[level-membership-for-emergency-medicine-category]
Chapter 2 Neonatal Resuscitation
2 What preparation is necessary for the unexpected emergency department (ED) delivery?
Preparation is key, as most ED deliveries are “unexpected.” A prearranged plan should be set in motion as soon as birth is imminent. That plan should include the assembly of personnel who are best able to take care of the newly born infant. A brief history should be obtained if possible because it may affect the resuscitation. Equipment and medications specifically for a neonatal resuscitation should be kept in a designated tray so they are quickly available (Table 2-1). Periodic inspection of this equipment for proper functioning and expiration dates of medication should become part of the routine upkeep of the neonatal resuscitation tray.
Table 2-1 Equipment and Drugs for the Neonatal Resuscitation
| Equipment |
 Gowns, gloves, and masks Gowns, gloves, and masks |
 Warm towels and blankets Warm towels and blankets |
 Bulb syringe Bulb syringe |
 Meconium aspirator Meconium aspirator |
 Suction catheters (sizes 5–10 Fr) Suction catheters (sizes 5–10 Fr) |
 Face masks (sizes premature, newborn, and infant) Face masks (sizes premature, newborn, and infant) |
 Oral airways (sizes 000, 00, 0) Oral airways (sizes 000, 00, 0) |
 Anesthesia bag with manometer (preferably 500 mL, no larger than 750 mL) Anesthesia bag with manometer (preferably 500 mL, no larger than 750 mL) |
 Laryngoscope with straight blades (sizes 0 and 1) Laryngoscope with straight blades (sizes 0 and 1) |
 Spare bulbs and batteries Spare bulbs and batteries |
 Stethoscope Stethoscope |
 Endotracheal tubes (sizes 2.5, 3.0, 3.5, 4.0) and stylet Endotracheal tubes (sizes 2.5, 3.0, 3.5, 4.0) and stylet |
 Tape Tape |
 Umbilical catheters (3.5 and 5 Fr) Umbilical catheters (3.5 and 5 Fr) |
 Oxygen source with flow meter Oxygen source with flow meter |
 Umbilical catheter tray Umbilical catheter tray |
 Three-way stopcocks Three-way stopcocks |
 Nasogastric feeding tubes (8 and 10 Fr) Nasogastric feeding tubes (8 and 10 Fr) |
 Needles and syringes Needles and syringes |
 Chest tubes (8 and 10 Fr) Chest tubes (8 and 10 Fr) |
 Magill forceps Magill forceps |
 Radiant warmer Radiant warmer |
 Cardiorespiratory monitor with electrocardiography leads Cardiorespiratory monitor with electrocardiography leads |
 Pulse oximeter with neonatal probes Pulse oximeter with neonatal probes |
 Suction equipment and tubing Suction equipment and tubing |
 Pulse oximeter with newborn probe Pulse oximeter with newborn probe |
 End-tidal CO2 detector End-tidal CO2 detector |
 Laryngeal mask airway (optional) Laryngeal mask airway (optional) |
| Drugs |
 Epinephrine 1:10,000 Epinephrine 1:10,000 |
 Naloxone Naloxone |
 Sodium bicarbonate Sodium bicarbonate |
 Dextrose in water 10% Dextrose in water 10% |
 Normal saline, lactated Ringer’s Normal saline, lactated Ringer’s |
 Resuscitation drug chart Resuscitation drug chart |
4 What are the critical facts in the history that should be elicited, if possible, prior to delivery?



7 How do you assess the condition of a newly born infant?
The basic principles for the newly born infant are the same as for any patient. However, there are particular problems of the neonate that bear special attention. After placing the neonate under the prewarmed radiant warmer on his or her back, dry and suction the baby (see Question 5). Carefully observe the respiratory effort and rate. If cyanosis or other signs of distress are noticed, administer oxygen. If the respiratory response is inadequate, stimulate the infant again and reposition. Adequacy of respirations is based on the rate (usually 35–60 breaths per minute), the effort (lack of retractions and grunting), and breath sounds. If the respiratory effort continues to be suboptimal (absent, slow, shallow), begin positive-pressure ventilation. If the respiratory effort is adequate, then evaluate the heart rate.
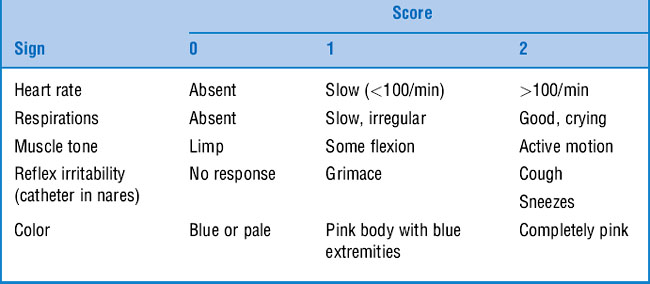
Finally, assign an Apgar score at 1 minute and at 5 minutes of life (Table 2-2). The Apgar score assesses heart rate, respirations, muscle tone, reflex irritability, and color. It indicates how the infant is doing or the responsiveness to the resuscitation. If the Apgar score is less than 7 at 5 minutes, continue scoring every 5 minutes. Do not delay resuscitative efforts to obtain an Apgar score.
10 What are the indications for tracheal intubation of the newly born infant?






