164
Necrobiosis lipoidica
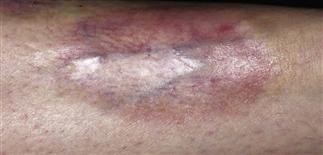
Necrobiosis lipoidica begins as a pink to violaceous oval asymptomatic patch that expands slowly. There is central atrophy of the patch with mild inflammation at the periphery.

Later, there is chronic inflammation and central ulceration followed by healing with bound-down scars. Treatment with intralesional corticosteroids may help control the spread of eruption.

More than 50% of patients with this condition are insulin-dependent. The majority of patients are female. The eruption is confined to the anterior surfaces of the lower legs in most cases.

One should look for diabetes mellitus in newly diagnosed cases, as symptoms may be subtle or subclinical.
DESCRIPTION
An inflammatory condition of degenertive collagen. When present, necrobiosis lipoidica is often associated with diabetes; therefore it is called necrobiosis lipoidica diabeticorum. However, only 1–2% of patients with diabetes develop necrobiosis lipoidica.
HISTORY
• More than 50% of individuals with necrobiosis lipoidica also have insulin-dependent diabetes. • Skin lesions may appear years before the onset of diabetes. • Lesions usually develop slowly and are often asymptomatic. • Onset may occur at any age, but the disease most commonly starts in the third or fourth decade. • About 75% of those affected are women.
PHYSICAL FINDINGS
• Lesions are usually limited to the anterior shins but may be seen on calves and thighs, and rarely on the arms, hands, feet, and scalp. • They begin as round, violaceous patches and slowly expand. The advancing border is red, and the central area turns a characteristic orange-yellow brown. The central area atrophies and shows a shiny, waxy surface with prominent telangiectasias. • Ulceration may occur, particularly after trauma, in about 15% of cases. These ulcers are exquisitely tender. • The number or severity of lesions or ulcerations has not been correlated with the degree of diabetic control. • The course is unpredictable. Lesions usually heal with atrophic scarring, or can be chronic and recurrent.
TREATMENT
• Topical and intralesional steroids slow the inflammation but may promote further atrophy. Middle- to high-potency corticosteroids can be used under occlusion. • Intralesional injections of triamcinolone acetonide 10 mg/mL can be helpful. • A short course (5–6 weeks) of oral corticosteroids can be considered if disease activity and symptoms are severe, but this is rarely the case. • Pentoxifylline (Trental) 400 mg t.i.d. has been advocated by some and has been used in combination with low-dose aspirin for ulcerating necrobiosis lipoidica. • Skin grafting can be performed for extensive disease.






