Movement analysis across the life span
DALE SCALISE-SMITH, PT, PhD and DARCY A. UMPHRED, PT, PhD, FAPTA
After reading this chapter, the student or therapist will be able to:
1. Comprehend the complexity and interlocking nature of human development over a lifetime.
2. Differentiate traditional theories of development from contemporary theories.
3. Analyze the differences among various subsystems within the human organism.
4. Identify elements of physiological changes over a lifetime.
5. Analyze normal movement strategies and identify subsystems responsibility for success of a motor task.
6. Identify normal changes in motor strategies over a lifetime and synthesize differences between normal movement patterns and pathological movement problems across the life cycle.
Throughout much of the twentieth century, developmental researchers were heavily focused on skill acquisition from infancy through early childhood.1–3 In the 1970s, as research paradigms directed at motor development and motor learning evolved, it became evident that changes in motor skills were not limited to childhood but occurred throughout the life span. Consequently, the concept of life span development came to incorporate the prenatal period through older adulthood.
During infancy (birth to 1 year) and childhood (1 year to 10 years) acquisition of motor skills coupled with cognitive and perceptual development are the primary foci of developmental researchers and clinicians. As the young child transitions to adolescence (11 to 19 years) and has the opportunity to experience motor behaviors across different environmental contexts, more complex behaviors emerge. Adulthood (20 to 59 years) signals a period when skills are refined and motor behaviors mature. Only through practice and repetition are skills attained and retained. Individuals who continue to use motor learning strategies into late adulthood (60 years through death) often report more successful aging than those who do not engage in such motor skills.4
Identifying mechanisms that enable individuals to be successful in acquisition and retention of functional motor behaviors is critical to examining variables that alter or impair these same behaviors in other individuals. Kandel and colleagues5 suggested that “the task of neural science is to understand the mental processes by which we perceive, act, learn, and remember” (p. 3). This view supports the interactive and collaborative nature of intrinsic and extrinsic systems to accomplish motor learning tasks.
Theories of development
Development is often portrayed as a series of stages through which an infant progresses, with a fixed order to the sequence.6 A developmental theory may be characterized as a systematic statement of principles and generalizations that provides a coherent framework for studying development. Historically, development was thought to be linear, occurring in an invariant sequence and resulting in behavioral changes that are direct reflections of the maturation of anatomical and physiological systems.7,8 Development is generally examined in terms of quantitative and qualitative change. Although it is universally accepted that acquisition of developmental skills is not reversible, the underlying principles surrounding the emergence of these behaviors has evolved over the past 50 to 75 years.
Early developmental theorists used neuromaturational models of CNS organization as the framework for conceptualizing development.1,2 These researchers provided elaborate descriptions of posture acquisition and a blueprint delineating skill development. Research focused on the emergence of cognitive and affective behaviors and ignored the processes and mechanisms involved in acquiring motor skills.9 Several investigators attributed developmental changes to intrinsic variables such as maturation of the CNS, whereas others associated changes with extrinsic variables involving the environment.1,2,10,11
During the 1930s and 1940s, Arnold Gesell and Myrtle McGraw led a cadre of avant-garde researchers exploring the field of infant motor development. Gesell1,12 described the normative time frame for when behaviors emerge, and McGraw2 examined the underlying mechanisms responsible for the emergence of these behaviors. The underlying premise, the foundation for their elaborate descriptions of motor development, was based on maturational processes in the CNS.
Gesell, a pioneer in developmental research, was a proponent of the theory that nature drives development.13 He proposed that growth is a process so complicated and so sensitive that intrinsic factors are solely responsible for influencing development. He used the evolutional thinking of Darwin and Coghill to explain changes in motor behaviors. Coghill,14 in his work with salamander embryos, reported that motor behaviors, like swimming, emerge in an orderly sequence as connections of specific neural structures appear. Coghill concluded from his observations of emergence of behaviors in the salamanders that human infant motor behaviors appear in a predictable sequence and at predictable chronological ages.
With Coghill’s research as the foundation for his thinking, Gesell embraced the concept of a hierarchical organization of the CNS. He believed that the emergence of motor behaviors was contingent on maturation in the CNS and concluded that only after the emergence of higher-level neural structures would complex motor behaviors appear. Within this constrained theoretical perspective, extrinsic or environmental stimuli, human or otherwise, were thought to have little impact on the appearance of motor behaviors. Gesell concluded that infant development is preprogrammed and linear, emerging at predetermined stages or periods in time.13 Perhaps his greatest contribution to motor development was the conceptualization of milestones as markers to evaluate infant behavior.
Although McGraw was a proponent of ontogenic development as one variable influencing motor development, she did not believe, as Gesell did, that it was the sole determinant.15 Rather, McGraw attempted to explain the emergence of motor behaviors through environmental influences as well as CNS maturation.2 She examined the temporal and qualitative aspects of motor skill acquisition through her study of Jimmy and Johnny,16 a study of twin brothers in which one twin was provided an exercise program, whereas no intervention was afforded the other twin. She found temporal and qualitative differences in the boys’ acquisition of motor skills and attributed differences in acquisition of these behaviors to disparities in practice opportunities.
Sufficient evidence exists to support the premise that although some predetermined processes occur at relatively similar points in development, not all motor behaviors emerge at the same biological, chronological, or psychological age in every individual. Although motor milestones provide information regarding outcome, no information can be derived about the process of attaining motor skills from those specific milestones. Perhaps a more realistic explanation may be that emergence of new skills occurs out of a need to solve specific problems within the environment. Working within this context, it is evident that traditional theories of development and maturation fail to adequately encapsulate the innate variability in human development.9,10
Within the last few decades, researchers have used more current theories of development when designing studies involving infants and young children.17–19 These investigators examined the process of skill acquisition rather than using traditional methods that assess outcome as a measure of motor development.20
Although early pioneers in developmental research described development as linear, uniform, and sequential, Thelan and Smith21 depict development as “messy,” “fluid,” context-sensitive, and nonlinear. Linear and nonlinear dynamics are derived from mathematics. Linear dynamics is described by the proportional relationship of the initial condition to the outcome, whereas no such proportional relationship exists in nonlinear dynamics. Nonlinearity is used to describe complex systems, in this case biological or more specifically human systems.22 Within these complex systems exists a level of unpredictability, given the interactive and interdependent nature of biological systems.
Thelan and Smith21 suggested that, although traditional theories of development support the premise that behaviors emerge in accordance with a relatively fixed temporal sequence, an organism may exhibit “precocial” abilities when the context is altered and the behavior emerges earlier than expected. These authors stated that immature systems exhibit behaviors that are variable and easily disrupted. Although development of some organisms in a controlled laboratory environment may reflect more traditional perceptions of development, outside, in a more naturalistic environment, development is more likely to be flexible, fluid, and tentative. Thelan and Smith also found that factors most likely to have an impact on performance are the “immediacy of the situation” and the “task at hand” rather than “rules” of the performance. Given this perspective, Thelan and Smith21 identified six goals as essential to developmental theory. These goals are as follows:
1. To understand the origins of novelty.
2. To reconcile global regularities with local variability, complexity, and context-specificity.
3. To integrate developmental data at many levels of explanation.
4. To improve a biologically plausible yet non-reductionist account of the development of behavior.
5. To understand how local processes lead to global outcomes.
6. To establish a theoretical basis for generating and interpreting empirical research.21 (p. xviii)
Thelan and Smith urged developmental researchers to devise paradigms that attempt to explain development in terms of diversity, flexibility, asynchrony, and “the ability of even young organisms to reorganize their behavior around context and task” (p. 18).21
Contemporary theorists inferred that developmental changes are nonlinear and emergent and may be the result of the interactive effects of intrinsic and extrinsic variables. This divergence from traditional thinking compelled avant-garde scholars to propose new theories.21,23,24 Investigators described behaviors as complex, interactive, cooperative, and reflects an ability to organize and regroup around task and context, rather than conforming to a rigid structure and rule-driven hierarchy, as many earlier cognitive researchers believed.21,24 Contemporary theorists exploit technology to derive a model to explain variability and flexibility in developing, mature, and aging populations.24
General systems theory
Systems theory, first described by von Bertalanffy in 1936, was not discussed in great detail until 1948. In 1954 von Bertalanffy and colleagues from three other professions met to discuss systems movement.25 Theorists then applied systems theory to a variety of human and nonhuman systems. As theorists became acquainted with systems theory, they became more receptive to alternate theoretical proposals of growth and development in living organisms.
Systems theory may be applied as a transdisciplinary model examining relationships of structures as a whole.26 “The notion of a system may be seen as simply a more self-conscious and generic term for the dynamic interrelatedness of components”26; von Bertalanffy proposed this theory to more adequately describe biological systems, investigate principles common to all complex organisms, and develop models that can be used to describe them.26
Principles that embody general systems theory include nonsummative wholeness, self-regulation, equifinality, and self-organization.26 Contrary to systems theory in disciplines such as traditional physics, in which systems are said to be closed, von Bertalanffy suggested that biological systems are open and modifiable and that changes in the system are the result of the dynamic interplay among elements of the system.26
Embedded in the general systems theory is nonlinear dynamics, a concept in which behaviors are not described as the sum of their parts. Thus within a nonlinear model, a mathematical model is derived.24,27 Characterized within this model is the notion that systems may change in a sudden, discontinuous fashion. During development a small increase or decrease in one parameter leads to changes in the behavior. This abrupt change, identified as a bifurcation, causes the system to move out of its previous state and toward a new state of being.
Throughout development, periods of rapid differentiation or change occur when an organism is most easily altered or modified. These periods were identified by Scott28 as “critical periods.” Physiological systems are most vulnerable during these periods and may be seriously affected by both intrinsic and extrinsic factors acting on the system. These periods occur at different times for different body systems. Understanding systems theory and the concept of critical periods is crucial to all aspects of motor development.
As scientists began to revisit theories of motor development, they discarded some of the traditional theories and embraced contemporary concepts of nonlinear dynamics.24,25,27 Proponents of nonlinear dynamics contend that modifications in motor behaviors are the result of dynamic interactions among the musculoskeletal, peripheral and central neuromuscular, cardiovascular and pulmonary, and cognitive and emotional systems.26 These interactive, multidimensional elements are vulnerable to changes in organizational and behavioral abilities (system) over time.28,29 Some theorists propose that as skills are acquired and organizational or behavioral changes occur, the system is driven to identify the most efficient and effective strategy to produce motor behavior(s).28,29 Yet others purport that variability implies that typical healthy individuals may use a variety of strategies to produce the same behavioral outcome and that variability is an indication of the individuals’ flexibility in responding to unpredictable perturbations.24,30 Implicit in nonlinear dynamics is the concept of critical periods in development.28,29,31 Investigators suggested that interventions imposed during a critical period may more easily positively or negatively modify the behavior. Recognizing the crucial role systems theory and critical periods play in development is vital to comprehending how developmental skills emerge. The multifactorial nature of nonlinear dynamics illustrates the complexity of development and the difficulty in identifying the appropriate variables that influence motor skill development.
With use of concepts previously described, it is reasonable to expect that a small change in any subsystem may result in a large change in a motor behavior. This is evident in work by Thelan and colleagues examining stepping in infants 8 weeks of age.29,31–34 They reported that introducing a small change in one element of the system, identified as a small weight applied to an infant’s leg, resulted in the infant being unable to step. The authors deduced that small changes in one subsystem, in this case the musculoskeletal system, may result in a change in the outcome. This lends support to the hypothesis that modifying one aspect of a multicomponent system, especially during a critical period, may cause the system to evolve into an entirely new behavior.
Menopause may be another critical period. During menopause, decreases in hormone production are thought to lead to osteoporosis and cardiac disease.35 Examples described previously provide evidence across the life span that the dynamic interplay within a system and among systems may significantly influence emergence and disappearance of behaviors.
Although research in the beginning of the twentieth century was heavily focused on development of the very young, studies during the latter part of the century were directed toward research on aging. Technological advances in medicine have dramatically increased life expectancies. During the twentieth century, the number of individuals in the United States older than 65 years old grew from 3 million to 35 million.36 Perhaps the most significant statistic is that the oldest old grew from 100,000 in 1900 to 4.2 million in 2000.36 By 2011 the Baby Boomer generation will begin turning 65 years old, and the number of older individuals will increase sharply between 2010 and 2030.36 By 2030, Americans over the age of 65 years will represent nearly 20% of the population, and by 2050 the number of individuals over the age of 85 years could grow to 21 million.36 Given this incredible demographic transformation and that current policymakers are, in large part, the generation directly affected by these statistics, a significant paradigm shift in funded research has evolved over the past quarter century. “As such, aging and death are inseparable partners to growth and development”37 (p. 32). Recognizing that a critical mass of Americans are entering older adulthood, terminology that operationally defines and is then applied consistently when referring to the aging population or an individual is imperative.
Biological and chronological age
Age can be described in terms of chronological age and biological age.38 Chronological age is the period of time that a person has been alive, beginning at birth. In infants it is measured in days, weeks, or months, whereas in adults it is expressed in terms of years and at times decades.
Although chronological age is measured in terms of temporal sequencing, biological age is related more to functioning and physiological aging of organ systems.39 For example, a triathlete may have biologically younger cardiovascular and pulmonary systems than same-age peers who do not perform high-level aerobic activities. Another example might be a child who underwent precocious puberty. Precocious puberty, identified as puberty earlier than 8 years of age in girls and 9.5 years in boys, results in acceleration in a biological system before same-chronological-age peers.40 Physiological changes include elevated hormonal levels, which would then stimulate development of breast tissue and early menstruation in girls. Changes in the musculoskeletal system include early closure of the epiphyseal plates, resulting in significantly smaller stature. Conversely, these young women’s reproductive cycles are significantly skewed. Women would also have menopause and aging issues associated with hormonal changes earlier than other women of the same chronological age. Although no consistent method has been established for measuring biological age, there is general agreement that a wide variability of biological aging exists and that a number of factors contribute to accelerated or decelerated biological aging.
Aging
“Aging refers to the time-sequential deterioration that occurs in most animals including weakness, increased susceptibility to disease and adverse environmental conditions, loss of mobility and agility, and age-related physiological changes” (p. 9).41 Although Goldsmith’s description of aging is typically viewed as an inevitable fact of life, there is scientific evidence and theoretical support for the idea that age-related changes will eventually be more medically treatable than previously thought.38,41,42
Scientists are hesitant to attribute a decline in functional movement in older adults to a decline in physiological systems or to diminished opportunities for practice or conditioning.4 Rowe and Kahn reported that “with advancing age the relative contribution of genetic factors decreases and [of] the nongenetic factors increases” (p. 446).4 Age-related factors that are modifiable may be used to identify individuals who may or may not age successfully. For instance, lifestyle choices, including diet, physical activity, and other health habits, and behavioral and social factors have a potent effect and accelerate or decelerate aging. Evidence to support this was initially derived from a 10-year study conducted by Rowe and Kahn.43 The authors identified three critical factors that contribute to aging successfully: avoidance and absence of disease, maintaining cognitive and physical functioning, and “sustained engagement in life.”43 Recently researchers suggested that Rowe and Kahn’s classification of successful aging is too restrictive and may lead to classifying individuals with relatively minor health problems as unhealthy. McLaughlin and colleagues44 suggested that a critical variable in defining successful aging is first identifying what the goal is for measuring successful aging. Only then can researchers determine how best to define and measure successful aging. Although controversy exists regarding defining successful aging, factors that contribute to successful aging hinge on higher levels of physical activity, increased social interactions, and positive perception of health, as well as no smoking, chronic diseases (arthritis, diabetes), or impaired cognition.45,46 Consequently, developing healthy behaviors early in life may be critical to maintaining good health and may play a significant role in successful aging. Factors associated with aging are generally identified as either age related or age dependent. Age-dependent changes within organ systems are observed in individuals at a similar age, whereas age-related changes may be accelerated or decelerated in same-age individuals on the basis of intrinsic or extrinsic factors related to lifestyle. Just as variables associated with lifestyle (extrinsic factors) influence aging, genetics (intrinsic factors) also play a significant role. From a genetic perspective, structural and functional changes are generally thought to be a consequence of aging and are therefore predictable and consistent across physiological systems. Variables thought to influence the genetic potential for longevity include environmental factors such as toxins, radiation, and oxygen free radicals. Free radicals are highly reactive molecules produced as cells turn food and oxygen into energy.47 In summary, the use of biological age rather than chronological age may be a more accurate reflection of an individual’s true age.
Theories of aging
Scientists view aging as a progressive accumulation of changes over time that increases the probability of disease and death.48 Given that portrayal of aging, researchers have proposed myriad hypotheses regarding aging. Aging theories evolved because there is no single factor or mechanism responsible for physiological aging.38 Biological aging theories, similar to developmental theories, are attributed to complex, underlying mechanisms.38,41,42,49 Although theorists attempt to classify aging theories, these theories are rarely mutually exclusive. Some theories were formulated around control of physiological functioning, others around cellular changes, and still others around genetic causes.
Neuroendocrine theory is based on the premise that hormones play a significant role in aging.42,49 Hormones are vital to repairing and regulating bodily functions. Hormone production decreases significantly during aging and limits the body’s ability to repair and regulate itself as effectively. Although hormonal decline is one plausible explanation for age-related changes, it does not account for all changes. Harman50 proposed the free radical theory on the basis of his investigations that examined the effects of radioactive materials on human tissue.50
Harman reported that when human tissue is exposed to radiation, a byproduct is formed. He identified the byproduct, an unstable compound, as a free radical. Over time, human tissue with free radicals showed evidence of biological defects consistent with accelerated aging. Harman postulated that accumulation of free radicals in human tissue may also occur as a part of the normal aging process. This became known as the free radical theory of aging.50–52
Free radicals are highly reactive molecules that damage proteins, lipids, and deoxyribonucleic acid (DNA). In some instances the free radicals combine with enzymes and turn into water and a harmless form of oxygen that moves harmlessly through the cells.51 In other instances the oxygen binds with intrinsic or extrinsic sources that influence the aging process.
Scientists have suggested several different ways that free radicals influence aging through intrinsic and extrinsic mechanisms.51,52 An example of an intrinsic mechanism would be chronic infections that extend phagocytic activity and expose tissues to oxidants, creating cumulative oxidative changes in collagen and elastin. Extrinsic sources of free radicals include environmental toxins—for example, industrial waste and cigarette smoke.
Human exposure to intrinsic and extrinsic free radicals causes large numbers of reactive oxygen molecules to interact with DNA, leading to mutations thought to be the cause of a variety of diseases, including cancer, atherosclerosis, amyloidosis, age-related immune deficiency, senile dementia, and hypertension. Although some scientists suggest that aging has many factors that can accelerate or decelerate the process, other scientists suggest a much simpler, preprogrammed theory, known as the Hayflick limit.38,51–53
Hayflick and Moorhead53,54 proposed that there is a finite number of times that a normal cell is capable of dividing. Current thinking is that cells are capable of dividing up to 50 times. Cell division is recognized as one way in which cells age and, after attaining the maximum number of divisions, finally die.
The factor thought to limit a cell’s ability to divide infinitely is the presence of telomeres. Telomeres are minute units at the end of the DNA chain.53 Each time a cell divides a small amount of the telomere is used in the process. Eventually, when cells have exhausted the supply of telomeres available, the cell is unable to divide and cell death ensues.
Telomerase, a substance that can lengthen telomeres, is available in human cells. Typically, telomerase is switched off in all cells except the reproductive cells. The availability of telomerase in reproductive cells allows for many more divisions than previously observed in the Hayflick limit. In addition to the presence of telomerase in reproductive cells, scientists have also discovered that telomerase remains active in cancer cells. Both reproductive and cancer cells divide well beyond the 50-division limit. Consequently, scientists are now working toward activating telomerase in all cells to slow or stop aging. If scientists are successful in activating telomerase in other cells, it may stimulate skin cell regrowth for burn patients and cure diseases that result from failure of aging cells to divide, as in macular degeneration or Hutchinson-Guilford progeria syndrome.55,56 The downside of this is that scientists may have a difficult time controlling the telomerase and in fact may see more uncontrolled cell growth—cancer—one of the greatest threats to prolonged existence.
Although many aging theories are directed at mechanisms that negatively influence aging, other theories are focused on factors that have a positive impact on aging processes. One such process is the caloric restriction theory.50,52,53,57 Liang and colleagues,57 with use of several genetic mouse models, investigated the impact of dietary control on the life span. The authors reported that the mice did, in fact, have their life spans extended when their dietary intake was controlled. Although these findings are potentially significant, given the small sample size and model examined, these data were not generalizable to all species. The researchers suggested that these preliminary data provide a foundation for scientists to examine whether dietary control will extend the life span in humans as it did in the mouse models.
Although a large body of literature exists examining the underlying mechanisms associated with aging, it seems inconceivable that any one mechanism is responsible for age-related changes. More likely is that aging may be attributed to multiple factors, including lifestyle choices, in combination with the physiological and environmental factors.58 Garilov and Gavrilova58 conducted an exhaustive review of aging theories and concluded that additional research is necessary to further elaborate and validate existing aging theories and dispel unlikely theories.
In summary, scientists are unsure how much of the decline in motor behaviors in older adults is attributable to true decline in physiological systems, how much is attributable to expected decline, how much to a decreased ability to perform skilled behaviors under variable conditions, and how much to decreased practice or conditioning.59–62 This suggests that physical or occupational therapy intervention may provide older adults with strategies to positively influence successful aging rather than being applied only after a negative outcome of aging is realized or a neurological insult has occurred.
Physiological changes in body systems across the life span
Musculoskeletal system
Skeletal muscle tissue first appears during the fifth week of embryonic development and continues to develop into adulthood.53,63 During this early period of embryonic development, the differentiation of musculoskeletal system is rapid: during the fifth week of embryonic life the limb buds appear, by the seventh week muscle tissue is present in the limbs, and limb movements emerge as early as the eighth week of prenatal life.40,64,65
Whereas many of the structural aspects of the musculoskeletal system are formed prenatally, muscle and bone continue to grow into adulthood. Motor skill acquisition involves considerable variability among young children from age 5 months through 3 years. During this time, the rate of growth of muscle tissue is reportedly two times faster than that of bone.66
Distinct differences also exist in temporal differentiation of the muscular systems of males and females of the same chronological age. Through adolescence, boys show evidence of a significantly greater increase in fiber size compared with girls.67 In addition, differences exist in the age at which the number of muscle fibers dramatically increases. Girls reportedly have a steady increase in the muscle fibers from 3.5 to 10 years of age. In contrast, boys have two periods of rapid differentiation in the number of muscle fibers. The first period occurs from birth until 2 years of age and the second from ages 10 to 16 years.67 Although the pace slows considerably, muscle fiber development continues in men and women well into middle adulthood.
Age-related changes evident in the musculoskeletal system include decreased fiber size, loss of muscle mass, denervation of muscle fibers, decline of total muscle fiber number, and decreased quantity of fast-twitch fibers.68–70 Muscle mass decreases beginning at around age 50 years, and by age 80 years up to 40% of muscle mass has been lost.71 Muscle force production likewise decreases at a rate of about 30% between 60 and 90 years of age. Additional musculoskeletal changes documented in older adults include decreased tensile strength in bone, reduced joint flexibility, and limited speed of movement. Decreased muscle mass in a person older than 60 years may be attributed to decreased size, fewer type II muscle fibers, and an increase in fat infiltration into the muscle tissue.72,73 Clinically these factors manifest as reduced muscle force production during high-velocity movements.
Currently, scientists are examining the premise that, as an individual ages, muscular changes are more likely attributable to decreased motor activity levels and are age related rather than being solely age dependent.69,72 Acknowledging that investigators had previously found that muscle power deteriorates more quickly with age, scientists set out to measure training effects in older adults.61,74 These investigators concluded that with training older adults were capable of improving strength, power, and endurance.
The skeletal system, similar to the muscular system, experiences periods of growth, stability, and degeneration. The immature skeletal system is composed primarily of preosseous cartilage and physes (growth plates).75 More simply, bone in infants and young children is flexible, porous (lower mineral count), and strong with a thick periosteum.75,76 Given these properties of immature bone, a child is less likely to have a fracture because the periosteum is strong and consequently the bones absorb more energy before the break point is reached. In addition, if a fracture does occur, healing is usually quicker because callus is formed faster and in greater amounts in children than in adults.
A primary difference between the child’s and the adult’s skeletal system is the presence of the growth plate complex in children. Whereas primary ossification occurs prenatally, secondary ossification is not complete until the child reaches skeletal maturity, generally at age 14 years in girls and 16 years in boys.76,77
Even after bones have attained their full length, they continue to grow on the surface. This is termed appositional growth and continues throughout most of life. During childhood and adolescence, new bone growth exceeds bone resorption and bone density increases. Until age 30 years, bone density increases in most individuals, and bone growth and reabsorption remain stable through middle adulthood. Later in adulthood, resorption exceeds new bone growth and bone density declines.78
Women exhibit more loss of bone mass than men do.79 Decreased bone density in women is generally attributed to differences in the types and levels of hormones present. Although the difference is most significant during menopause, premenopausal women still lose bone density at a higher rate than their male peers do.
Osteopenia is the presence of a less-than-normal amount of bone and, if not treated, may result in osteoporosis. Progressive loss of bone density, observed into older adulthood, is commonly identified as osteoporosis. Osteoporosis is more common in women than in men and is a major cause of fractures and postural changes in both sexes.80
Overall, much of the growth in the musculoskeletal system is related to demands placed on the system. Intrinsic and extrinsic forces imposed on the musculoskeletal systems of typically and atypically developing children may lead to structural and functional differences in their respective skeletal structures. Consequently, temporal sequencing, acquisition, and characteristics of motor behaviors emerge differently in typically and atypically developing children. Similarly, age-related changes in older adulthood may be accelerated in direct proportion to decreased levels of activity.81 Older adults who maintain more active lifestyles and place greater physical demands on their musculoskeletal systems are more likely to have an improved bone density and muscle mass than their peers who are not as active.82
Sarcopenia, the age-related loss of muscle mass, affects strength, power, and functional independence in older adults.72,82 Although these changes are observed in many older adults, the degree of the muscular changes varies.70 Researchers examining sarcopenia in older adults reported that men are affected more by sarcopenia than women are.72,83 In fact, men with sarcopenia manifest four times the rate of activity limitations than do men with a normal muscle mass. Changes in the cross-sectional area of muscles directly affect the force production of a given muscle; consequently, as the cross-section of a muscle diminishes, its ability to produce force decreases. As an individual ages the number and size of the muscle fibers decrease, resulting in a reduction in strength.80 Although this is true in all muscles, the impact is greater on muscles of the lower extremities than in those of the upper extremities.72
Although strength is critical to musculoskeletal function, flexibility is equally as important. Flexibility incorporates joint motion and the extensibility of the tissues that cross the joint. The degree of flexibility changes across the life span as a direct result of aging and activity level.10 Changes in flexibility are evident throughout life: limited at birth, increasing until the individual approaches adolescence, and then gradually decreasing. Exceptions may be seen in athletes, dancers, and other individuals involved in activities that incorporate flexibility training. Loss of flexibility as a consequence of age may have a negative impact on functional independence in older adults. Flexibility is thought to be directly proportional to the amount, frequency, and variability of motor activities performed. As activity increases, so does flexibility. Conversely, as individuals exhibit decreased levels of motor activity, often associated with age, flexibility decreases.78
By age 70 years, flexibility is thought to have decreased by 25% to 30%.70 Although this was purported to be age dependent, it may be more likely that it is age related.69 Regularly performing exercise directed toward improving strength and flexibility can reverse the effects of inactivity for most individuals, even those older than 90 years of age.69,81
As scientists continue to examine functional changes across different systems as a consequence of age, physical and occupational therapists must educate individuals regarding the importance of embracing a physically active lifestyle and methods to enhance quality of life at each stage in an individual’s life (see Chapter 2). Although all systems contribute to an individual’s health and wellness across the life span, the cardiovascular and pulmonary systems play a key role (see Chapter 30).
Cardiovascular and pulmonary systems
The cardiovascular system is composed of the heart, lungs, and associated vascular complex. It is responsible for pumping blood through the coronary, pulmonary, cerebral, and systemic circulations, with the goal of perfusing all bodily tissues for the delivery of oxygen and vital nutrients and picking up waste products for elimination. The pulmonary system is responsible for oxygen transport, gas exchange, and removal of airborne pollutants that may enter during respiration (see Chapter 30).
The interdependent nature of the cardiovascular and pulmonary systems is evident in the fact that, each minute, all of the body’s blood travels through the lungs before being returned to the left side of the heart for ejection into the systemic circulation.84 Because of this relationship, changes in heart function can dramatically affect lung function, and vice versa. In addition, these two systems are connected as part of a larger closed pressure-volume loop through the peripheral circulatory structures. Likewise, any alteration in the function of the peripheral vessels will affect both the heart and lungs, and vice versa.
The function and homeostasis of the cardiovascular, pulmonary, and peripheral vascular systems are influenced by both internal and external forces.84 Internal mechanisms of control are based on the autonomic nervous system, the relative health of the anatomic structures involved, the growth and development of the structures, and the behavioral and emotional adaptations of a particular individual. All those internal mechanisms are subject to changes with growth and development, aging, and the unique life experiences of an individual. Growth and development primarily affect the physics of the system by altering volumes, lengths, smooth and myocardial muscular tension, and physiological capacitance within the system to support the growing body. Numerous effects of aging have an impact on the adaptability of the system. Behavioral and emotional responses influence both autonomic and volitional cardiovascular and pulmonary reactions to stress. External forces include movement environment and activity level, which alter the gravitational forces on the closed pressure-volume system. An increased activity level causes exercise stress, which requires an altered demand for oxygen and nutrients to the structures providing the work. Finally, emotional stress needs to be considered as an external factor. Behavioral responses to stress can affect functional movement and cause maladaptive coping mechanisms on any or all systems. As with anything, the age, cognitive status, and relative health of an individual will dictate the potential success of these endeavors.
Because oxygen transport and exchange are the primary requirements for sustaining life, efforts toward maximizing the efficiency of the cardiovascular and pulmonary systems represent a fundamental component of therapeutic practice. It is critical that no matter where a patient falls in the life span, strategies for screening, prevention, and rehabilitation of the cardiovascular and pulmonary systems be incorporated into a comprehensive plan to promote optimal mobility and independence.85 It is essential for therapists to keep in mind that all interventions have a direct or indirect impact on these systems and that it is their responsibility to monitor and manage those responses to maintain safety.
A detailed understanding of the anatomy of the heart, lungs, and vessels, as well as the physiology and interrelationship of the organs involved, is essential to the practice of both physical and occupational therapy. Refer to Chapter 30 for additional information. For pediatric therapists, the added knowledge of normal growth and development of these structures is critical.
From weeks 3 to 8 of fetal life, the cardiac structures are formed.63,64,86 All other structures of the cardiovascular system are fully developed and functional shortly after birth. Although the left and right ventricles are of similar size at birth, by 2 months of age the muscle wall of the left ventricle is thicker than that of the right ventricle.87 This is attributable to the fact that the left ventricle is responsible for pumping blood to the whole body, requiring a higher internal pressure and contractile force, whereas the right ventricle is responsible for pumping blood only to the lungs, a relatively low-pressure function in a healthy individual.
It bears mentioning that the heart’s function begets structure. Therefore if function becomes impaired, the structure is likely to adaptively change. For example, if the resistance in the vascular system from the right ventricle to the lungs becomes increased, the right ventricle must pump harder, with a greater volume of blood, to overcome the resistance.88 Over time, this will increase the size of the ventricular walls because the myocardium is muscular tissue that is as equally capable of hypertrophy as skeletal muscle tissue.
Structurally, the heart doubles in size by year 1, and its size increases fourfold by year 5. Many of the changes associated with size are complete by the time the child has reached maturity. Recall that cardiac output (CO) is equal to stroke volume times heart rate. As the size of the heart increases (increasing the volume capacity for each stroke), the heartbeat decreases and the blood pressure increases.89 Heart rate in a newborn infant is generally 120 to 200 beats per minute (bpm), 80 bpm by 6 years of age, and 70 bpm by 10 years of age.87,90 Systolic blood pressure (defined as maximal pressure on the artery during left ventricular contraction or systole) is 40 to 75 mm Hg at birth and increases to 95 mm Hg by 5 years of age.87 Blood pressure continues to rise into adolescence. The capacity to maintain exercise for longer periods and greater intensities increases through early childhood. Although cardiovascular disease is generally associated with adults, children as young as 5 years of age may show signs of or be at risk for cardiovascular disease if they do not engage in regular aerobic activity.87,91
Development of the pulmonary system occurs late in prenatal and early postnatal life.90 As the lungs increase in size, tripling in weight during year 1, the capacity and efficiency increase while the respiratory rate decreases.90 Although the vital capacity of a 5-year-old child is 20% of an adult’s, this is not usually a limiting factor during exercise.89 Overall, aerobic capacity increases during childhood and is slightly higher in boys than in girls. The overall work capacity of children increases most dramatically from 6 through 12 years of age.89 Peak oxygen consumption is achieved early in adulthood and changes in direct relation to activity levels. Lungs of an average adult at rest take in about 250 mL of oxygen every minute and excrete about 200 mL of carbon dioxide.92
As activity decreases in older adulthood, so do the structural and functional capacities of the cardiovascular and pulmonary systems. Many of these changes are a result of decreased elasticity of the tissues, decreased efficiency of the structures, and decreased ability to increase workload. CO decreases approximately 0.7% per year after age 20 years so that by age 75 years the CO is 3.5 L/min, down from 5 L/min at age 20 years.92 Functional changes include a decrease in the overall maximum heart rate from 200+ bpm through young adulthood to 170 bpm by age 65 years.87 Older adults have less elastic vessels, and resistance to the blood volume increases. Consequently, older adults reach peak CO at lower levels than do younger individuals. These cardiovascular changes may be compounded by inactivity, resulting in decreased capacity to perform activities that raise metabolic demands and increase the requirement for oxygen transport.93 The impact of these normal aging responses, however, can be reduced through structured aerobic and anaerobic activities. Conversely, physiological performance of the cardiovascular and pulmonary systems improves in response to growth and development.
Neurological system
The nervous system encompasses the CNS and the peripheral nervous system (PNS). The CNS includes the brain and spinal cord, and it is responsible for all bodily functions. The PNS includes both the autonomic and the somatic nerves and is responsible for transporting impulses to and from the CNS.5 The capacity for humans to produce behaviors far beyond those of other animals is directly related to the complex abilities of the CNS and interneuronal communications.
Over the past two decades, technological advances have enabled neuroscientists to dramatically improve their understanding of the molecular changes in the nervous system over time.94 Development of the CNS is coordinated through intrinsic influences involving the temporal and spatial coordination of synaptic connections with genetic processes, along with extrinsic or environmental factors. Initially, development of the CNS is dependent on precise connections formed between specific types of nerve cells and begins with the recruitment of cells that form the neural plate, which gives rise to the neural tube, and then differentiation of regions of the brain begins.5,95 Changes in the nervous system are predicated on critical periods, or times when different regions of the brain are sensitive to change, and occur across the life span.5,28
Differentiation of cells in the nervous system begins during the embryonic period and continues throughout adulthood.5,94 Development of the nervous system during embryonic life involves the overproduction of glial cells and neurons that, after they are no longer useful, die. Additional developmental changes noted in the nervous system include increased myelination within the brain and an increase in neuronal size.63 Much of the growth may be attributed to these changes in the nervous system and may account for the development of the infant’s brain, which increases to one half the size of the adult brain during the first year of life. Neural development, particularly in the cerebral cortex, documented early in development may emerge out of environmental demands and the need to solve problems (tasks). Consequently, experiences can alter neural networks, and more complex experiences lead to increasing complexity of the neural structures.96 Whereas researchers long supported the premise that decline of the nervous system begins generally after age 30 years, more recent studies indicate that adults, even older adults, can form new neural connections and grow new neurons as an outgrowth of learning and training.94,97 Before the work of Eriksson and colleagues, researchers and clinicians believed that structural changes in older adults, such as decreased numbers of corticospinal fibers, intracortical inhibition, and neuronal degradation in centers in the CNS, particularly the cerebellum and basal ganglia, were inevitable.98 In contrast, findings from a study conducted by Draganski and colleagues99 challenged traditional constructs that the only possible changes in the adult human brain were the result of negative changes caused by aging or pathology. Instead these researchers suggested that a direct relationship existed between learning a novel task, juggling, and structural changes in the gray matter. The authors caution that these structural changes were task specific and limited to the training period. Reexamination of magnetic resonance imaging (MRI) scans, after 3 months of no training, demonstrated that subjects no longer displayed the same structural changes as during juggler training.
Loss of neurons in the centers controlling sensory information, long-term memory, abstract reasoning, and coordination of sensorimotor information negatively affects function. For some individuals this may not have significant implications. For others, CNS changes create serious functional losses. Alterations in the CNS, including altered neural control and decreased efficiency in temporal sequencing of muscle synergies, may play a role in postural instability and impaired sensation. Together these changes can result in falls.68
Although the CNS, similar to other bodily systems, may have the capacity to compensate for some age-related changes, the degree of compensation may be modulated by the complexity of the task and continuation of “practice” over time. Although some investigators have reported that neuromuscular systems in older adults may not be as flexible as systems in younger adults, new studies examining changes in mature and aging systems are still in the early stages. Neuromuscular systems in older adults may not be as capable of rapidly reorganizing muscle synergies to produce variable functional responses.98 The researchers did say that this may be related not solely to the aging neurological system but to other factors including experience, cardiovascular and musculoskeletal fitness, and current level of functional independence. Other scientists suggested an alternative view that repetition of motor activities may stimulate new growth in dendrites located proximal to neurons previously lost.68 The authors were quick to add that, although the pathways or connections may be activated, this may or may not result in improved functional ability. Implicit in performance of many functional activities is cognition. If changes in cognition coexist with changes in other systems, it may be difficult to accurately interpret the underlying causes.
Cognitive system
Cognition may be defined as awareness, perception, reasoning, and judgment.100 Cognitive development involves processes of perception, action, attention, problem solving, memory, and mental imagery. Action, from the perspective of physical or occupational therapy, may be referred to as functional movement(s) and incorporates all the processes described previously to successfully perform a specific task.
Jean Piaget, one of the most recognized scientists in developmental psychology of the twentieth century, was particularly intrigued with how biological systems affect what individuals “know.”100,101 He observed interactions among children of different ages and hypothesized that younger children’s thought processes were different from those of older children as evidenced through the differences in responses between them to the same questions.
Piaget proposed that cognitive development moved in a linear, stagelike progression, each stage of which involves radically different schemes.101 He suggested four stages of cognitive development, identified as sensorimotor state (infancy), preoperational (toddler and early childhood), concrete operational (childhood and early adolescence), and formal operational (adolescence and adulthood).100 He proposed that (1) sensorimotor behaviors stimulate cognitive development and (2) problem solving as a measure of cognition enables infants and young children to identify and modify motor behaviors.
Piaget’s theory of cognitive development focused around how humans adapt within the environment and how these adaptations or behaviors are controlled.101 He postulated that behavioral control is mediated through schemas or plans, generated centrally. These schemas provide a representation of the world in an effort to formulate an action plan. At birth, infants’ earliest schemas are organized around reflexive behaviors that are modified as the infant adapts to the affordances and constraints of the environment.
Piaget suggested that adaptations occur through two processes: assimilation and accommodation.101 He defines assimilation as a process of altering the environment around cognitive structures. An example of assimilation is when an infant, initially breast-fed, is transitioned to bottle feeding. Accommodation refers to changes of the cognitive structures to meet changing demands of the environment. Accommodation may be involved when an infant transitions from nutritive sucking (breast or bottle) to nonnutritive sucking (pacifier).
Rather than postulating that infants are reflexive beings with little or no volitional movements early on, it may be more appropriate to view infants as competent beings with volitional and complex behaviors present at birth.102 Brazelton reported that a newborn infant turns toward the mother’s voice rather than toward an unfamiliar voice. In addition, research conducted by Meltzoff and Moore103 provides evidence supporting the complex nature of infant behavior. They found that infants as young as 2 to 3 weeks of age can imitate facial gestures performed by adults. Their work was supported by subsequent studies performed by independent investigators using different procedures and in different environments.104 These findings, contrary to Piaget’s proposal that infants were not capable of imitative behaviors until 1 year of age, provided scientists with a new perspective on infant behavior.
Contemporary researchers approach developmental theory from a dynamic and nonlinear model.21,95,96,105 Over the past 10 years, advances in technology (e.g., diagnostic imaging, functional magnetic resonance imaging [fMRI], magnetoencephalography [MEG], event-related potentials [ERPs]) have dramatically improved the ability to document change within the developing brain.95 These technological advances coupled with developmental paradigm shifts and computer modeling have led developmentalists to propose new theoretical frameworks to explain cognitive development. One model, called neuroconstructivism, incorporates intrinsic constraints and abilities of the CNS at the most basic cellular level with extrinsic influences involving environmental experiences and interactions.95,96 Fundamental to the neuroconstructivist theory is the principle of context dependence, in which representations emerge in direct response to the structural changes in the cognitive system. Embedded within neuroconstructivism is the concept of the infant as interactive, in contrast to more traditional developmentalists’ perception of the infant as passive. Experiences that individual infants engage in vary through processes involving competition and cooperation. The processes employed during development may result in differing pathways or trajectories of development through which the outcome or behavior is realized. Despite the variability in the individual developmental trajectories, the behavioral outcome is often similar.
Current theories lend support to the concept that the cognitive system integrates multimodal input to process, interpret, store, and retrieve information as a mechanism for information processing and problem solving.100 Changes in cognition, defined as relatively permanent changes in behavior, cannot be measured directly but rather must be inferred from changes observed across multiple systems.
The integrative nature of movement, cognition, and perception is evident in developmental psychology literature.106 Given that these domains are interrelated, one area cannot be examined in isolation of other interrelated systems. Acquisition of motor skills is the primary mechanism for evaluating cognition and perception in prelinguistic children. In addition, as individuals grow older, changes in any system may influence functional movement. Finally, when examining functional movements, therapists must always consider the individual’s cognitive and perceptual abilities.
As higher-level cognitive processing skills become apparent, the child can accurately identify relevant cues, filter irrelevant cues, and process information more efficiently. One such higher-level cognitive processing skill is executive functioning. Adolescence signals a period during which executive functioning begins to mature.107 This period may be characterized as critical in CNS development. During this critical period, production of mature, adult-like decisions requires selective attention and increased integration of information via the prefrontal cortex. During the maturation process, adolescents may exhibit inconsistent decision making, resulting in less-than-optimal outcomes. By young adulthood, as the individual approaches maturity, optimal executive decision making becomes more consistent.
Another example of the multidimensional processes involved in higher-order tasks such as functional movement is found in a study conducted by Hazlett and Woldorff.108 They proposed that implicit in motor tasks are concepts of cognition including attention, perception, and information processes. This multimethodological approach examined (1) the influence of attention on sensory and perceptual processing, (2) the executive control of attention by higher centers of the brain, and (3) the processes underlying multisensory integration and the mechanisms by which attention interacts with such integration processes.108
A new paradigm that embraces the concept that memory and cognition do not deteriorate as part of normal aging is a topic of discussion in scientific literature.109 This perspective was proposed after Gould and colleagues109 conducted a study that found that adult primates continue to develop new brain cells throughout life. The addition of new neocortical neurons throughout adulthood provides a continuum of neurons of different ages that may form a basis for marking the temporal dimension of memory. These late-generated neurons play an important role in learning and memory of older adults.
Changes in cognitive function are often revealed during tasks that require processing and retrieval of cognitive or motor memory. Consequences of aging include slowed information processing and increased time necessary to perform motor skills. Even though learning may take more time in older adults, once a behavior is learned, retention is similar to that of younger individuals. Of significance for older adults is delayed performance of long-standing tasks such as driving a car, which may have serious consequences for the driver, passengers, or others in the immediate vicinity of the vehicle. Delays in processing and task execution pose risks to the older adult or individuals with CNS deficits and may affect the individual’s level of independence and quality of life.110
Memory
Memory can be broken down to three types: working, declarative, and procedural. Working memory, short-term memory, is the equivalent of the RAM of a computer.100 This is the mechanism that enables a child who does not appear to be attending to what the parent is saying to repeat what the parent has just said. Given the temporary nature of this memory, no space in the hippocampus or amygdala is required. Working memory may in fact be more of a cortical phenomenon. Declarative memory is what is typically envisioned when we think of intermediate or long-term memory. Declarative memory is the area where long-term information about everything an individual has ever learned or information acquired is stored, including facts, figures, and names.100 An example of declarative memory is a second-grade teacher recalling the name of a student she had in her class 15 years previously. Declarative memory is analogous to the hard drive in the computer. The third type of memory is procedural memory. Procedural memory involves all motor activities, actions, habits, or skills that are learned through repetition in motor practice.100 Examples of procedural memory include walking, playing an instrument, and driving a car.
Rovee-Collier and colleagues111–113 have conducted numerous studies related to memory retention in prelinguistic children. Evidence exists to support the premise that infants as young as 2 to 3 months of age are capable of identifying relevant cues and chunking this information for later retrieval. One caveat is that retrieval of such information is possible only when the specifics of the behavior are retained. Infant memories are tightly linked to the specific information related to the task, environment, and stimulus. Consequently, a slight change in any of these three components may result in an inability to retrieve information from infant memory. Retention of information is directly proportional to the infant’s age. As an infant grows older, the period for which information is retained increases.
Across the life span, some aspects of cognition seem to be impaired or changed before others. One area most susceptible to age-associated changes is the prefrontal cortex. This particular area of the brain is where information critical to executive function, attention, and working memory is stored.114 Although memory is one component of cognition that is generally acknowledged to deteriorate as an individual moves toward older adulthood, not all aspects of memory are affected at the same time or in the same way.
Episodic memory is reportedly the first to be impaired, then working memory (short-term memory).114 Implicit memory and semantic memory remain intact for a much longer period of time. Little information is available about procedural memory, memory of how to perform tasks. Researchers have suggested that an older adult’s declarative memory is also affected by normal and neuropathological aging.42,114 These investigators suggested that although older adults with deterioration in declarative memory are able to perform tasks, the individual is unable to retain information and consequently unable to learn tasks.42 Many factors negatively or positively influence memory, including the nature of encoding or processing that information, such as the source of the material or time of day material is presented.114
Although evidence exists that many aspects of memory decline with age, recent evidence supports the premise that variables other than encoding and retrieving information may have a significant impact on memory and remembering in older adults.115,116 Researchers at the University of Kuopio examined memory in older persons and focused on neuropsychological processes as a method for evaluating memory and other functions of the frontal lobe.116 The investigators reported that elderly subjects with subsequent degradation of the frontal lobe had memory loss. These researchers suggested that some aspects of memory loss could be staved off through memory-sharpening activities and games, limitation of alcohol consumption, and participation in activities designed to retain details of skills and tasks. Similar to these findings are the conclusions of May and colleagues,115 who examined the role of emotion in memory tasks for older adults. They reported that older adults seem to be motivated to remember information that is emotionally relevant and meaningful. These findings lend support to yet another system, the emotive system, which could add vital information to an older adult’s memory and task performance.
Emotional system
Although current literature does examine the emotional development of children,117–125 the normal emotional development of adults over a life span remains a mystery. Zinck and Newen126 proposed a classification of emotion that might provide a clearer understanding of responses within and between individuals and factors that affect emotion. The authors characterized emotion into four categories based on when the emotions appear developmentally. Emotion is characterized as a means of communicating state, expectations, and reactions of an individual.126 Emotions are “interpersonal/interactive” behaviors that enable the individual to communicate to the world. The four categories are pre-emotions, basic emotions, primary cognitive emotions, and secondary cognitive emotions. Pre-emotions and basic emotions function as basic mental representations, whereas primary cognitive and secondary cognitive emotions are categorized as cognitive attitudes.
Pre-emotions are characterized as innate behaviors, present at birth, nonspecific, nonintentional, and used for communication to others about the state of the infant.126 Pre-emotions are identified as comfort and distress. These responses may be positive or negative responses depending on the situations. Pre-emotions are the most fundamental sensations followed by basic emotions.
Basic emotions and developmental timing of basic emotions include joy at 2 to 3 months, anger at 3 to 4 months, sadness at 3 to 7 months, and fear at 7 to 9 months. These emotions are said to emerge in the absence of conscious processing of stimuli. These responses are shared by other mammals, and do not involve complex cognitive processing. These behaviors lead to faster and more stereotypic responses.126
Typically, emotional “development” emerges in childhood. Examination of emotion in adults often involves a retrospective analysis of the behavior over a specified period of time. Although the focus of the research may be directed toward emotion, memory cannot be disentangled from the emotion. With regard to aging in older adults, researchers generally have reported that emotions—in particular, negative emotions—diminish later in life. Some researchers have suggested that diminished negative emotions may be attributed to decreased functioning in the amygdala.127 Still other investigators have suggested that, rather, a decline in the functioning of the amygdala and decreased ability to recall negative experiences may be attributed to the socioemotional selectivity theory (SST).128 The SST involves prioritization of memories and which temporal boundaries play a role in prioritization. Specifically, older adults do not perceive negative emotions as a priority; hence older adults are more likely to process positive emotions than negative.
A literature search of “normal emotional development across the life span” was limited in scope and volume.129 Problems in normal emotional development can be identified throughout medical literature, but again the emphasis is on children and adulthood emotional problems stemming from either pathological conditions or environmental conditions during childhood.130–135 Within the literature, the reader can find discussions of emotional intelligence in adults and how emotional skills such as empathy or cultural sensitivity might be taught.136–142 Specific aspects of an emotion or mood change and how that might assist or hinder an individual within a psychosocial environment can be located,143–146 but the integration of the entire emotional system and its normal changes throughout life still eludes researchers. Future research directed toward aging and emotion has potential to broaden the theoretical perspective by examining emotional experiences in an ecological context.147 In addition, identifying, measuring, and analyzing variables that appear to make a difference in social and professional success will be future scholars’ dissertation studies.148 (See Chapter 5 on the limbic system and its influence on motor control and Chapter 9 on psychosocial adaptation and adjustment for additional information.)
Language
Consistent with all areas of development, acquisition of language, receptive and expressive, is measured quantitatively and qualitatively. Critical to the acquisition of receptive and expressive language is sensory, cognitive, perceptual, and motor development in the infant and child. Researchers have found evidence that language development emerges through nonverbal gestures or “signs”149–153 and is evident as early as 6 months of age.152,153 As the number of nonverbal gestures increases, verbal communication reportedly emerges earlier than in infants who do not use nonverbal gestures.150,152,153 “Gesture thus serves as a signal that a child will soon be ready to begin producing multi-word sentences.”154 Having a large number of gestures at 18 months of age positively affects later language development and is the foundation for later linguistic abilities.151
Imitation, such as “mama” or “dada,” is often the first form of verbal communication, progressing to spontaneous single-word utterances. Infants produce their first spoken single-word utterances as early as 12 to 15 months of age.155 During this time the child’s brain is undergoing rapid differentiation in Broca’s area; at the same time, motoric ability to communicate verbally is emerging. Consequently it is evident that intrinsic (neurodevelopmental) constraints and extrinsic (environmental) factors affect the emergence of receptive and expressive language. Investigators examining utterances in children and adults reported that utterances produced by children do not approximate those of adults until 14 years of age.156,157 Recently researchers reported that, consistent with findings of earlier investigators, articulatory movement speed increases from birth to adulthood.157 Throughout childhood, as language acquisition emerges, children become more sophisticated in communicating and more fully integrate information from intrinsic and extrinsic sources to produce more complex utterances.155
Maner and colleagues156 reported that children exhibited increased variability when a five-word sentence was embedded in longer sentences than when the child spoke only the five-word sentence. These findings led the investigators to infer that a relationship existed between language processing and movement in young children.158 In addition, adults reportedly modified the five-word sentence when it was embedded in the longer sentence, but 5-year-olds did not modify the utterance. Sadagopan and Smith159 replicated the work of Maner and colleagues156 and found that children aged 5 to 16 years exhibited more variability when the five-word sentence was embedded in a more complex sentence compared with when the five-word sentence was spoken in isolation. Young adults (21 to 22 years old) reportedly did not exhibit this same variability. In addition, investigators reported that the duration of the simple and complex utterances differed between children and adults. Unlike the youngest children (5 and 7 years), duration of the utterances decreased in adults. This finding provided evidence for the investigators’ theory that adults altered or shortened the complex utterances, given the shorter duration taken to utter the complex sentence. Whereas earlier researchers reported that both adults and children decrease their rate of speech during complex sentences,160 more recently investigators suggested that adults may increase their rate of speech production. Sadagopan and Smith159 reported that although both children and adults slow the rate of speech production, children exhibited a much slower rate than adults in producing complex sentences. Hence investigators concluded that whereas adults’ rate of speech production did explain some of the difference in utterance duration for the simple and complex sentences, it did not fully explain the differences. This led investigators to suggest that differences in utterance duration may be attributed to both faster rate of speech and altered or shortened complex sentences containing the simple five-word phrase.
Perceptual system
As researchers continue to examine the interactive and interdependent roles of body systems, the perceptual system must not be omitted. Perception, yet another process important to performance of functional movements, involves acquisition, interpretation, selection, and organization of sensory information. Perception is the very essence of the interaction between organism and environment. Every movement gives rise to perceptual information and in turn guides the organism to adapt movements accordingly.10,161
Initially perception revolves around the infant’s visual exploration of people, objects, and environmental activities. Infants are capable, at birth, of visually exploring their environment, people, and objects.101 Investigators have suggested that infants use information acquired through visual exploration to develop new methods of exploring and discovering cues about the environment such as depth, distance, surface definition, and dimensionality of objects.162
A second phase of perceptual exploration emerges as an infant’s exploratory behaviors transition to functional movements such as reaching and kicking. Through these exploratory behaviors emerge additional mechanisms for acquiring information about the environment.6,161 Throughout development, active exploration enhances perceptual information through each new encounter and enables the infant to recognize distinctive features and similar characteristics that allow the infant to differentiate between objects. The information generated from exploration provides new input to many subsystems, in particular the sensory, motor, and cognitive systems that enable the individual to gain new knowledge about the environment and the action.
If perception is the process of integrating and organizing intrinsic and extrinsic input, then changes in sensory systems as a consequence of aging are certain to affect perception.163 The visual perceptual processing system is most often identified as altered in older adults. Specifically, researchers have reported that although older adults are capable of discriminating between variation in depth perception in a manner similar to that of younger adults, they are less able to discriminate between three-dimensional shapes of objects.164 Clearly the perceptual system is closely associated with many other body systems, and therefore age-related or age-associated structural and functional changes in associated systems will affect the perceptual system.
In addition, May and colleagues115 found that older adults placed less emphasis on perceptual aspects of an event than they did on the emotional components when encoding information. They suggested that older adults may find emotional information to be more meaningful than perceptual information and may retain more elaborate, detailed processing of emotional data than perceptual information.
Although there is no conclusive evidence regarding age-related changes in perception, evidence may be emerging that supports age-associated or individual differences.165 Nonetheless, the role of perception in aging should continue to be investigated and should not be underestimated or minimized until such time as adequate evidence exists.
Motor development
Movement is the primary mechanism by which prelinguistic children communicate with their environment. That said, it is no wonder that development of motor skills is greatest during the first 2 years of life. Motor development may be defined as the acquisition, refinement, and integration of biomechanical principles of movement in an effort to achieve a motor behavior that is proficient.11
Early developmental researchers referred to infants as reactive, inferring that, early on, infants are responsive to stimuli rather than capable of initiating functional movements. Young infants were characterized as “reflexive” beings producing stereotypic primitive and postural responses to stimuli. Emergence of these reflexive motor behaviors was based on traditional models of CNS organization and motor development theories. Traditional theories of human development emerged from animal models and studies involving spontaneously aborted fetuses.14,166 Traditionally, sucking and stepping behaviors were examples of developmental reflexes. By definition, a reflex is a consistent response to a consistent stimulus. By use of traditional models of CNS organization, developmental reflexes, present at birth, become integrated as higher centers assume control over lower centers and then volitional movements begin to emerge.
Over the past two to three decades, advances in technology have enabled scientists to gain more insight into fetal and infant motor abilities. More recently, research has generated evidence that behaviors emerge out of a need to solve a problem in the environment rather than solely as a result of maturation in the CNS.167 Given this evidence supporting the premise that newborn infants are capable of producing complex volitional movements, previous views of the infant as passive and “reflexive” are no longer accurate. In addition, continuing to refer to early infant motor behaviors as “reflexes” may also not accurately reflect the behavior. A reflex is defined as a consistent response given in response to a consistent stimulus. Perhaps use of the term innate motor behaviors to reflect behaviors that are present at birth may be more appropriate. See Figure 3-1, A to C, for a visual explanation of how the complexity of the stepping reaction of a newborn infant and the learned programming for upright posture and balance, including biomechanical range and force production, will lead to the integration of stepping in standing. Similarly, as an individual ages, loss of some of the postural power, effectiveness of balance reactions, and fear can create a potentially dangerous environment for an elderly person (Figure 3-1, D to E). Likewise, an individual with an abnormal or inefficient stepping pattern (Figure 3-1, F) should automatically stand out to a therapist analyzing movement dysfunction. If a clinician does not have a clear picture in his or her mind of the movement pattern desired, then easily or quickly identifying the system or subsystem motor impairments seen in a client’s movement dysfunction may be outside a therapist’s analytical repertoire.
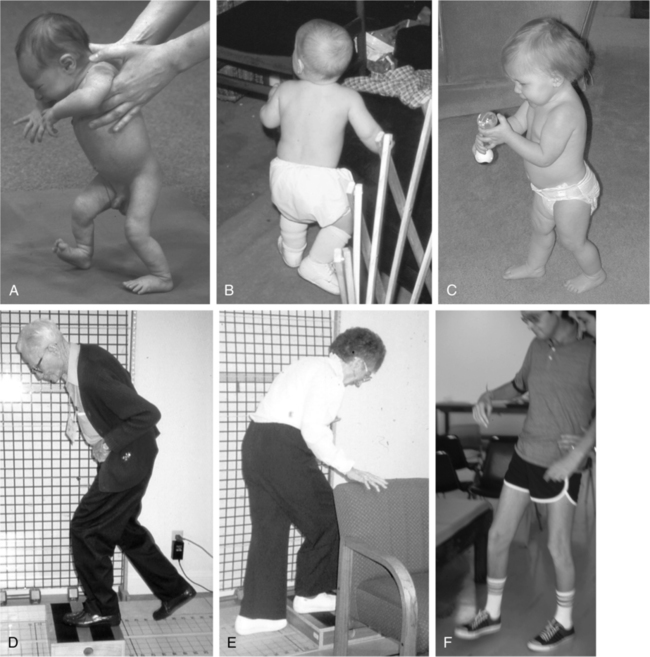