11 How should endotracheal intubation of the newborn be performed?

The proper depth of insertion can be estimated by:

13 What is the proper technique for chest compressions in the newborn?
David R: Closed chest cardiac massage in the newborn infant. Pediatrics 81:552–554, 1988.
14 How does the resuscitation of the newly born infant differ if meconium is present in the amniotic fluid?
15 What are the most common drugs used in a neonatal resuscitation, and when are they indicated?
 Epinephrine is recommended when the heart rate remains below 60 beats per minute despite adequate ventilation with 100% oxygen and chest compressions for 30 seconds. Evidence from neonatal models shows increased diastolic and mean arterial pressures in response to epinephrine. The current recommended dose for epinephrine during the neonatal resuscitation is 0.01 to 0.03 mg/kg of 1:10,000 concentration (0.1–0.3 mL/kg). High-dose epinephrine is not recommended for neonates because of the rare incidence of ventricular fibrillation and the theoretical risk of a hypertensive response, which could result in intraventricular hemorrhage.
Epinephrine is recommended when the heart rate remains below 60 beats per minute despite adequate ventilation with 100% oxygen and chest compressions for 30 seconds. Evidence from neonatal models shows increased diastolic and mean arterial pressures in response to epinephrine. The current recommended dose for epinephrine during the neonatal resuscitation is 0.01 to 0.03 mg/kg of 1:10,000 concentration (0.1–0.3 mL/kg). High-dose epinephrine is not recommended for neonates because of the rare incidence of ventricular fibrillation and the theoretical risk of a hypertensive response, which could result in intraventricular hemorrhage.




16 Where is the best place to obtain IV access?
1 Prevent hypothermia. Although some studies have suggested that cerebral hypothermia of the asphyxiated infant may protect against brain injury, it is not routinely recommended pending controlled human studies.
2 Prevent hyperthermia because it has been associated with perinatal respiratory depression.
3 Use 100% oxygen with positive-pressure ventilation. Although some studies have shown that lower inspired oxygen is useful in some settings, this is not recommended because of insufficient data.
4 A laryngeal mask may be used as an alternative airway method by trained providers when bag-mask ventilation is ineffective or attempts at endotracheal intubation have been unsuccessful.
5 Confirm endotracheal intubation with CO2 detectors.
6 The two-thumb method of chest compressions is preferred for newborns, with the depth of compression being one-third of the anterior–posterior diameter of the chest rather than a fixed depth. Compression should be deep enough to generate a pulse.
7 Administer epinephrine if the heart rate remains 60 beats per minute after 30 seconds of adequate ventilation and chest compressions.
8 Albumin-containing solutions are no longer the fluid of choice for initial volume expansion. Isotonic crystalloids are the first choice.
9 Intraosseous access can be used if the umbilical vein is not readily available.
17 Are there circumstances when resuscitation of the newly born infant may not be the appropriate action?
[/level-membership-for-emergency-medicine-category][not-level-membership-for-emergency-medicine-category]
Chapter 2 Neonatal Resuscitation
2 What preparation is necessary for the unexpected emergency department (ED) delivery?
Preparation is key, as most ED deliveries are “unexpected.” A prearranged plan should be set in motion as soon as birth is imminent. That plan should include the assembly of personnel who are best able to take care of the newly born infant. A brief history should be obtained if possible because it may affect the resuscitation. Equipment and medications specifically for a neonatal resuscitation should be kept in a designated tray so they are quickly available (Table 2-1). Periodic inspection of this equipment for proper functioning and expiration dates of medication should become part of the routine upkeep of the neonatal resuscitation tray.
Table 2-1 Equipment and Drugs for the Neonatal Resuscitation
| Equipment |
| Gowns, gloves, and masks |
| Warm towels and blankets |
| Bulb syringe |
| Meconium aspirator |
| Suction catheters (sizes 5–10 Fr) |
| Face masks (sizes premature, newborn, and infant) |
| Oral airways (sizes 000, 00, 0) |
| Anesthesia bag with manometer (preferably 500 mL, no larger than 750 mL) |
| Laryngoscope with straight blades (sizes 0 and 1) |
| Spare bulbs and batteries |
| Stethoscope |
| Endotracheal tubes (sizes 2.5, 3.0, 3.5, 4.0) and stylet |
| Tape |
| Umbilical catheters (3.5 and 5 Fr) |
| Oxygen source with flow meter |
| Umbilical catheter tray |
| Three-way stopcocks |
| Nasogastric feeding tubes (8 and 10 Fr) |
| Needles and syringes |
| Chest tubes (8 and 10 Fr) |
| Magill forceps |
| Radiant warmer |
| Cardiorespiratory monitor with electrocardiography leads |
| Pulse oximeter with neonatal probes |
| Suction equipment and tubing |
| Pulse oximeter with newborn probe |
| End-tidal CO2 detector |
| Laryngeal mask airway (optional) |
| Drugs |
| Epinephrine 1:10,000 |
| Naloxone |
| Sodium bicarbonate |
| Dextrose in water 10% |
| Normal saline, lactated Ringer’s |
| Resuscitation drug chart |
