Chapter 57 Neonatal infections
Kohl S: Herpes simplex virus. In Behrman R, Kliegman R, Jenson H, editors: Nelson textbook of pediatrics. Philadelphia, 2004, WB Saunders, pp 1051–1057.
Jacobs RF: Neonatal herpes simplex virus infections, Semin Perinatol 22:64–71, 1998.
Smith CK, Arvin AM: Varicella in the fetus and newborn, Semin Fetal Neonatal Med 14:209–217, 2009.
Tolfvenstam T, Broliden K: Parvovirus B19 infection, Semin Fetal Neonatal Med 14:218–221, 2009.
Key Points: Neonatal Infection
DeVries J: The ABC’s of CMV, Adv Neonatal Care 7:248–255, 2007.
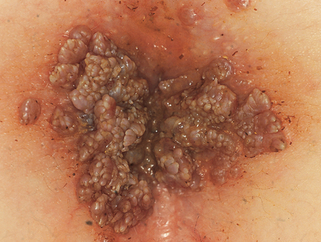
Anogenital warts in young children can also be acquired as a congenital infection, through sexual abuse, or by other postnatal, nonsexual contact with affected adults (Fig. 57-3).
Weston WL, Lane AT, Morelli JG: Color textbook of pediatric dermatology, St Louis, 2002, Mosby.