Contemporary research refutes the assertion that infants are reactive organisms.95,96 In contrast, contemporary studies purport that infants are competent and capable of producing complex interactive behaviors at birth.101,168 Additional support for the complex nature of a newborn infant is evident in the infant’s ability to discriminate and turn toward his or her mother’s voice rather than toward the voice of an adult with whom the infant is unfamiliar.
Evidence from studies examining motor development indicate that motor behaviors do not always emerge in a linear and predictable sequence, nor do all individuals achieve the same skills at the same chronological age.8,168 Rather, emergence of motor behaviors in an alternate sequence may be attributed to the intrinsic and extrinsic constraints that contribute to motor development in a nonlinear fashion and is not necessarily indicative of atypical development. Figure 3-2, A is an example of a child who had a very large head at birth. His head circumference was in the 99.9th percentile and remained so for the first 3 years of his life. His Apgar score at birth was 10, or normal. He was slow in rolling over and coming to sit and spent much of his time playing with his hands and feet and visually exploring the environment. Figure 3-2, B and C illustrate that his focus was on fine motor development throughout his first year, especially when he was placed in a vertical position. He loved to play catch when placed in a sitting position and accurately trajected the ball toward a partner when playing by age 1 year. His early gross motor development was within the normal range but below the mean. He started independently walking at age 14 months and began running on the same day. Figure 3-2, D through F illustrate that once he gained control over the heavy weight of his head, he quickly caught up in gross motor skill. And, like any child, he has taken full advantage of his environment to play and learn.


