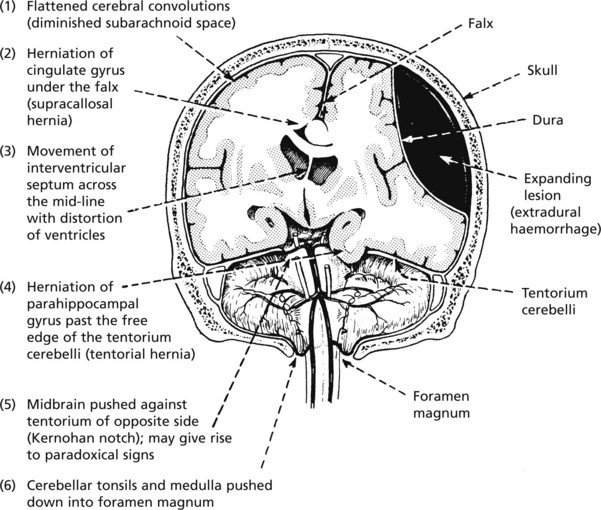
Intracranial Expanding Lesions
These lesions may occur within the brain substance or in the meninges. Important examples are:
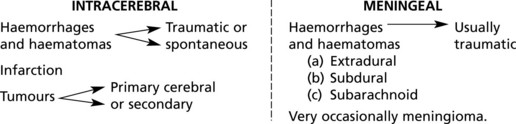
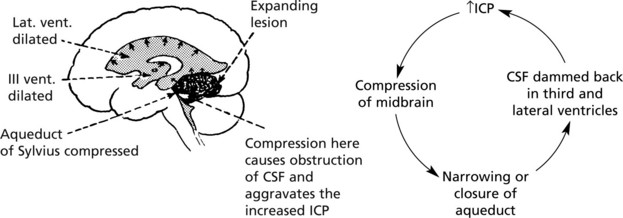
The situation is often aggravated by cerebral OEDEMA.
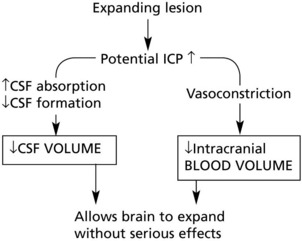
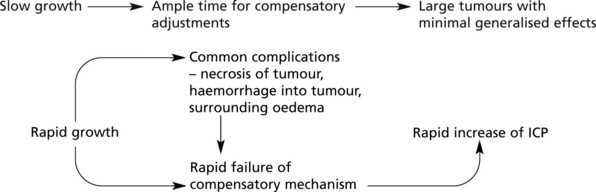
The severity of the effects is modified by two important factors:
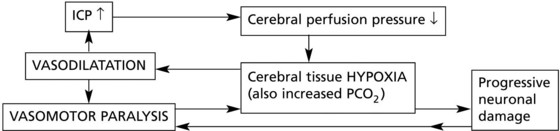
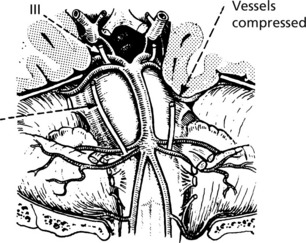
There are three stages in the progress of increased intracranial pressure (ICP).
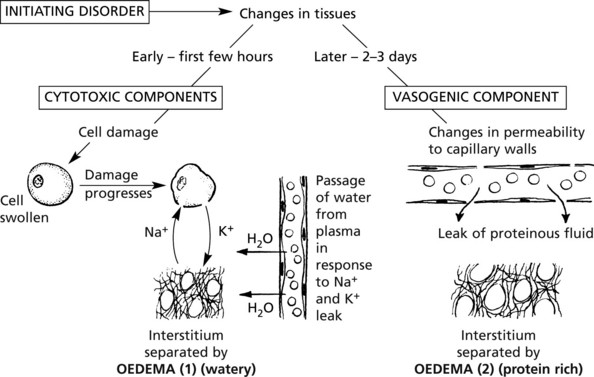
Cerebral Oedema
Swelling of the brain, of which oedema is the major component, is an important complication of many brain diseases because the enlargement either initiates or aggravates increased intracranial pressure.
The process may be localised or generalised depending on the type of initiating disorder.
| Localised conditions | Generalised conditions |
|---|---|
| Examples: | Examples: Intoxications |
| Infarcts, and local ischaemia | Metabolic disturbances, e.g. hypoglycaemia |
| Haematomas (due to vessel rupture and injury) | Generalised hypoxia |
| Tumours | Severe head trauma |
| Malignant hypertension |
The pathological mechanism is as follows:
Increased Intracranial Pressure
Secondary Complications
Circulatory Disturbances
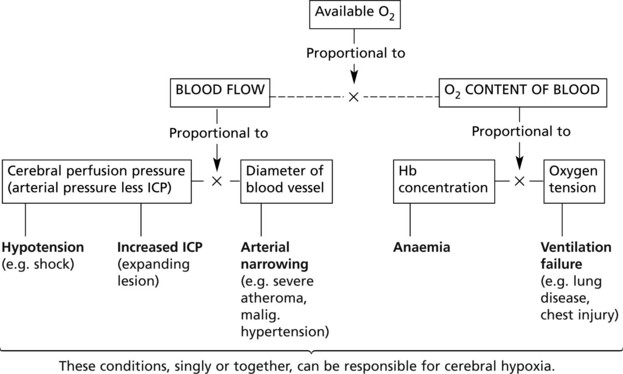
(1) Hypoxia and ischaemia and (2) intracranial haemorrhage are the important and common mechanisms causing brain damage.
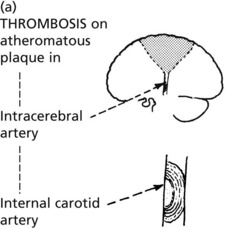
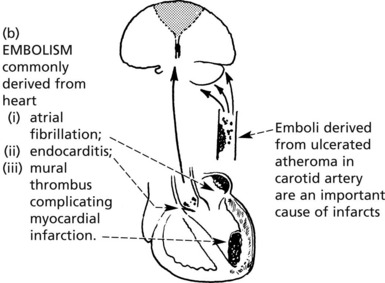
Cerebral Infarction
This condition, the commoner of the two main types of stroke (the other is spontaneous intracerebral haemorrhage), is caused by failure of the supply of oxygen (and glucose) to maintain the viability of the tissues in the territory of a cerebral arterial branch. This is not always due to simple local arterial occlusion, and very often a component of central circulatory deficiency is contributory. The lesion is essentially necrosis of all the tissues in the affected territory.
