8 Multiple sclerosis
Introduction
Definition
It has been found that the central nervous system is able to overcome small areas of axon loss by finding ways to reroute messages around an area of damage through undamaged nerve cells. This ability to adapt in areas of damage is called plasticity. If the area of damage becomes too large, this rerouting process is no longer able to compensate and messages to or from that part of the central nervous system are permanently blocked, resulting in symptoms that do not improve. There seems to be a mixture of both grey and white matter affected by the demyelination process [1].
Mortality
It appears that only about half the patients suffering from MS eventually die of causes related directly to it. Respiratory disease or cardiovascular complications, mainly brought about by demyelinating lesions, involving brain regions that regulate cardiorespiratory activity, could be considered as the immediate cause of death. But poverty of movement, trauma or even poor nursing care are also problems. The standardized mortality ratio in a recent study indicated that MS sufferers were almost three times as likely to die prematurely compared to the general population [2] but MS was not always given as cause on the death certificate.
Diagnosis
Tests
Medical treatment
Pharmacology
The mechanism of action of interferon-β1b in MS is not clearly understood, but is thought to involve immunoregulatory activities, including enhancing the suppressor activity of peripheral blood mononuclear cells. In a recent study looking at patients with a single clinical event suggestive of MS, the relative risk of clinically definite (CD) MS was reduced by 41% in those receiving interferon-β1b 250 μg every other day for 3 years (early-treatment group) compared with patients who were initially randomized to placebo then switched to interferon-β1b 250 μg every other day at the end of 2 years or at the onset of CD MS (delayed-treatment group) (P < 0.01). [5]. Thus there is some evidence that early doses of this particular type of interferon may be helpful in preventing further development of symptoms in some patients, but much more work is needed [6].
MS and physiotherapy
Fatigue
Contributing factors such as loss of sleep, poor diet or lack of aerobic exercise will be assessed.
Contractures affecting joints
If there is no response then splinting and serial casting may be tried.
Pain and other problems
Acupuncture research in MS
Acupuncture has been recommended as a safe alternative intervention for pain relief in MS [8]. However there remains a question as to whether muscle spasm is sometimes made briefly worse by deep needling [9].
There have been two systematic reviews of acupuncture in general neurology [10, 11]; both reports have concluded that the studies included showed no definitive data on the use of acupuncture for MS, although there might be a positive influence on the secondary symptoms. However, Hopwood & White [12] advise caution in reading systematic reviews, stating the review quality and conclusions depend on the research work included, mentioning in particular the difficulties facing researchers in adequately controlling acupuncture trials. Some qualitative work, including that by Pucci et al. [13], indicates that the use of acupuncture by MS patients is quite high and 61.5% of the patients interviewed in the Pucci study claimed that acupuncture was beneficial.
Acupuncture has been found to have a consistently beneficial effect on insomnia, although the quality of studies has been variable [14]. Auricular acupuncture for insomnia has also been investigated [15], offering moderately positive evidence for acupuncture. The auricular points used were mainly in the helix so could indeed have affected the parasympathetic nervous system and thus provided a calming effect. These were not investigations specific to MS but they are relevant.
A recent review of the use of complementary therapies in MS included acupuncture [16] and patients described it as generally relaxing but also a treatment which increased their energy and feelings of well-being. More specifically they said it reduced pain, increased flexibility, improved balance and reduced recovery time from relapses. The text does not offer information on the type of acupuncture given but it is likely to be of the traditional type as Western health professionals do not generally include acupuncture in the ‘black box’ of therapies for MS yet.
Acupuncture treatment for MS
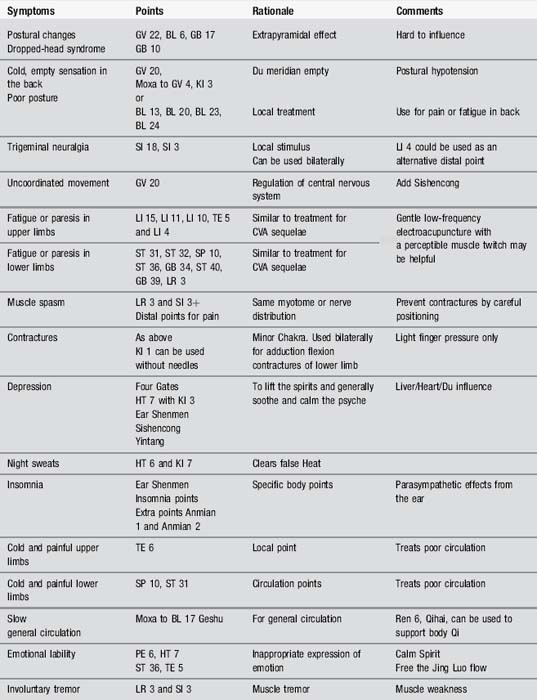
Considering the symptoms in Table 8.1, it is clear that acupuncture may be able to affect most of them.
| Symptom | Characteristic presentation | Multiple sclerosis |
|---|---|---|
| Decreased mobility | Rigidity |  |
| Fatigue | Lack of energy |   |
| Pain | X | |
| Muscle spasm | Tremor |  |
| Contractures | Stiffness and rigidity |  |
| Autonomic changes | Slowing circulation |   |
| Cognition/mood |




X, usually absent;  , common;
, common; 
 , very frequent.
