Appendiceal Mucocele
Synonyms/Description
Etiology
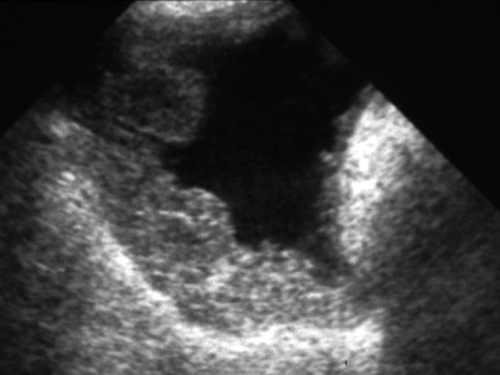
Ultrasound Findings
Differential Diagnosis
Clinical Aspects and Recommendations
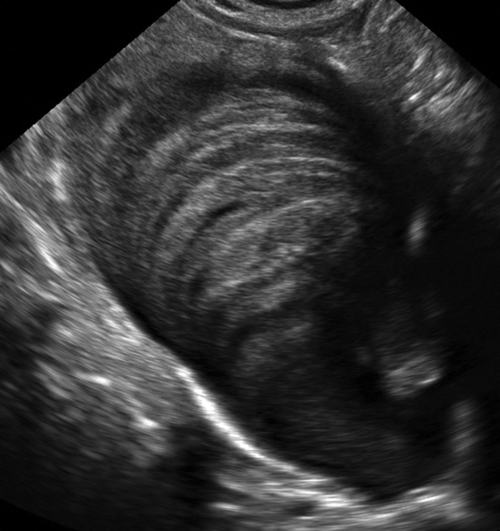
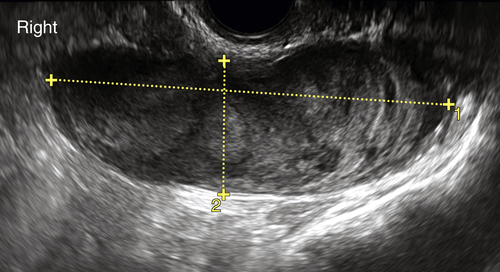
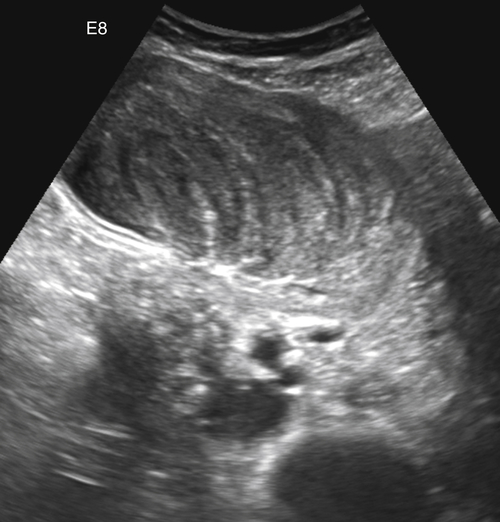
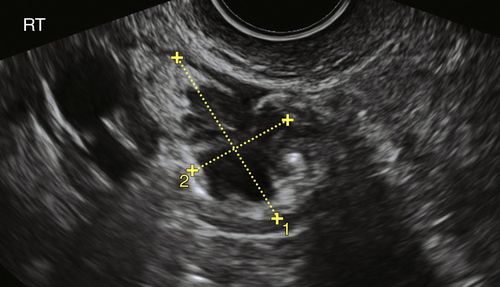
Figures
Suggested Reading
Caracappa D., Gullà N., Gentile D., Listorti C., Boselli C., Cirocchi R., Bellezza G., Noya G. Appendiceal mucocele. A case report and literature review. Ann Ital Chir. 2011 May-Jun;82(3):239–245.
Dragoumis K., Mikos T., Zafrakas M., Assimakopoulos E., Venizelos I., Demertzidis H., Bontis J. Mucocele of the vermiform appendix with sonographic appearance of an adnexal mass. Gynecol Obstet Invest. 2005;59:162–164.
Papoutsis D., Protopappas A., Belitsos P., Sotiropoulou M., Antonakou A., Loutradis D., Antsaklis A. Mucocele of the vermiform appendix misdiagnosed as an adnexal mass on transvaginal sonography. J Clin Ultrasound. 2012;40:522–525.
Pickhardt P.J., Levy A.D., Rohrmann C.A., Kende A.I. Primary neoplasms of the appendix: radiologic spectrum of disease with pathologic correlation. RadioGraphics. 2003;23:645–662.
Witkamp A.J., de Bree E., Kaag M.M., van Slooten G.W., van Coevorden F., Zoetmulder F.A. Extensive surgical cytoreduction and intraoperative hyperthermic intraperitoneal chemotherapy in patients with pseudomyxoma peritonei. Br J Surg. 2001;88:458–463.
Yabunaka K., Katsuda T., Sanada S., Fukutomi T. Sonographic appearance of the normal appendix in adults. J Ultrasound Med. 2007;26:37–43.