Motor performance, measured both qualitatively and quantitatively, is highly dependent on the task, the environment, and the individual. Changes in motor performance emerge in accordance with age-dependent changes, within different systems, and with respect to environmental affordances and constraints. As skills emerge in speech, language, and cognition, other previously achieved skills may “regress.” In reality, acquisition of a new skill requires more attention than the previously attained skills; consequently, the infant or child’s attention is divided between the tasks. Lindenberger and colleagues169–171 conducted studies investigating life span changes in resource allocation during multitask activities. The researchers found that for young children certain tasks require more attention, and attempting to perform such a task in conjunction with a task requiring less attention causes deterioration in performance of both tasks. Hence, deterioration of a previously attained skill is more likely a result of attentional demands of young children performing high-attention tasks rather than a true “regression” of the skill (see Chapter 1, Figure 1-9, p. 18). This progression is illustrated by a child confronted with a new environment, who will seem as if he or she has regressed in motor performance while confronting and solving a task-specific challenge—for example, crossing over a suspension bridge that moves from side to side, is compliant to body weight, and creates a perceptual challenge from the visual surround. Once the child understands the task, his attention is directed toward developing effective strategies to solve a problem and successfully perform the motor behavior of crossing the bridge. Stability or consistency in performing a skilled movement is achieved by self-organization through practice and repetition.21 Performance of skilled movements, such as those observed in athletes, is measured not only on the consistency in performing the task but also on the skilled performance of the task under variable conditions.21 Conversely, decreased frequency in performing a motor skill as an effect of age may result in a less rich repertoire of normal variability and may be a contributing factor to a decline in motor skills.30 Just as motor skills emerge from a multifactorial interweaving of maturation and experience, deterioration in motor performance may be attributable to alterations in various systems that occur as part of the aging process. Emergence of motor behaviors is never the same for any two individuals, nor does decline in functional motor behaviors follow the same time line. Figure 3-3 illustrates how standing patterns will change with practice, be maintained as long as practice continues, become extremely efficient within a specific environmental context, or become deficient after CNS injury.
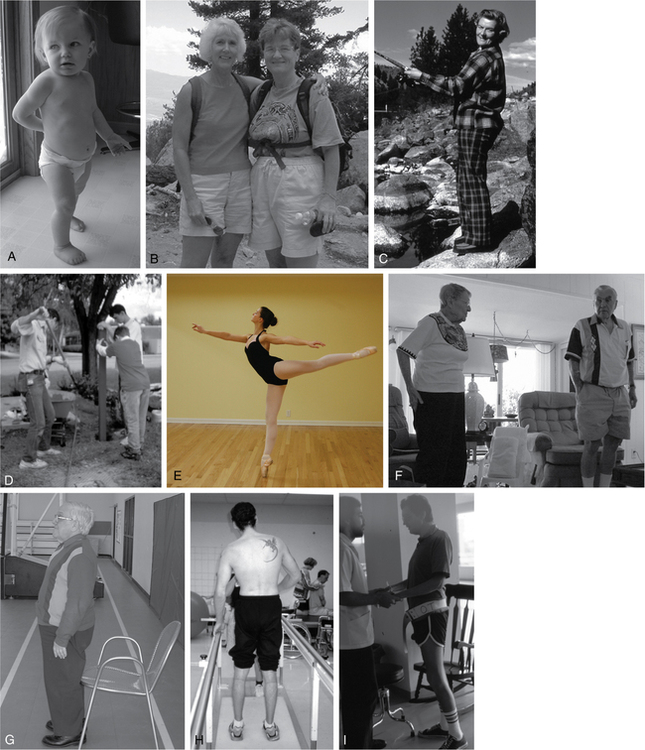