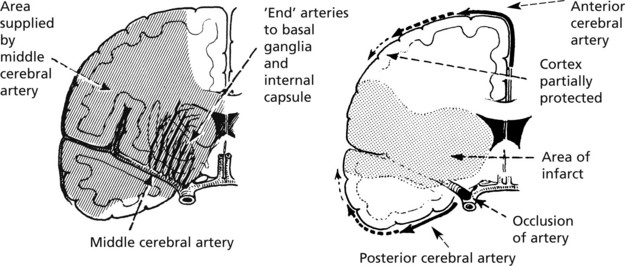
Sites
While infarcts may occur anywhere in the brain, depending on the vagaries of the precipitating arterial lesions, certain sites are more commonly affected.
Brain Damage Due to Cardiac Arrest
| Affected areas – | total cortical necrosis | |
| or | ||
| most sensitive zones | – hippocampus | |
| – layers III, V, VI of cortex | ||
| – within sulci | ||
| – Purkinje cells of cerebellum. |
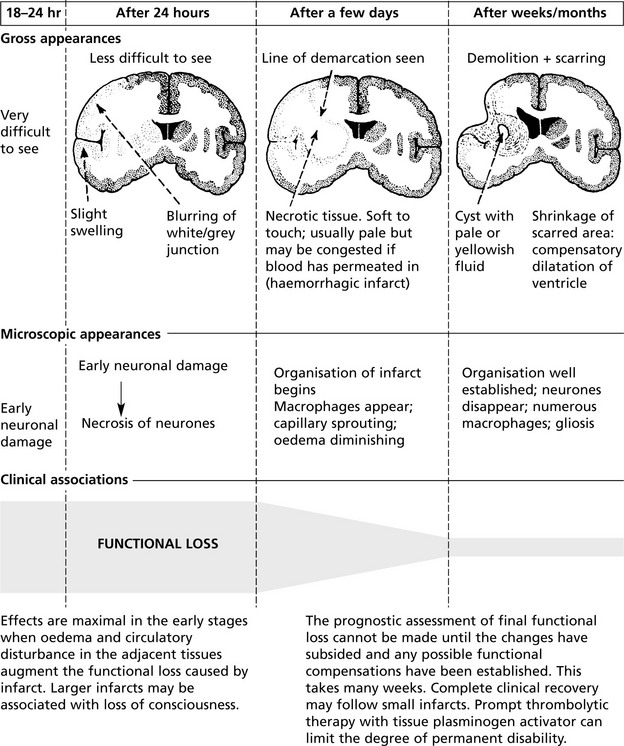
Cerebral Infarction
The diagram below illustrates the evolution of an infarct, e.g. in the territory of the middle cerebral artery. Up to 24 hours there is virtually no visible change.
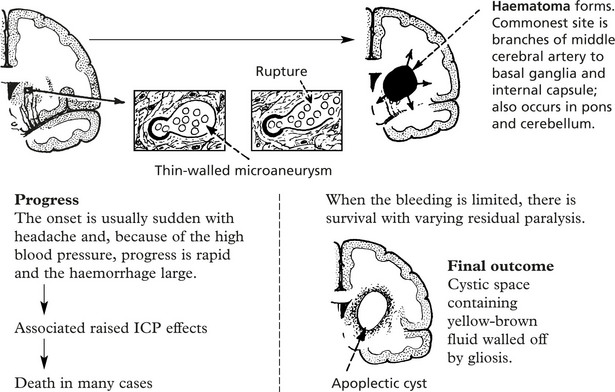
Cerebral Haemorrhage
Spontaneous intracranial bleeding is the second main type of stroke. In the great majority of cases there is localised arterial disease aggravated by hypertension. A small number are associated with cerebral tumours, systemic bleeding diathesis or arteriovenous malformations.
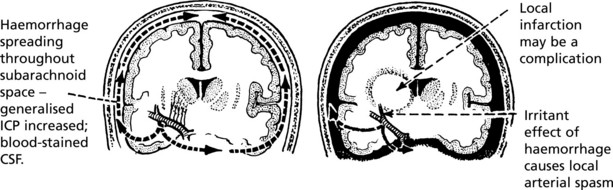
Subarachnoid Haemorrhage
This is commonly but not exclusively the result of rupture of a ‘berry’ aneurysm at or near the circle of Willis. The basic abnormality is a congenital weakness of the elastic tissues in the arterial wall; only rarely is an aneurysm present at birth, and while subarachnoid haemorrhage does occur in young people, the incidence increases with age. Hypertension is an important contributing factor.
Sites Often multiple, near arterial junctions.
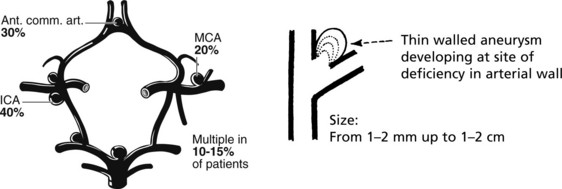
Not all aneurysms rupture; they are found incidentally at autopsy.
Progress
Note: The aneurysm may rupture directly into the brain and mimic an intracerebral haemorrhage.
