[level-membership-for-obstetrics-gynecology-category]
13 Multiple pregnancy, breech and abnormal presentations
Malpresentations
Breech
The presentation of the fetus refers to the part of the fetus that occupies the lower uterine segment, which in this case is the fetal buttocks. This is the commonest malpresentation, occurring in 3–4% of singleton pregnancies at term, but in up to 25% in preterm labour. There are three types of breech presentation (Fig. 13.1):
1. Frank breech – buttocks presenting with the legs extended.
2. Complete breech – legs flexed so that feet present beside the buttocks.
3. Footling breech – one or both feet presenting below the buttocks.
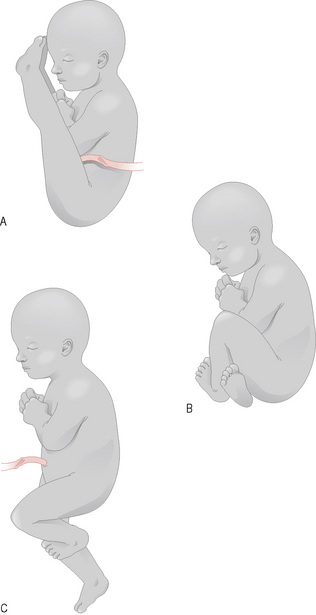
Figure 13.1 Breech presentations. (A) Extended (frank); (B) flexed (complete); (C) footling.
(Redrawn with permission from Rymer J, Davis G, Rodin A et al. 2003 Preparation and Revision for the DRCOG, 3rd edn. Edinburgh: Churchill Livingstone, p. 235.)
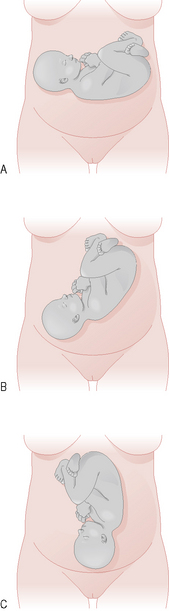
Transverse (and oblique) lie
The aetiologies of both these presentations are similar to those outlined for breech presentation and also an ultrasound assessment should be performed for the same reasons (Fig. 13.2).
Multiple pregnancy
Management
1. Diagnosis – women will often have exaggerated symptoms of pregnancy, including hyperemesis gravidarum. On examination the uterus feels larger than would be expected for her dates. Ultrasound assessment is usually performed in all pregnancies and should reveal the diagnosis.
2. Multiple pregnancy is not a normal pregnancy and should be closely monitored.
3. Both congenital abnormality and intrauterine growth restriction (IUGR) are more common in multiple pregnancy and so regular ultrasound assessment is important at 28, 32 and 36 weeks or more frequently if necessary.
4. An early ultrasound scan should determine chorionicity at 12 weeks or less.
Complications of multiple pregnancy
Maternal
Fetal
• Perinatal mortality is increased fourfold
• Congenital abnormality, especially in monozygotic twins
• Preterm labour occurs in 40% of twin pregnancies. More than 50% of babies from multiple pregnancies are less than 2500 grams compared with 6% of babies from singleton pregnancies
• Placental insufficiency or IUGR, especially in monochorionic twins
• Twin–twin transfusion in monochorionic twins, due to anastomosis of vessels within the single placental mass of a monochorionic twin pregnancy. In this condition one twin gains at the expense of the other, i.e. one twin becomes anaemic and the other polycythaemic
Summary
• All women with a malpresentation should deliver in hospital.
• Breech presentation is associated with an increased perinatal mortality rate and, therefore, is considered a high-risk pregnancy.
• Transverse and oblique lie at term are uncommon and women should be admitted after 37 weeks as cord prolapse is more common in these situations and is an obstetric emergency.
• Multiple pregnancies have significantly increased fetal and maternal morbidity and mortality and, therefore, require regular specialist monitoring.
[/level-membership-for-obstetrics-gynecology-category][not-level-membership-for-obstetrics-gynecology-category]
13 Multiple pregnancy, breech and abnormal presentations
Malpresentations
Breech
The presentation of the fetus refers to the part of the fetus that occupies the lower uterine segment, which in this case is the fetal buttocks. This is the commonest malpresentation, occurring in 3–4% of singleton pregnancies at term, but in up to 25% in preterm labour. There are three types of breech presentation (Fig. 13.1):
1. Frank breech – buttocks presenting with the legs extended.
2. Complete breech – legs flexed so that feet present beside the buttocks.
3. Footling breech – one or both feet presenting below the buttocks.
Figure 13.1 Breech presentations. (A) Extended (frank); (B) flexed (complete); (C) footling.
(Redrawn with permission from Rymer J, Davis G, Rodin A et al. 2003 Preparation and Revision for the DRCOG, 3rd edn. Edinburgh: Churchill Livingstone, p. 235.)