Prenatal (0 to 40 weeks’ gestation) development
Motor behaviors emerge early in embryonic life. By the tenth week of fetal life the variety of observed movements increases, as does the frequency of the movements. Complex movements are present by gestational age (GA) 12 weeks, and goal-directed movements may be seen as early as GA 13 weeks. Facial movements, including sucking, swallowing, and yawning, are evident in the second and third trimesters. The fetal activity level increases so that by week 14 GA, periods of quiet (no activity) are only 5 to 6 minutes in duration. Investigators have documented 15 fetal movements visible by 15 weeks of age.172 After initial observation of a motor behavior, it remains part of the fetal repertoire. Pooh and Ogura’s172 research lends support to the premise that before delivery fetuses are in fact capable of producing complex motor behaviors.
The dynamic nature of birth and the associated change from the intrauterine to the extrauterine environment alter the production of movements previously observed in fetal life.65 As the newborn infant adapts to the forces in the extrauterine environment, motor behaviors emerge. These complex behaviors lend additional evidence to the premise that at birth infants are competent beings.
Infancy (birth to 12 months)
As alluded to earlier, newborn infants possess a rich array of motor behaviors. During the first year of life, motor behaviors are the primary mechanism for learning. Every movement is a new and unique opportunity to gain knowledge about the environment. During each movement, new information is gathered in an effort to solve environmental problems, and as a result this motor planning fosters cognitive development. Similarly, each movement provides feedback that intrinsically enables the infant to modify movements in accordance with changes in the environment, the skill, or growth parameters.173 This interdependence between perception and motor behaviors allows one domain to facilitate acquisition of skills in the other domain in a reciprocal fashion.
Given the capabilities of a newborn infant, many behaviors previously identified as reflexes are in fact functional motor behaviors that the infant is capable of modifying. Evidence that one such behavior, sucking, is not a reflex was supported by studies examining sucking rates when stimuli were varied.174,175 Researchers reported that the sucking response varied depending on the level of hunger or environmental stimuli. In addition, when the stimulus is introduced after feeding, after the infant is satiated, the stimulus may produce no response or a diminished response, thus refuting the idea that sucking is reflexive.
Additional evidence exists to refute the concept that other motor behaviors are reflexes. Stepping is one such behavior. Thelan and Fisher18,32,33 conducted a series of experiments examining the stepping reflex in young infants. Early developmentalists hypothesized that stepping reflexes, present at birth, became integrated and then later emerged as a volitionally controlled movement. Thelan and Fisher18,33 found that when one variable, weight, was altered, infants mimicked “integration” or emergence of the behavior. Young infants who were stepping had weights added to their lower extremities, to simulate weight gain over the first few months. These infants stopped stepping. Similarly, infants who did not step were submersed in chest deep water, simulating less weight in the lower extremities, and stepping appeared. Obviously, the presence and absence of this behavior was mediated by weight gain in the lower extremities and not by CNS control as early developmental researchers had postulated. Consequently, upright mobility emerges when the infant is able to garner the force production in the lower extremities to modulate stepping. This is just one example of the significance of one system on another and the interdependent nature of body systems. Recognizing the interdependence of systems may provide one explanation for the presence or absence of motor behaviors at any given time. These concepts have been transferred into the therapeutic practice environment when working with individuals who cannot generate enough force to produce the movement given the body size or cannot produce the postural stability to reinforce the stepping pattern or one of a variety of other motor components that support normal upright stepping or walking. (See Chapter 4 for theories of motor control and learning, Chapter 8 for therapeutic approaches to assist a client with learning or relearning motor control, and Chapter 37, which introduces emerging practices to bridge the gap between normal human movement development and technologies.)
At birth, an infant is capable of turning toward the sound of her or his mother’s voice and visually focusing on objects 8 to 12 inches from the face.101 These behaviors are apparent when the infant’s head is supported, given that at birth the newborn infant does not have the neck strength to maintain head control against gravity. Similarly, auditory and visual stimuli continue to bombard the infant and challenge the motor system, fostering the need to attain head control.
By age 3 to 4 months, as the infant is able to maintain head control in the upright position for longer periods, coordinated eye-hand activities begin to emerge. Acquisition of manipulative skills involves perception and lends support for the coupling of developing cognitive, sensory, and motor systems.23,161 Bushnell and Boudreau6 added that if the infant is unable to achieve a motor skill and this skill is coupled with a sensory or cognitive task, that task may not be attained. Bushnell and Boudreau’s6 research focused on the role of motor development in achieving skills in other domains.
Reaching is one such task that the researchers suggest may serve to promote skills in cognitive and sensory domains. Initial reaching activities enable the infant to gain information relevant to depth perception, and coupling this information then allows the infant to modulate parameters associated with reaching. For example, the infant must learn to vary the distance moved and force necessary to attain an object given a series of opportunities. Infant grasping and reaching may initially seem inefficient, but with practice under varying situations efficiency and accuracy improve across multiple domains with varying rates. Figure 3-4 illustrates both the error that provides feedback and the success during complex movement patterns after practice.
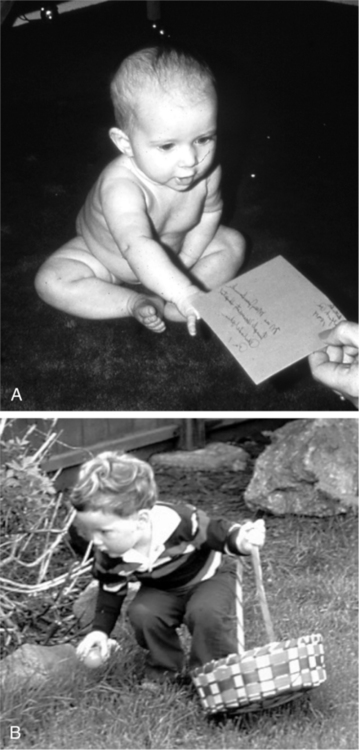