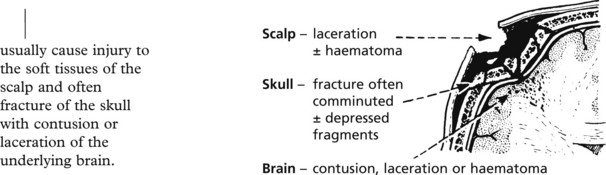
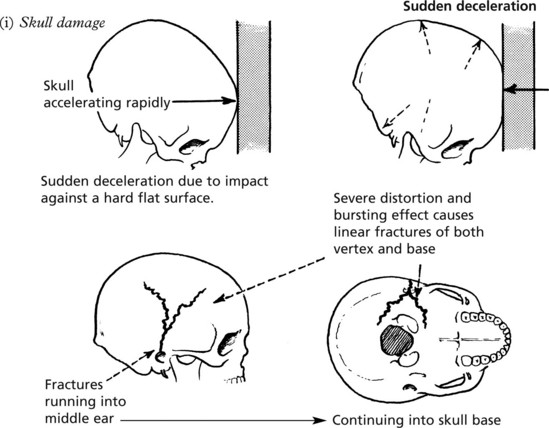
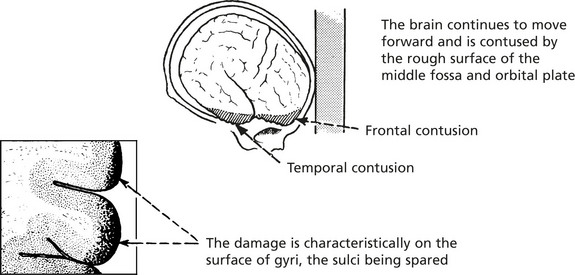
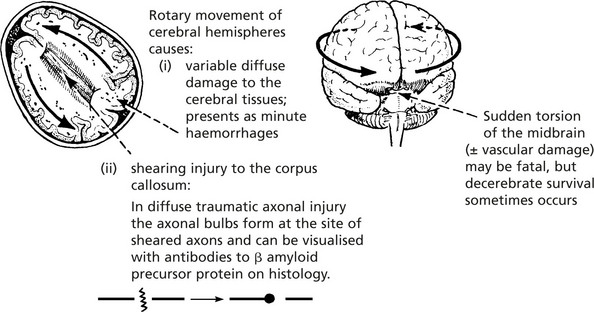
Head Injury
Head injuries of varying severity are common nowadays, particularly as a consequence of road traffic accidents. Immediate damage is caused by two main mechanisms which overcome the protection of the vulnerable cerebral tissues provided by the skull and the CSF ‘water cushion’.
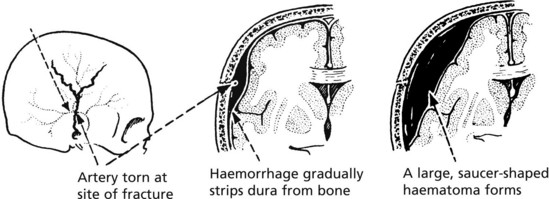
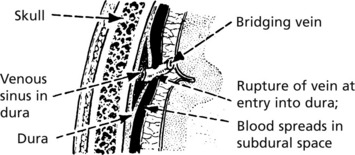
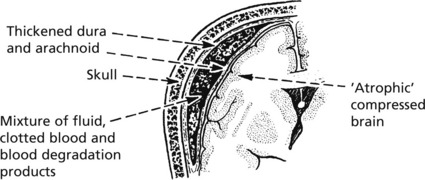
Delayed Complications
In addition to damage sustained immediately at the time of impact, certain serious complications may supervene over the next hours or few days.

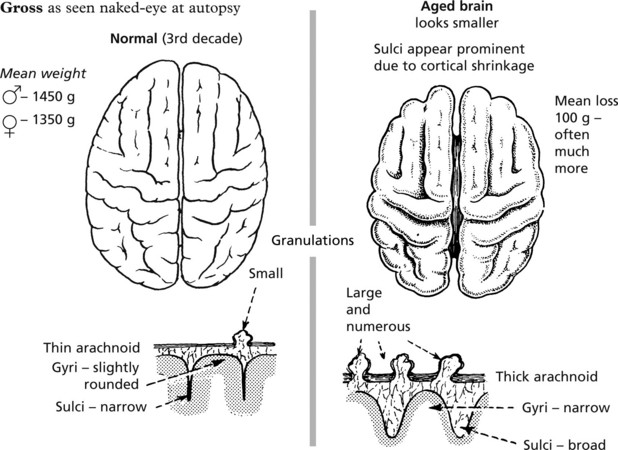
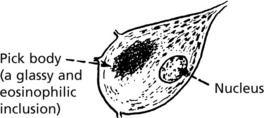
Ageing and Dementia
Alzheimer’s Disease
This disease accounts for around 70% of cases of dementia. While typically a disease of the elderly, especially females, it is also seen in patients under 60 years, in whom there is often a family history. Almost all patients with Down’s syndrome who survive to 50 years develop Alzheimer’s (suggesting that chromosome 21 is important).
Pathology
The histological hallmarks are:


Paired helical filaments composed of tau protein form around the nuclei of neurones.
Pathogenesis – this is not fully understood but the theories include:
Genetic factors – several genes are involved
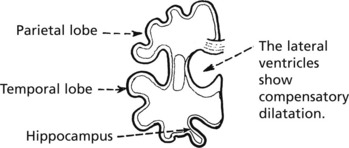
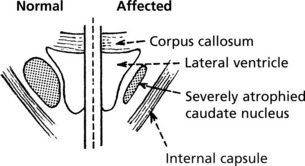
Dementia
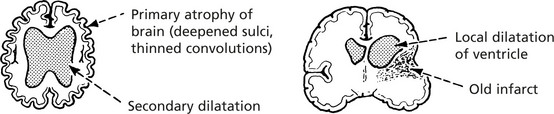
Multi-Infarct Dementia
This form of dementia is associated with vascular disease – with infarcts often in the middle cerebral arterial distribution. The volume of brain loss appears to be important.
Loss of >100ml of brain correlates with dementia.
Hypertension is an important underlying factor. A stepwise progression is typical.
Infections
Compared with the high incidence of infection generally, infection of the central nervous system is uncommon. The pathological effects may be slight and wholly recoverable as in some virus infections, or severe, leading to permanent damage or death.