, very frequent.
Body acupuncture
Body points can be selected according to local symptoms or according to the organ system that seems to be affected at the time. MS patients are subject to a considerable variation in severity of symptoms, and remissions and exacerbations are characteristic of the disease. A minimal selection of the appropriate points is necessary as overtreatment is very easy and patients can often be quite exhausted by their acupuncture treatment (Table 8.2). Needling is generally applied to the affected limbs.
Scalp acupuncture
This is occasionally used in MS but has no research evidence to support it. Logically, work on the motor or sensory cortical lines could be helpful when treating changes in limb function. Jiao Shunfa has made anecdotal claims that scalp acupuncture can help with pain, paralysis and vertigo in MS [17].
TCM approach
Traditional Chinese medicine (TCM) offers an apparently complex approach to what is a complex disease process but when considered as separate and distinct stages the syndrome theories can be easily applied. The most commonly adopted TCM staging for MS was originated by British acupuncturists Blackwell and MacPherson [18] and offers a logical framework for treatment.
MS can be considered as four stages (Table 8.3): the first stage is remission, either before the disease process has really started or, far more likely, as an interval where symptoms recede and a near-normal state is regained.
| Stage 1 | Stage 2 |
|---|---|
| Remission |
| Stage 3 | Stage 4 |
|---|---|
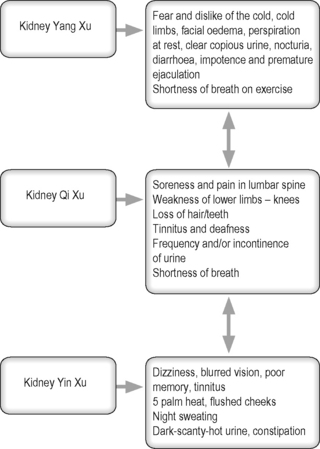
| Kidney Xu |
Stage 2: moving inwards (Damp Heat invades and obstructs channels)
Blackwell and MacPherson [18] offer a helpful differentiation between stages 2 and 3 (Table 8.4).
| Damp affecting the channels | Liver blood deficiency |
|---|---|
| Widespread numbness | Extremities numb and tingling |
| Heavy, aching limbs | Stiff limbs, increased muscle tone |
| Variable onset and progression | Slow gradual onset |
| Continuous symptoms | Symptoms much worse when the patient is tired |
| Emotions mostly unchanged, possible depression with generally low motivation | Either apathetic or anxious with tight, brittle emotions |
| Pulse full or normal | Pulse choppy or thready |
Stage 3.1: Spleen Qi Xu
Points to be used include Zusanli ST 36, Taibai SP 3, Zhangmen LR 3, Weishu BL 21, Sanyinjiao SP 6, Zhongwan CV 12 and Pishu BL 20. As usual, add points to deal with superficial or channel problems as necessary. Figure 8.1 shows how the different syndromes which may be present are interlinked and interdependent.
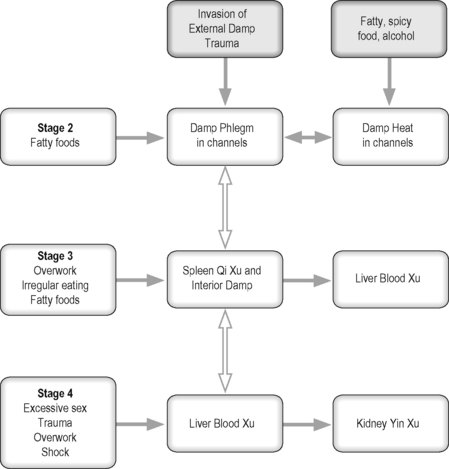
Figure 8.1 Moving through the stages of multiple sclerosis in traditional Chinese medicine terms.
After Blackwell and MacPherson [18].
Other syndromes which may occur in MS
Phlegm Heat agitating Wind (affecting Liver)
Case study 8.2: level 3 case study
Assessment
Objective assessment revealed the following:
Treatment
Treatment 2
2 days later, 10 minutes in supine.
Points: GB 34 Rt, +7 TPs in quadriceps muscles.