As infants develop an upright sitting posture, they use their upper extremities for support. Sitting, a functional motor behavior, is tightly linked to the performance of most ADLs and occupational and leisure-time activities. Figure 3-5 depicts development of functional sitting over a lifetime. A delay in attaining independent sitting may directly affect upper extremity control, alter attainment of skills in other domains, and ultimately affect an individual’s level of functional independence.
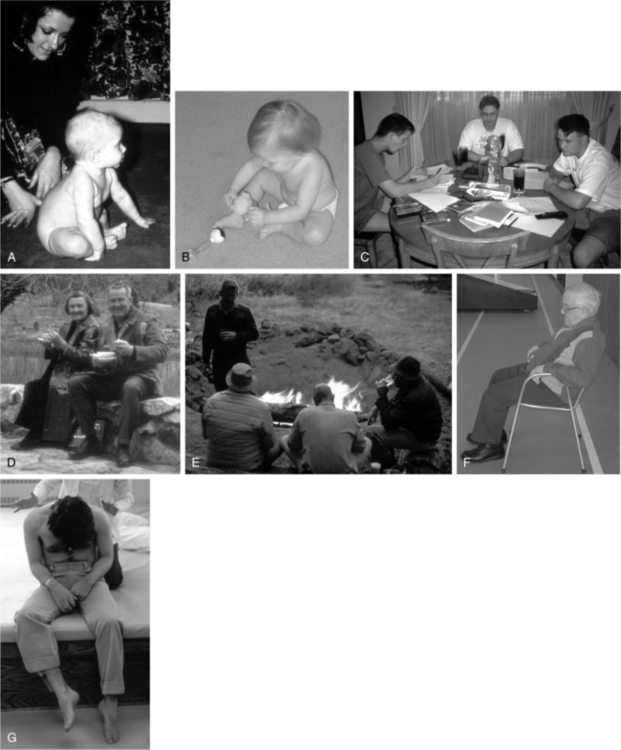