Infections will be considered in three broad aetiological groups:
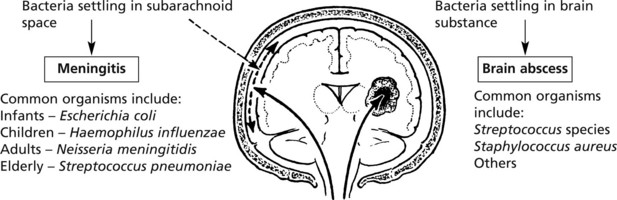
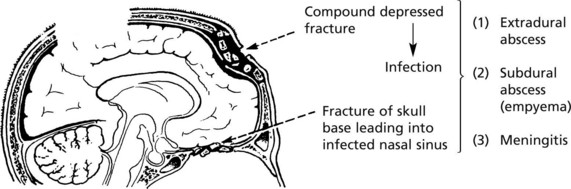
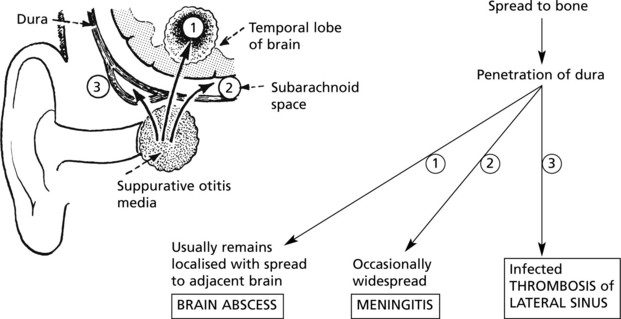
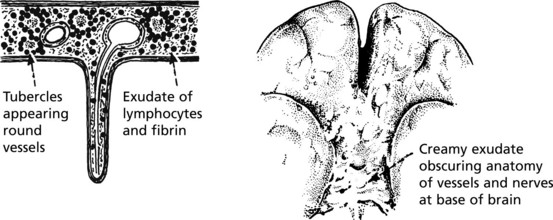
Pyogenic Brain Abscess
The abscesses resulting from direct spread of adjacent infection or by blood borne infection – as seen particularly in bronchiectasis – are often well circumscribed by a pyogenic membrane.
Virus Infections
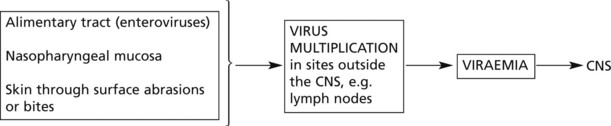
Compared with the incidence of virus infections in general, infection of the central nervous system is rare, even with viruses having an affinity for the CNS – NEUROTROPIC VIRUSES.
Virus infection also has a possible role in oncogenesis within the CNS.
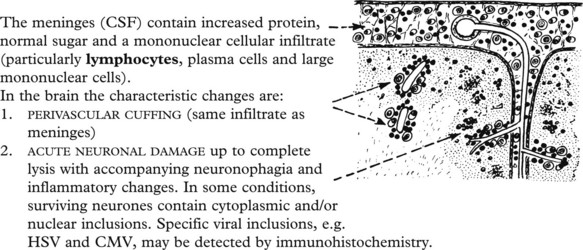
Basic Pathological Effects
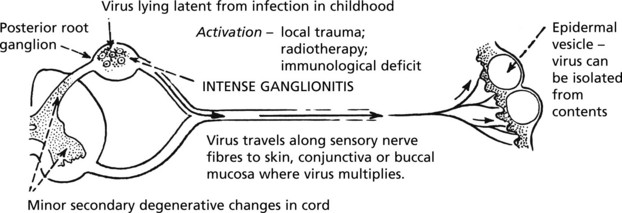
Herpes Simplex Virus (HSV) Encephalitis
This is the commonest form of severe acute viral encephalitis and is almost always due to Herpes Simplex Virus Type 1. It occurs in 2 forms:
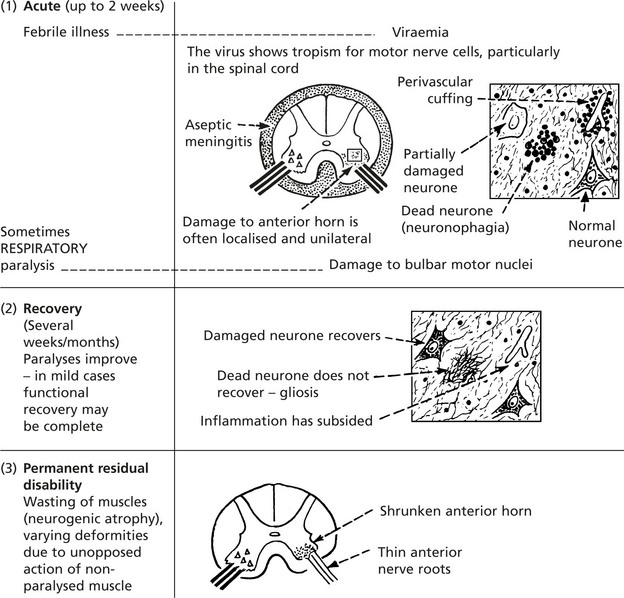
Enteroviruses
These are small RNA viruses (picornavirus group) and include polioviruses, coxsackie viruses and echoviruses.

Persistent Virus Infections
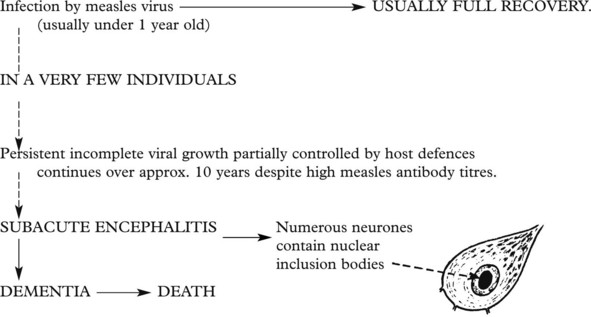
Subacute sclerosing panencephalitis is a very rare disorder due to reactivation of latent measles virus. It affects children and young adults, often several years after uncomplicated measles, and is usually fatal within 6 months. The sequence is probably as follows:
Prion Diseases
Also known as the transmissible spongiform encephalopathies, this group of diseases is caused by abnormal, distorted PRIONS. A prion is a small protein molecule found in the brain cell membrane. Normal cellular prion protein is termed PrPc whereas the distorted protein is termed PrPsc (originally referring to scrapie but now a generic term).

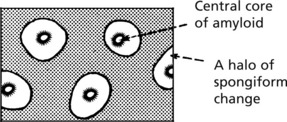
Pathology
There are 4 characteristic histological features:
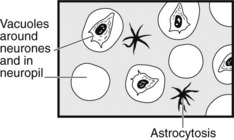
They can be detected by immunohistochemistry with antibodies to PrPsc.