Research has reported that treating patients with MS with acupuncture provoked spasms, clonus and even tonic-clonic muscle contractions of the extremity muscles [20]. Similarly, this patient experienced an increase in right leg flexor spasms during acupuncture, perhaps because a deep insertion was used, making the treatment very uncomfortable. This made it too difficult to insert needles on the anterior of the hip (such as at ST 31), and the needles were removed after 5 minutes of the first treatment.
Treatment 4
4 days later; repeated treatment +BL 62 (opening point for GV meridian)
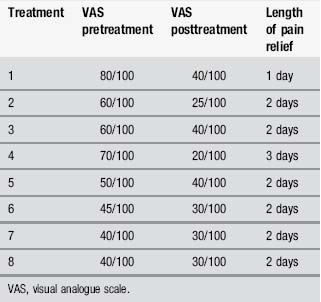
Table 8.5 gives details of pre- and posttreatment measures for right hip pain. As can be seen from Table 8.1, acupuncture provided good temporary pain relief, lasting between 1 and 3 days. Some of the acupuncture-induced analgesia was maintained over the course of treatment. The client reported the worst pain was 40/100 on completion of the course of acupuncture, a 50% reduction from the worst pain experienced before acupuncture treatment commenced.
[1] Gilmore C.P., Donaldson I., Bo L., et al. Regional variations in the extent and pattern of grey matter demyelination in multiple sclerosis: a comparison between the cerebral cortex, cerebellar cortex, deep grey matter nuclei and the spinal cord. J Neurol Neurosurg Psychiatry. 2009;80(2):182-187.
[2] Hirst C., Swingler R., Compston D.A., et al. Survival and cause of death in multiple sclerosis: a prospective population-based study. J Neurol Neurosurg Psychiatry. 2008;79(9):1016-1021.
[3] Callander M., Landtblom A.M. A cluster of multiple sclerosis cases in Lysvik in the Swedish county of Värmland. Acta Neurol Scand. 2004;110(1):14-22.
[4] Peterli B., Ristic S., Sepcic J., et al. Region with persistent high frequency of multiple sclerosis in Croatia and Slovenia. J Neurol Sci. 2006;247(2):169-172.
[5] McKeage K. Interferon-beta-1b: in newly emerging multiple sclerosis. CNS Drugs. 2008;22(9):787-792.
[6] Rojas J.I., Romano M., Ciapponi A., et al. Interferon beta for primary progressive multiple sclerosis. Cochrane Database Syst Rev. (1):2009.
[7] NICE. Management of multiple sclerosis in primary and secondary care. National Collaborating Centre for Chronic Conditions, editor. Clinical Guideline. 8, 2003. 13–6-0009
[8] van den Noort S., Holland N.J. Multiple Sclerosis in Clinical Practice. New York: Demos Medical Publishing, 1999.
[9] Donnellan C.P., Shanley J. Comparison of the effect of two types of acupuncture on quality of life in secondary progressive multiple sclerosis: a preliminary single-blind randomized controlled trial. Clin Rehabil. 2008;22(3):195-205.
[10] Lee H., Park H.J., Park J., et al. Acupuncture application for neurological disorders. Neurol Res. 2007;29(Suppl. 1):S49-S54.
[11] Rabinstein A.A., Shulman L.M. Acupuncture in clinical neurology. Neurologist. 2003;9(3):137-148.
[12] Hopwood V., White P. Poor reviews may not give a true reflection of the evidence. Physiotherapy. 2001;87:549-551.
[13] Pucci E., Cartechini E., Taus C., et al. Why physicians need to look more closely at the use of complementary and alternative medicine by multiple sclerosis patients. Eur J Neurol. 2004;11(4):263-267.
[14] Kalavapalli R., Singareddy R. Role of acupuncture in the treatment of insomnia: A comprehensive review. Complement Ther Clin Pract. 2007;13(3):184-193.
[15] Sjoling M., Rolleri M., Englund E. Auricular acupuncture versus sham acupuncture in the treatment of women who have insomnia. J Altern Complement Medicine (New York, NY). 2008;14(1):39-46.
[16] Esmonde L., Long A.F. Complementary therapy use by persons with multiple sclerosis: Benefits and research priorities. Complement Ther Clin Pract. 2008;14(3):176-184.
[17] Jiao S. Scalp Acupuncture and Clinical Cases. Beijing: Foreign Languages Press, 1997.
[18] Blackwell R., MacPherson H. Multiple sclerosis. Staging and patient management. J Chin Med. 1993;42:5-12.
[19] Maciocia G. The Practice of Chinese Medicine. Churchill Livingstone: Edinburgh, 1994.
[20] Steinberger A. Specific irritability of acupuncture points as an early symptom of multiple sclerosis. Am J Chin Med. 1986;14(3–4):175-178.