As upright trunk posture is attained and independent sitting emerges, usually by 6 months of age, and infants then begin to explore using their manipulative skills. Manipulative skills are composed of reaching and grasping behaviors. Upper-extremity interlimb coordination bimanual and unimanual tasks include retrieving objects (placed within reach); holding two objects, one in each hand; using two hands to hold an object (bottle); and holding a toy in one hand while retrieving another object with the free hand.176
During the second half of year 1, the infant is focused on mobility, initially prone (rolling, crawling), then creeping on all fours, and then upright (cruising and ambulation). Adolph and Berger23 reported that as coordination of upper- and lower-extremity movements with trunk control emerges and infants begin upright mobility, they spend up to 50% of their day performing balance- and mobility-based activities, varying the surface, distance, and other parameters each time the task is performed (Figure 3-6). On the basis of research conducted with infants acquiring independent mobility, Adolph and Berger23 estimate that an infant walks up to 29 football fields each day.
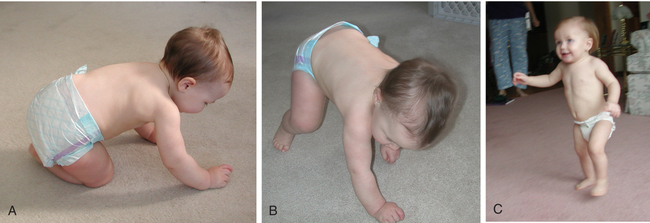

Acquisition of independent mobility is complicated by new manipulative skills, as discussed by Corbetta and Thelan.176 They found that while infants are achieving independent mobility, their manipulative skills are highly variable and vacillate between bimanual and unimanual tasks depending on the nature of other tasks with which the infant is involved. Infants may revert to performing bimanual activities, with upper extremities coupled and movements synchronized, during early acquisition of independent mobility, signaling the presence of multiple tasks requiring attention. Unimanual control signals uncoupling of the upper extremities and asynchronous manipulation in young children.
Analyzing the early development of a child is often done at specific times over the first year, such as at birth, 2 months, 6 months, and 9 months. As important as understanding and analyzing a complex phase of development such as 3 months is analyzing the changes in motor control and learning of a specific motor function over a period of time. The development of head control is a good example of how the nervous system adapts and learns given different environmental restraints over a period of time. The complexity and integration of movement patterns involved in a child gaining functional control over the head in all spatial environments can be delineated into many components. Each component can then become a variable in determining how and if a child has or will develop a specific movement pattern such as head control (see Figure 3-2).
Early childhood (1 year to 5 years)
Whereas the first year of life is characterized by periods of rapid physical growth and acquisition of motor skills, the second year signals a slower rate of growth, refinement of current skills, and acquisition of new motor skills.177 Concurrently the toddler experiences rapid differentiation in other domains including cognition, speech, and social-emotional domains.
At the onset of the second year of life, independent ambulation becomes refined as other forms of mobility wane. Dynamic balance in an upright bipedal posture evolves as the infant develops more mature gait characteristics. Modification of parameters indicative of a more mature gait include narrowing of the base of support, decreased co-contraction in the lower extremities, and improved intralimb coordination, as well as learning to modulate displacement and velocity.23 As gait matures and toddlers have more opportunity to explore their environment, more challenges appear. Attempts to solve these problems and challenges result in the appearance of more complex motor behaviors that include running, climbing, and jumping. Toddlers find particular pleasure in throwing, kicking, and catching balls. In addition, toddlers assert their independence through such activities as propelling themselves with riding toys.
Toddlers continue to explore and assert independence through activities involving bimanual and unimanual tasks. Challenges to fine motor skills of toddlers involve manipulating functional objects (large buttons, eating utensils, crayons, door knobs, and blocks; opening and closing jars to retrieve small objects [cereal, raisins]). Achieving these tasks enables the toddler to perform rudimentary aspects of ADLs such as eating and dressing and adds another degree of independence. Figure 3-7 illustrates development of ambulatory skill over a lifetime.
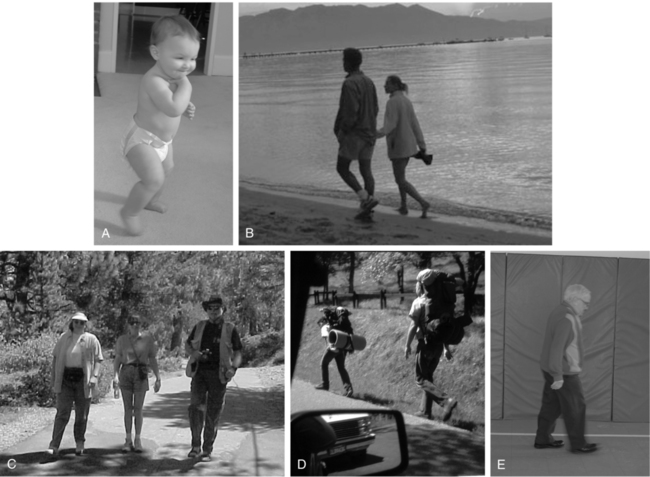

Preschool-age children pedal a tricycle and use a narrow base of support to walk along a balance beam. By age 3 years most children ascend stairs using alternating feet and by 4 years most descend stairs alternately. Figure 3-8 shows a preschooler descending stairs. The gait pattern matures with reciprocal arm swing and a heel-to-toe gait pattern. Early in the preschool period, children mimic a “true” run and have difficulty efficiently controlling all aspects of the behavior. Finally, receipt and propulsion of balls of all shapes and sizes improve qualitatively.
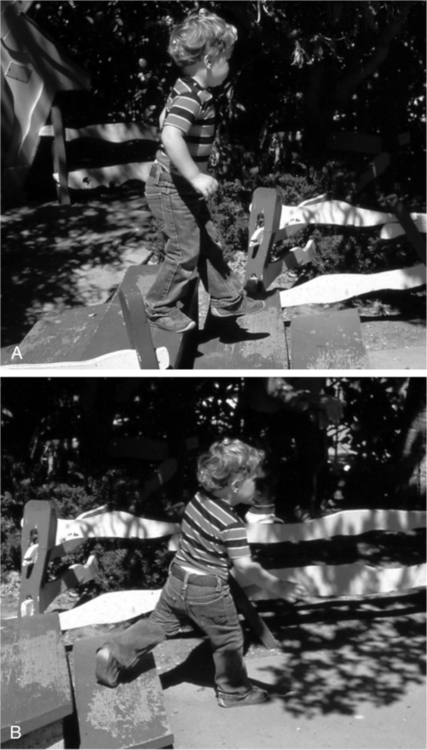