Types of Prion Disease
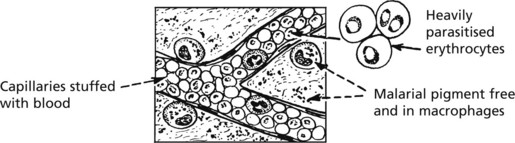
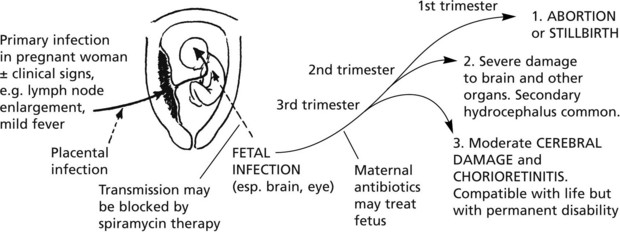
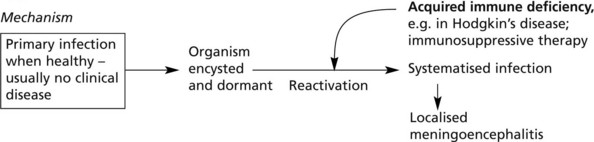
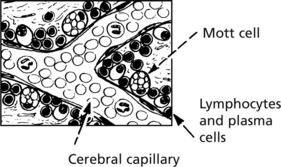
Miscellaneous Infections and Infestations

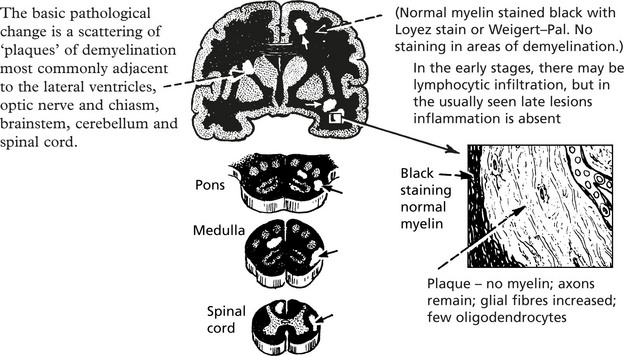
Demyelinating Diseases
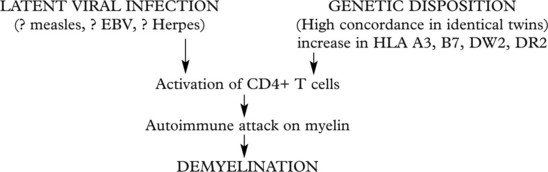
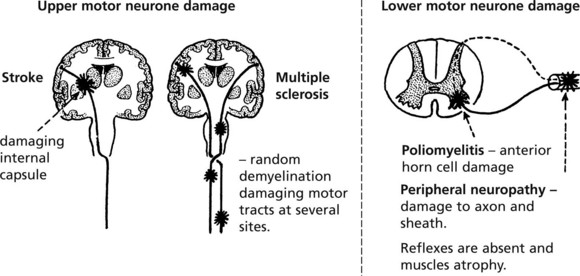
Multiple Sclerosis (MS)
This is the commonest demyelinating disease – where the myelin sheath breaks down, leaving the axons healthy but with serious effects on their function. Multiple sclerosis is a chronic disease of young adults.

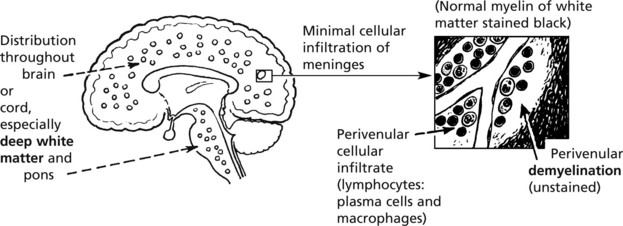
Acute Disseminated Encephalomyelitis
An acute encephalitis in which demyelination is a prominent and characteristic feature is a very rare sequel to many natural viral diseases such as mumps, measles, chickenpox and rubella and to vaccination, historically against smallpox and rabies.
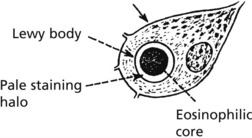
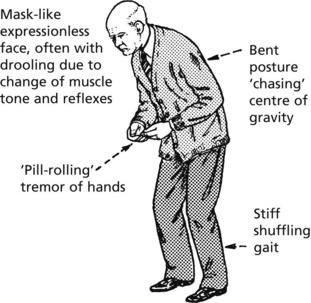
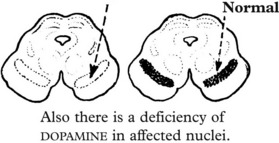
Parkinson’s Disease
This is a disease of the extrapyramidal system which links the higher motor centres and effector motor cells of the spinal cord. Important neurotransmitters are DOPAMINE and γ-aminobutyric acid (GABA).
Aetiology – The disease occurs in 2 main circumstances:
Clinically, Parkinsonism illustrates the classical features of extrapyramidal damage.
Miscellaneous Disorders
Nutritional and Metabolic Disorders (Encephalopathies)
In the last analysis, all disorders in this group are mediated by disturbed neuronal metabolism, so that exact classification may present some difficulty. However, it is convenient to consider them in 2 broad groups.
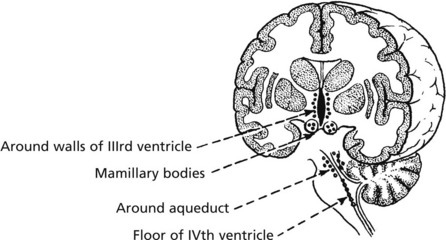
Wernicke’s Encephalopathy

The lesions have a characteristic anatomical distribution:
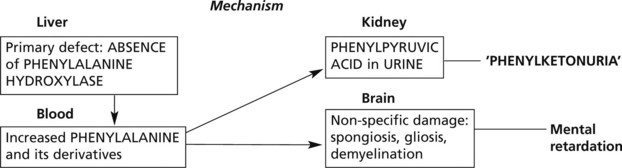
In the following examples, the metabolic defect causes neurological disorder, but in addition, other organs are seriously disturbed.
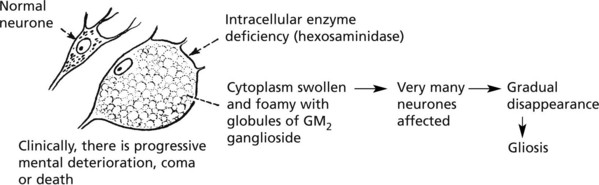
Tay-Sach’s disease (amaurotic familial idiocy) is an illustrative example.