Childhood (5 to 10 years)
Motor skills that children display during this period include galloping, hopping on one foot for up to 10 hops (hopscotch), jumping rope, kicking a ball with improved control (soccer), and bouncing a large ball (basketball). Often these skills emerge while playing with peers during directed (physical education or community-based team sports) and nondirected (recess) periods. Mobility, balance, and fine motor skills improve dramatically. Girls and boys exhibit similar abilities in speed up to age 7 years but by age 8 years boys begin to outperform girls.177
During childhood, manipulative skills increase exponentially. Figure 3-9, A through E, shows the amazing skill developed between birth and age 4 years. Manipulative skills assume a predominant role as part of the academic experience, requiring high levels of practice and opportunities for refinement of the skills. Hand preference is confirmed by this age. As components of independence, many of the manipulative skills achieved are directly related to self-care activities. Skills that improve dramatically include dressing, including fastening and unfastening clothing; tying shoes; using an implement for writing (coloring and handwriting); and successfully manipulating utensils not only to eat, but to socially interact while eating. As children approach preadolescence (9 to 12 years of age), manipulative skills improve dramatically. Children produce cursive handwriting and complex drawings.
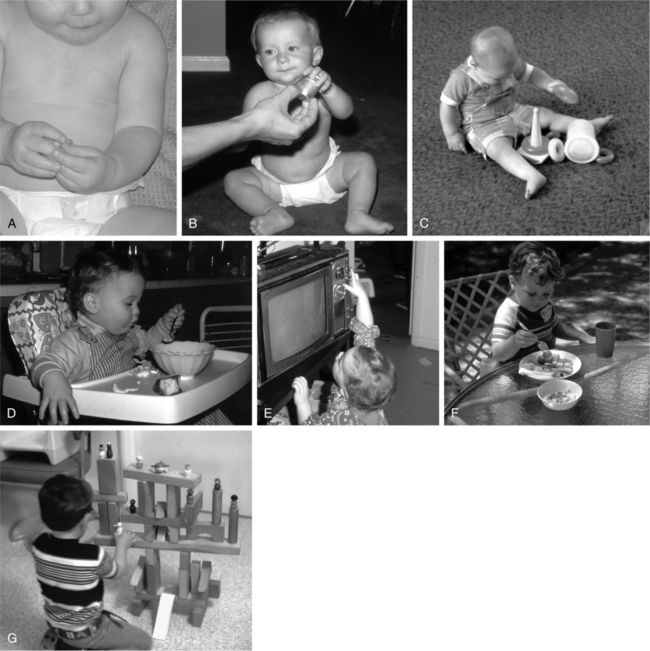

Perceptual development often improves significantly, often in direct relationship to the demands of the tasks along with practice, feedback, and motivation.177 Visual-perceptual systems are nearing maturity and allow children to participate in sophisticated activities such as archery, baseball, dance, and swimming. Figure 3-10 helps bring to light complex skill development during a lifetime. That skill development may begin with a fun team sport activity and lead to a lifetime of professional accomplishment.
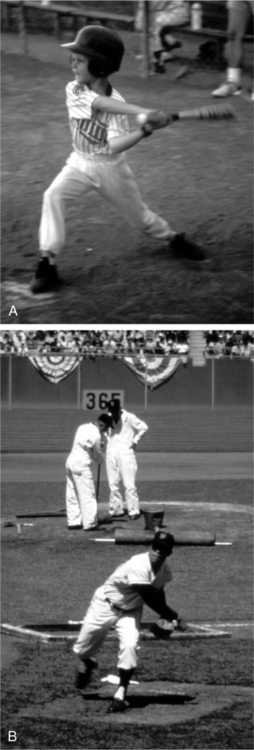

The musculoskeletal system enters a period when muscle growth is rapidly increased, accounting for a large percentage of the weight gained during this period.177 Constraints and affordances of the musculoskeletal system along with demands of the tasks and environment are highly interactive and influential in skilled activities. Children are generally flexible because muscle and ligamentous structures are not firmly attached to bones. Although this allows for flexibility, it also poses risks for musculoskeletal injury. Care should be taken when participation in high-level athletic activities is a consideration.
Qualitative changes in coordination, balance, speed, and strength improve while existing motor skills become more refined and controlled, more efficient, and more complex.177 Qualitative improvements of motor skills may be attributed to an asynchronous growth in children’s limbs in relation to the trunk. Consequently, better leverage is attained. Motor skills strongly influence social domains as boys and girls begin to perform in organized sports teams in school and the community. Competition within sports becomes a powerful force in motivating children to practice motor skills or directing children away from organized sports. Children with poorly developed motor skills, as a result of either genetics or opportunity, may be excluded from team activities and experience social isolation.177 Similarly, a child may have the genetic potential to become a master in an area that uses a specific motor task, but if he or she is never introduced to the specific environment, such as playing a piano, and the motor skill is never actualized.
Adolescence (11 to 19 years)
Early adolescence signifies a period characterized by improved quantitative performance and qualitative changes in skills along with physical growth (size and strength).11 By age 12 years, reaction times closely resemble those of the mature adult. Although skills involving balance, coordination, and eye-hand coordination also continue to improve with respect to perceptual development and information processing, the rate is not as dramatic. Elite athletes, in contrast, often continue to show steady improvement in qualitative and quantitative skill performance well into adulthood.
During later adolescence, when periods of physical growth have stabilized, motor skills acquired previously continue to develop in speed, distance, accuracy, and power. Many adolescents are involved in competitive sports. However, few exhibit performance levels identified with elite athletes. Those athletes that do reach this high level of skill often have a genetic predisposition, environmental affordances, adequate opportunities for high-level practice and performance, and strong motivation. More often, adolescents performing in competitive sports will find this is their avocation rather than their vocation (see Figure 3-10).
Adulthood (20 to 39 years)
Motor performance is relatively consistent in adulthood. Skillful performance of movements may be characterized not only through consistency, but also through the infinite ways in which the skill is performed. Hence, change is generally focused on leisure activities or elite athletic competition. Leisure activities of many adults involve exercise of some form. Maintaining a healthy lifestyle through exercise and fitness is one method for staving off effects of aging and degenerative diseases. Although many adults participate in exercise for health and wellness (refer to Chapter 2 for additional information), others who do not routinely exercise are at risk for obesity and associated health problems. Often some of the physical activity expressed through the motor system is an example of parent-child bonds and creates a fun environment for play. When a task-specific activity is selected and challenged by family members, the motivation to perform becomes high. In Figure 3-11, A, the observer might think that all three individuals are performing similarly with similar strategies. In reality, single-leg stance increases in difficulty as the base of support decreases and the body size changes. Note that the smallest individual has the smallest foot and the largest base of support in proportion to his body size. The adolescent is not as tall as his father, but his foot size is significantly larger, which (1) increases his base of support, (2) gives him less input proportional to his foot size or representation on the somatosensory cortex, and (3) gives him higher degrees of freedom when shifting his weight, which can either increase or decrease the task difficulty depending on practice. Figure 3-11, B shows the way both taller individuals use strategies to initially assume the upright stance position while the smaller child attained the single leg stance by stepping from a table. Body height, weight, and amount of practice all are variables that will help determine outcome. All three individuals achieve success, although the specific motor patterns and strategies used to succeed may be different. In Figure 3-11, C, a child with severe sensory organization problems would not be able to solve the challenge presented in Figure 3-11, A, because he cannot even begin to stand independently on a large, stable surface. Again, therapists need to be able to match the motor program impairments causing the child with learning disabilities to fail at the task and identify what programs are needed or expressed in the success of all three individuals in Figure 3-11, A.
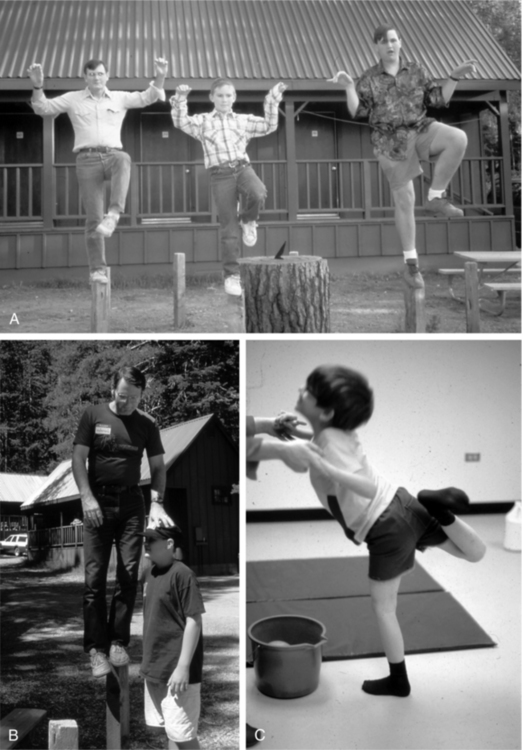

The peak of muscular strength occurs at 25 to 30 years of age in both men and women. After that period, muscle strength decreases as result of a reduction in the number and size of the muscle fibers.178 Loss is related to genetic factors, nutritional intake, exercise regimen, and daily activities.
Middle adulthood (40 to 59 years)
Changes associated with aging have been identified in the neuromuscular, musculoskeletal, and cardiovascular and pulmonary systems. These age-associated changes can greatly affect motor performance, although the degree is highly variable. Between 30 and 70 years of age, strength loss is moderate, with about 10% to 20% of total strength lost, for most activities—insignificant and undetectable by the individual.68,179 Participating in regularly scheduled exercise regimens that emphasize aerobic and strengthening activities may reduce effects associated with aging. Furthermore, developing muscle mass and competence in motor skills early in life may have long-term positive effects on adult skills and reduce the risk of disability and frailty later in life.180
Older adulthood (60+ years)
Age-related changes may be attributed to alteration in perception, compensations in the neural mechanisms, and changes between and within the different systems involved in motor skill performance.181 Integrated effects may include slowing in movement production and increased activation of agonist-antagonist muscle groups. An example of agonist-antagonist activation is during dynamic balance activities.182 After age 70 years, most individuals incur losses in muscle strength of up to 30% over the next 10 years. Overall, the loss of muscle strength through adulthood may be as much as 40% to 50% by the time an individual reaches 80 years of age.65 The percentage decline is inversely related to the demand by the individual for repetition of the movements. For example, repetitive movements, such as playing tennis daily, running, playing golf, or downhill skiing, may significantly decrease the percentage of loss of strength compared with individuals who do not participate in such activities.
Although some effects are age associated and may be reduced with regular exercise and increased motor activity, not all are modifiable. Willardson82 reported that older adults who maintain more active lifestyles are more likely to have a more favorable outcome than are peers who were not as active. Findings by Voelcker-Rehage and Willimczik97 supported the findings of Willardson82 in regard to older adults and lifestyle. In addition, Voelcker-Rehage and Willimczik97 found that older adults aged 60 to 69 years were able to acquire and refine a novel task (juggling) at a level comparable to children 10 to 14 years old and adults 30 to 59 years old. Only young adults aged 15 to 29 years performed at a higher skill level. Furthermore, adults older than age 70 years were found to have limitations in their ability to learn the novel motor skill. Moreover, as individuals age, they generally have a decreased ability to produce force, and they tend to coactivate agonist-antagonist muscles.183 The researchers suggested that older adults may coactivate agonist-antagonist muscles as a strategy to (1) modulate movement variability and (2) maintain accuracy in movement. The investigators also reported that older adults’ coactivation strategy compromised the subjects’ ability to rapidly accelerate their limbs in exchange for improved accuracy of control.
In addition, information processing appears to be slowed in older adults.181 Motor times have also been found to be delayed in older adults, particularly when a higher-level force is required.
Temporal coupling also appears to be altered in older adults.181 Perhaps as individuals age, they are less able to modulate timing of muscles during contraction and relaxation phases and are more likely to coactivate agonist-antagonist muscles. The outcome behaviors are typified by poorly coordinated motor activities and increased time to produce adequate muscle force to elicit the behavior.
In addition to reduced efficiency in movement production, variability in performance of motor skills also increases with age. Although small changes in individual systems may not have a significant effect on functional movements, the compounding effects of changes in several systems may have serious implications for older adults and place them at increased risk for falls and injuries.58 Figure 3-12, A and B are examples of movement dysfunctions seen within an elderly population. These alterations are limiting the individual’s ability to respond to a given motor task. As individuals age, there can be a large number of potential alterations in the body systems that limit CNS and musculoskeletal options when the individual tries to accomplish a motor activity. These limitations can place individuals at high risk of failure of any one motor task. The greatest fear within this group is not death; it is falling, and as a result losing independence. Prevention, as discussed in Chapter 2, will be more and more important as the world’s population of elderly individuals enlarges on a yearly basis.
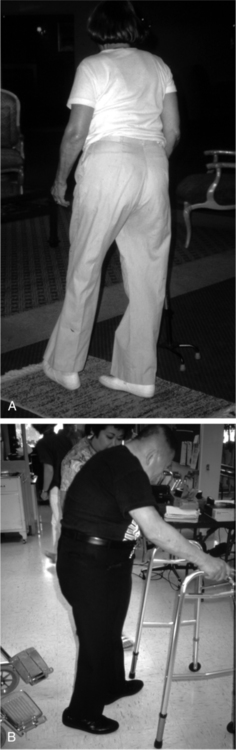