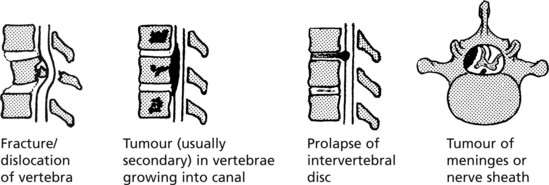
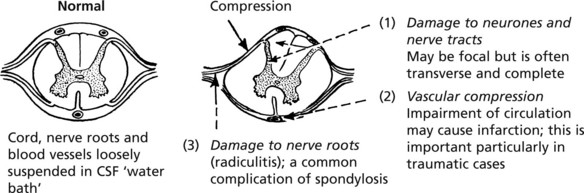
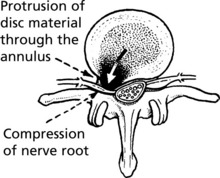
Diseases of the Spinal Cord
In purely spinal lesions, basic disease processes have important anatomical and functional implications. Lack of space for expansion produces important compression effects. Examples are:
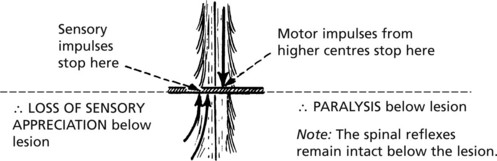
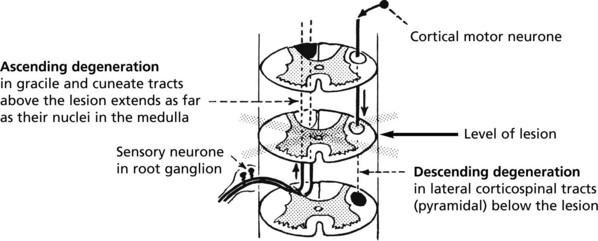
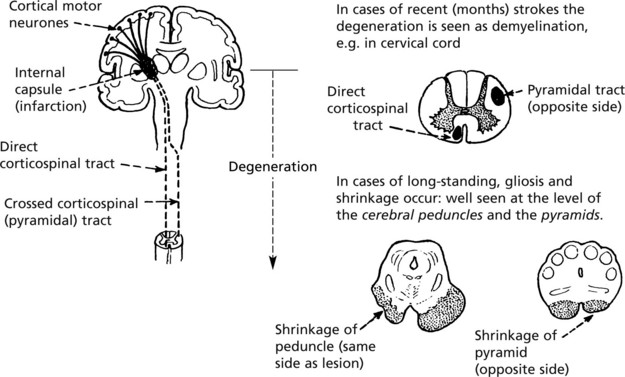
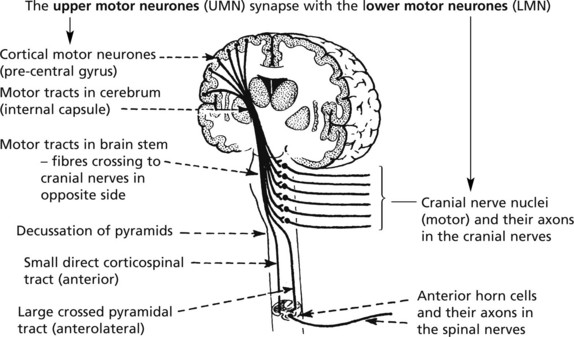
Disorders of Motor Pathways
The concept of upper and lower motor neuronal activity, based on anatomical and physiological evidence, has great clinical value in diagnosis.
Note: Clinically, tendon jerks are increased and the plantar reflex is extensor.
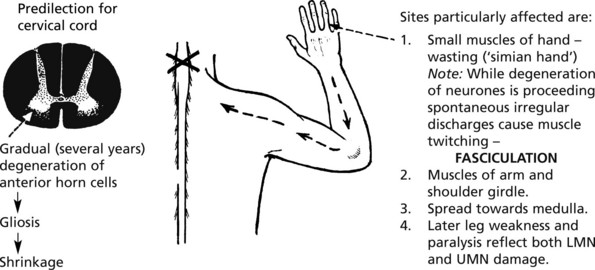
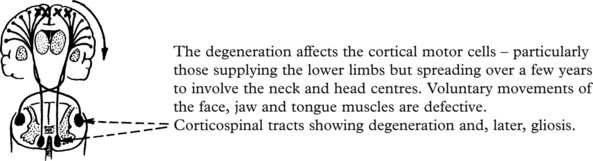
Motor Neurone Disease
This is a disease of unknown aetiology occurring predominantly in adult males. In a few cases motor neurone disease is familial and is caused by a mutation in the gene encoding a free radical scavenger, superoxide dismutase 1. Other susceptiblity genes have been identified.
Three variants of MND are recognised according to the distribution of the disease process.
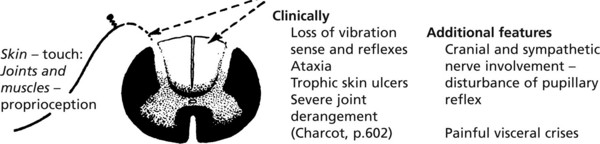
Mixed Motor and Sensory Disorders
Subacute Combined Degeneration of Cord
Due specifically to vit B12 deficiency. If replacement therapy is begun early enough, there is restoration to normal.



The Peripheral Nerves/The Neuropathies
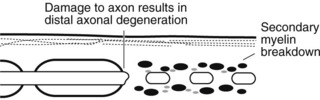

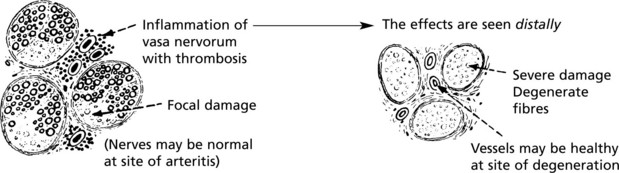
The Neuropathies
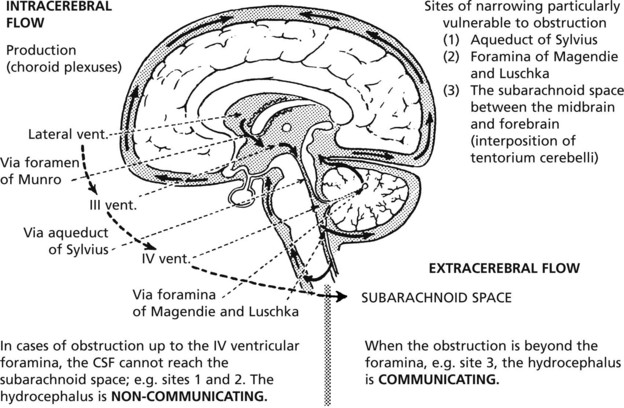
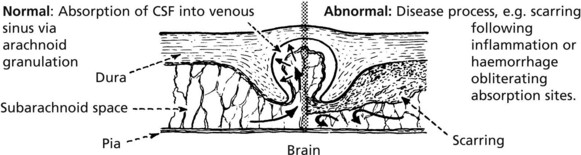
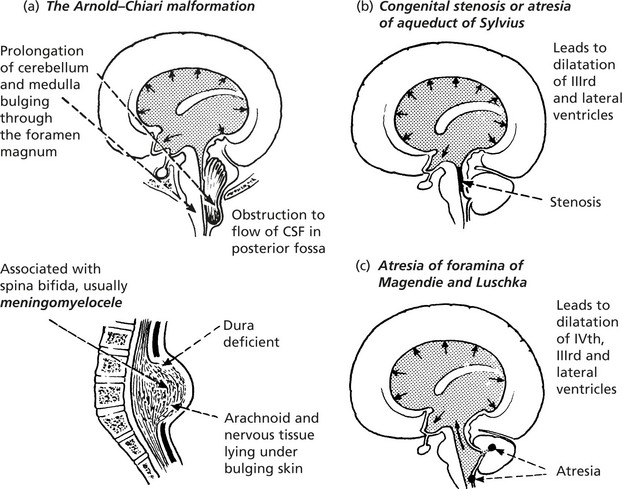
Hydrocephalus
In hydrocephalus, the volume of the CSF is increased and the ventricles are dilated. In the majority of cases, there is an increase in intracranial pressure. Three possible mechanisms are considered.
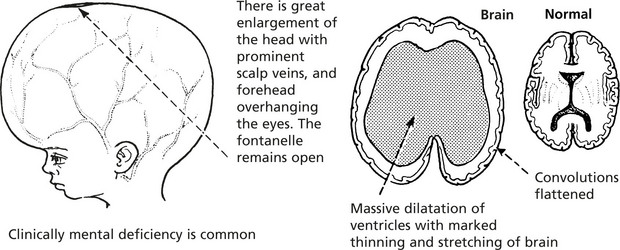
Effects
In the infant and young child, the pliable skull expands to accommodate the enlarging brain – but these extreme changes do not occur if an effective shunt is inserted.
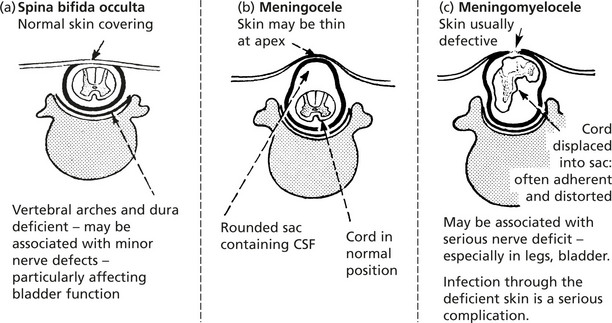
Developmental Abnormalities
Developmental abnormalities of the brain and cranium are relatively common. They range from anencephaly (absence of brain) to minor malformations, e.g. meningocele and encephalocele. There may be associated congenital defects elsewhere in the body.
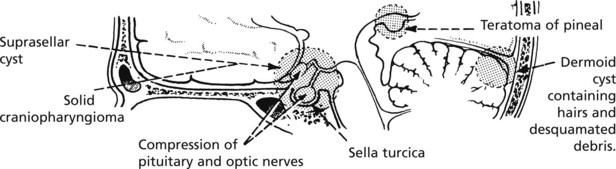
Tumours of the Nervous System
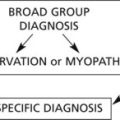
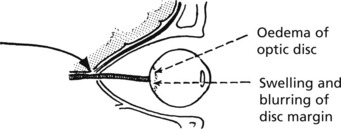
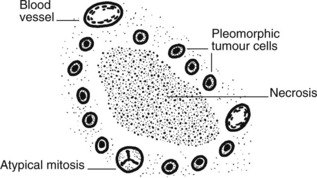
The following scheme illustrates the various non-specific clinicopathological effects of a tumour within the skull.
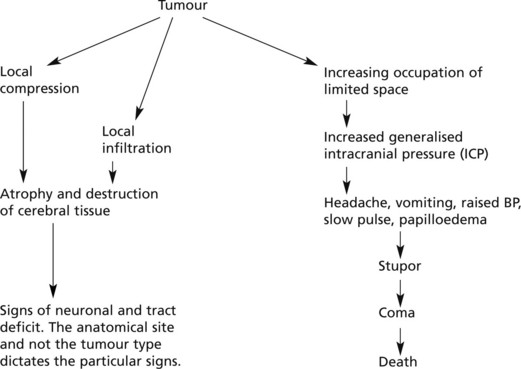
Tumours will be considered in a simplified form under the following broad headings:
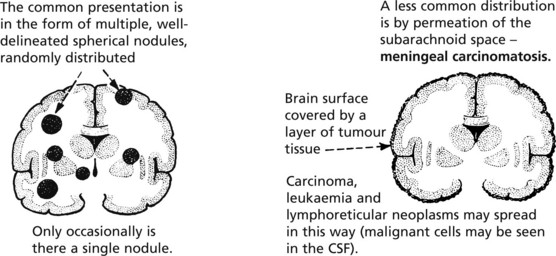
Secondary Brain Tumours
In the general population the incidence of metastatic cerebral tumour is much higher than that of primary cerebral neoplasm. The two most common primary sites are lung and breast, but any malignant tumour can metastasise to the brain.
There is a wide range of disorders which are conveniently divided into two groups:
| Examples | Mechanism caused by cancer | |
|---|---|---|
| Opportunistic infections | _______________________ | Immune depression |
| Metabolic and hormonal imbalance | _______________________ | Destruction of organs, e.g. liver, kidney Inappropriate secretion |
| Vascular accidents | ______________________ | Coagulation disorders |
Primary Brain Tumours
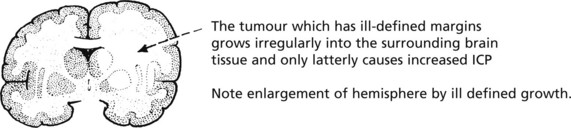
Tumours of the Nervous System
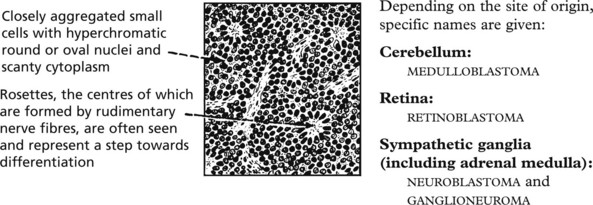
Tumours of Neuronal Type Cells
Fully differentiated neurones can neither multiply nor give rise to neoplasms. Tumours of this type, derived from primitive nerve precursors (blast cells), are seen in infancy and childhood before completion of differentiation.
They display a basic histological pattern.
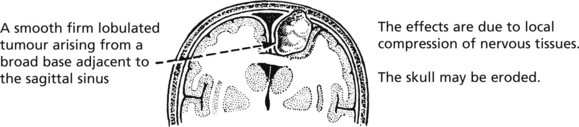
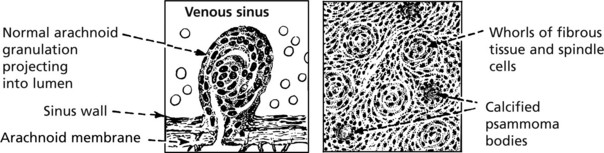
Meningiomas
These are thought to arise from arachnoid granulations and so are found most commonly adjacent to venous sinuses. They account for 15–20% of intracranial tumours. They are slow growing and essentially ‘benign’. A few more aggressive tumours may metastasise.
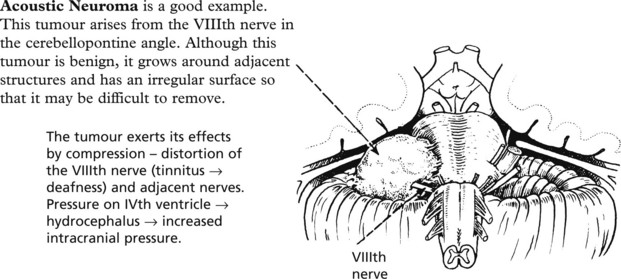
Tumours of Peripheral Nerves
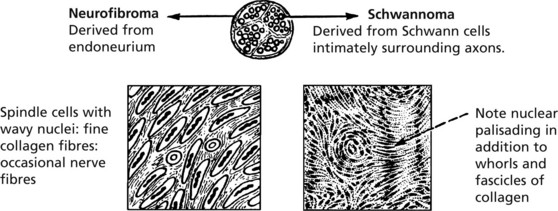
Note: Since neurones do not give rise to these neoplasms, the term neuroma is not used. Traumatic neuroma indicates proliferating nerve endings following injury and is not a true neoplasm (see p.57).
Cerebrospinal Fluid
Although the CSF and extracellular fluid of the central nervous system are essentially similar in composition, changes in the CSF are not reliable indicators of disease within the brain parenchyma.
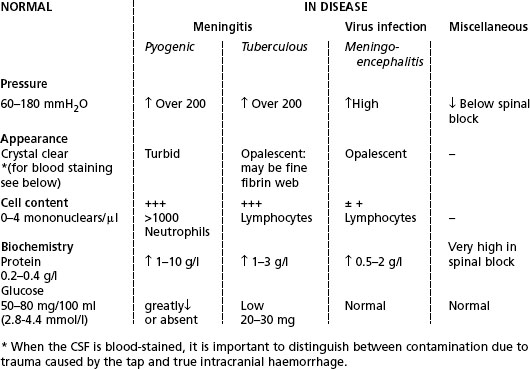

Microbiology. Identification of organisms is very important.

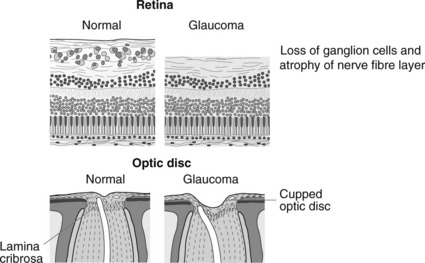
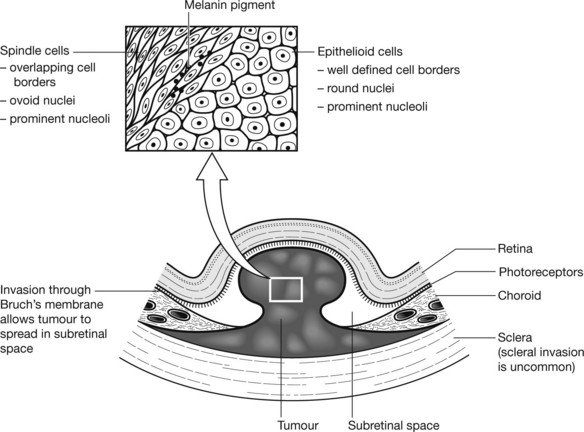
The Eye
Cataract
The normal lens consists of soluble crystalline proteins encased within elongated lens fibre cells surrounded by an elastic lens capsule. There is also a layer of lens epithelium beneath the anterior capsule. The metabolism of the lens depends on diffusion of nutrients from the aqueous. In cataract the lens is opaque either because of disorganisation of the fibre membranes at a microscopic level or of the lens proteins at a molecular level. Cataract is one of the most common and treatable causes of blindness worldwide.
Aetiology Of Cataracts
Developmental: due to congenital malformation or toxic damage to lens fibres, e.g. Rubella.
Inflammation: inflammatory mediators alter the constituents of the aqueous.
Metabolic Disease: hypocalcaemia and diabetes alter the consituents of the aqueous.
Senile: due to degradation of lens proteins in the oldest central part of the lens.