Thirty percent of all community-dwelling elderly persons fall at least once each year.179,184 Factors contributing to falls include intrinsic and extrinsic variables.185–187 Intrinsic alterations in the older adult have implications for performance of motor skills and potential for falls. Risks associated with falls increase with age and when functions of the neuromuscular, musculoskeletal, cardiovascular and pulmonary, and sensory systems deteriorate. This deterioration of covariant factors and not age itself is more closely related to health and wellness and end-of-life age.188 Another critical variable that is closely associated with motor decline in the aging is the individual’s social interactions and participation in life.189 Research has yet to determine whether a decrease in motor performance results from a decrease in participation in life.
Researchers have examined manipulative skills in older adults and reported changes in muscle performance and flexibility.56,190,191 These changes resulted in decreased hand function associated with impaired performance of ADLs.
Strategies for fostering acquisition and retention of motor behaviors across the life span
Movements occur out of a need to solve problems in the environment. Solving these problems is not dependent on any one system but rather is a collaborative effort of multiple systems. The clinician is responsible for examining the patient’s performance by evaluating the underlying conditions and the strategies that the individual may use to modify a behavior. Figure 3-13, A to F, presents an example of individuals standing up from a chair. The first panels (Figure 3-13, A and B) show a child whose feet are not on the surface because the child’s legs are not long enough. No matter the variance of the task, the child was motivated to succeed. The second individual (Figure 3-13, C and D), an elderly man, has lost the ability to shift his weight forward over his feet and thus is rising posterior on his heels, which will require anterior flexor power to prevent him from falling backward. The third individual (Figure 3-13, E and F) has residual motor problems after a stroke. She has been taught to come to stand over her less-involved leg versus centering her base of support between her two feet. The specific way an individual learns, maintains, and relearns a specific motor task as a functional activity will vary, but the important principle will be to empower the individual to succeed with fluid, dynamic motor pattern options. Therapists need to visualize movement and place the movement pattern of the individual on top of that image. The specific motor impairments will then become obvious and treatment options will be generated. Examination is vital to this process, although it often occurs in an environment far removed from the client’s natural surroundings.
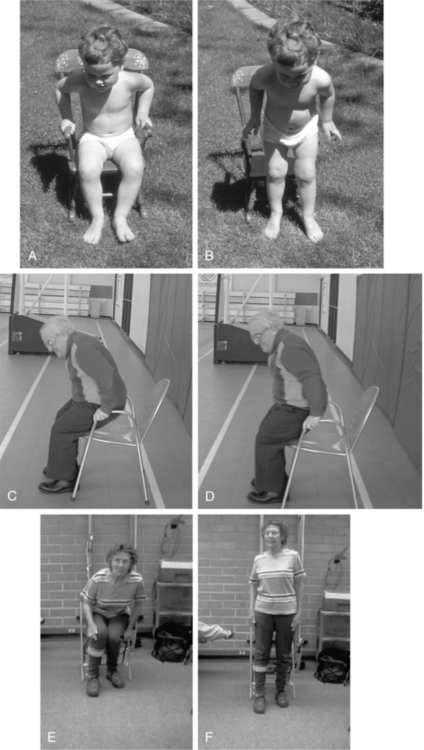

Through acquisition of motor skills, individuals of all ages are afforded the opportunity to meet the environmental demands imposed by work, play, family, or personal activities. Refer to Figure 3-13 as an example of common motor activities used at work, play, and home. Motor skill acquisition, retention, and decline are influenced by constraints or affordances that affect opportunities for practice in an environment that challenges and drives the individual to perform optimally. The client’s investment in achieving a successful outcome can help foster persistence in reaching the desired outcome.
Practice, the primary method for acquisition and retention of motor tasks, is exciting for very young children because each attempt is a new opportunity to achieve the outcome and reach a new level of independence. In contrast, practice in adolescent and adult populations may not be seen in the same light but rather as tedious and boring. Instead, physical and occupational therapists have the responsibility to challenge the cognitive, affective, motor, perceptual, sensory, and physiological systems through client-selected activities. Activities directed toward the age and needs of the individual, such as interactive dance mats for adolescent clients or ballroom dancing for the older adult, may provide the motivation necessary to practice the task a sufficient number of times to achieve the desired outcome. Figure 3-14, A to H show age-appropriate challenges to individuals. The activity used with a child may be inappropriate for use with an adult, although a similar motor behavior may be the desired outcome. If the individual identifies the activity, he will be more motivated and more likely to practice a desired skill. Carryover from a clinical setting to a home or environmental setting is critical when looking at movement function over a life span.
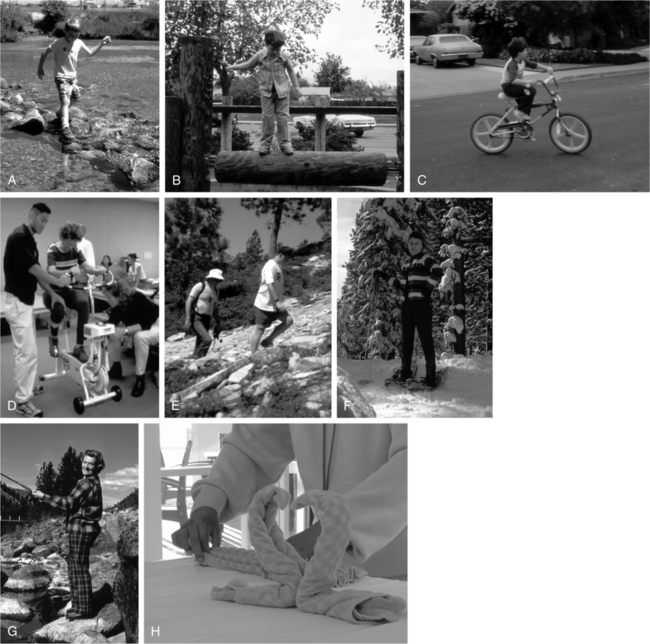

Development of head control as an example of movement development across the life span and its impact on quality of life
Flexor control
Figure 3-15, A through F, illustrates the patterns of a healthy 4-week-old when being pulled to sit and returned to the floor. Initially the child has difficulty flexing his head when trying to pull the head into flexion from the supine position because of both the extensor tactile system and the labyrinthine mechanism, which inhibit the flexors while facilitating the extensor muscles. This can be seen in Figure 3-15, A through C. This lack of adequate flexor control would be considered normal for the child’s age but also defined as a head lag (Figure 3-15, A through C). As the child approaches vertical, his weight is shifted down through his buttocks and over his base of support. At that point the head control kicks in (Figure 3-15, D and E). This motor control of the head in vertical incorporates both postural extensors and flexors while optimizing the use of optic and labyrinthine righting and stretch to both flexors and extensors muscle groups (Figure 3-15, D). The child is able to maintain better control of head and neck flexors when lowered back down to supine (Figure 3-15, E and F). This ability to control the head while transitioning from sitting to supine illustrates the fan swing principle: once the flexor program is elicited in the vertical position, it can maintain head control for a longer period of time and through more degrees of motion as the head movement progresses from vertical to horizontal.
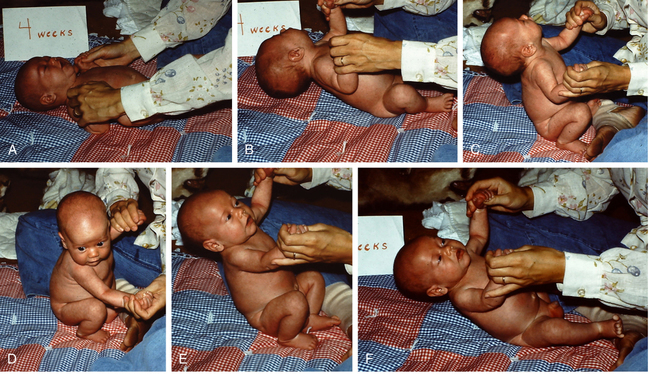

Over the next month the child will develop flexor control in space by using head righting, muscle strength, and facilitation of the nervous system to keep the head and eyes oriented toward an object as the head travels through space. Motor control over flexor patterns becomes more flexible, and the power needed to perform tasks increases. Figure 3-16, A through C, demonstrates the pull to sit pattern in a healthy 3-month-old infant. She not only has learned to dampen the influence of the TLR in the supine position and the skin’s influence on the extensor motor pool, but also has learned that by flexing most of her body parts (flexion facilitates flexion) she will gain additional flexor control of the head when pulled from supine (Figure 3-16, A). This flexion continues as the child goes through midrange (Figure 3-16, B) and continues as the child approaches vertical (Figure 3-16, C). Unfortunately, the child does not have the integrated motor control over flexion and extension or the balance reactions in sitting to extend the legs as she approaches vertical. This movement is a prerequisite for gaining control of long sitting in vertical. These new motor movements will become the foundation for balance reactions in vertical sitting.


A month later the child’s nervous system integrates the flexor patterns into smooth movement through 90 degrees of motion from supine to sitting (Figure 3-17, A through C). The child also demonstrates a more integrated response to being lowered backward from vertical (Figure 3-17, D). Yet the child’s motor system has not developed the rotatory aspects or control of the diagonal flexor patterns as shown in Figure 3-17, E. These rotatory patterns will develop as the child practices rotation in rolling and then incorporates that rotation when coming to sit in a partial rotation pattern.
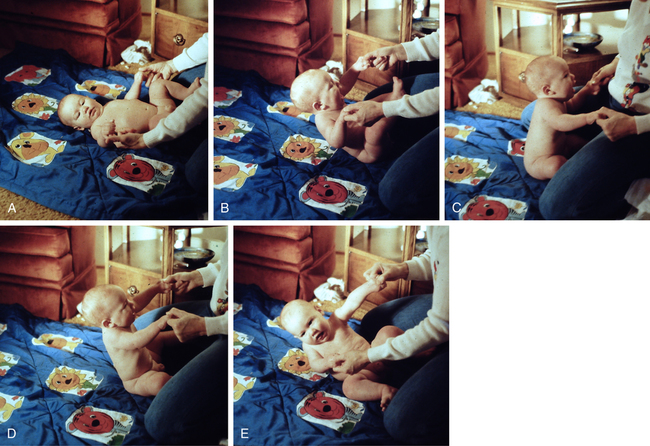

The child will not be able to independently initiate motor control over the adult pattern of coming to a sitting position for at least 3 to 5 years but certainly should gain that control by age 6 (Figure 3-18). As the child’s age increases, the movement patterns become more complex, and additional motor programs are learned and integrated. This aspect of head control will be maintained and integrated in movement patterns as the individual explores the environment.


Assessment of head control
Most individuals analyze the development of postural control by evaluating the extensor aspect of head control in the prone position. But the prone position is not the first position in which a child begins to achieve independent head control. Figure 3-19, A through C, illustrates a newborn (2 days old) extending both the long extensors (Figure 3-19, A and B) as well as moving into the postural extensor pattern component when tucking the chin (Figure 3-19, C). While prone the newborn child has very little independent control over extension and can just clear the airways (Figure 3-20). This same limitation is not present when the child is in a supported vertical position. After a week the extensor patterns in the vertical position have already become more functional and demonstrate better motor control and greater power. Figure 3-21, A through C, shows the same child at 1 week of age while supported in a vertical position. Figure 3-21, C is a beautiful example of the postural pattern one expects to see consistently later in the child’s development. Obviously, he is practicing these movements every time he is vertical and given these limited degrees of freedom. Looking at the same child at 1 month of age (Figure 3-22), the integration of these postural movements is continuing down his entire spine. This does not mean he can hold this pattern for an extended period of time but does illustrate his ability to move with control into a total postural extension pattern and hold it at least briefly. On the same day and about 15 minutes later, the child (Figure 3-23) was placed prone on the floor, clearly demonstrating that he has not developed the necessary power to control his head or upper trunk for postural extension in the prone position. Although he is more relaxed prone at 1 month than at birth (see Figure 3-20) and can lift and turn his head in both directions, it will still be 1 or 2 additional months before he can extend his head and trunk enough to prop on his elbows. It will take more time to roll from prone to supine.









 Same child when placed prone, 15 minutes after Figure 3-22 was taken. This child demonstrates that when prone he still has a flexor bias and has little adequate postural extension in this position.
Same child when placed prone, 15 minutes after Figure 3-22 was taken. This child demonstrates that when prone he still has a flexor bias and has little adequate postural extension in this position.While the cervical and upper thoracic muscles are developing postural power, they need to learn to hold the head in space against gravity for longer periods of time. Postural function requires coordination and coactivation of the short extensors of the neck and the neck flexors—especially the sternocleidomastoid, hyoid, and scalene muscles—in order to tuck the chin and balance the head in space. These movement patterns play a key role in stabilization of the head in order to move the head in and out of vertical space. The motor control system uses both righting and balance reactions in order to gain full head and neck control of vertical space. The movements become more and more complex, modifying and integrating various additional motor programs in order to have greater flexibility to control and move the head. These patterns give the eyes and ears the visual and auditory orientation needed to process consistent external environmental information. Figure 3-24 illustrates an individual after head injury who has lost his automatic righting of the head in vertical. He has the ability to bring his head to vertical by hyperextension of the neck but does not do so automatically. This hyperextension pattern dramatically changes the motor patterns of head, neck, and trunk control which will affect his upright behaviors including balance, gait, feeding, and social interactions.


Analysis between normal and impaired motor function
Differentiating normal age-related reactions of any movement impairment is the responsibility of a movement specialist. For example, differentiating the movement of a normal child who has a lag in head control (see Figure 3-15, B and C) from the movement of a child who does not demonstrate any head control (Figure 3-25, A through E) should guide the therapist in a decision about where to begin treatment. It is an unrealistic expectation for the child in Figure 3-25 to gain flexor head control by starting at supine. After the child has been pulled to sit, flexor power production is beyond the control of the child’s motor system. Once the child is vertical, the influence of gravity on the weight of the head has decreased. The vertical position also inhibits any influence of the otoliths when supine. The upright position helps to facilitate the labyrinthine and optic righting of the head. Figure 3-25, D and E demonstrates how the tone within the neck and shoulder girdle changes once the head attains a vertical position. A therapist should not only see a change to more normal tonal patterns but also observe relaxation of the facial muscles—closure of the mouth and a more functional position of the eyes in space for visual processing.
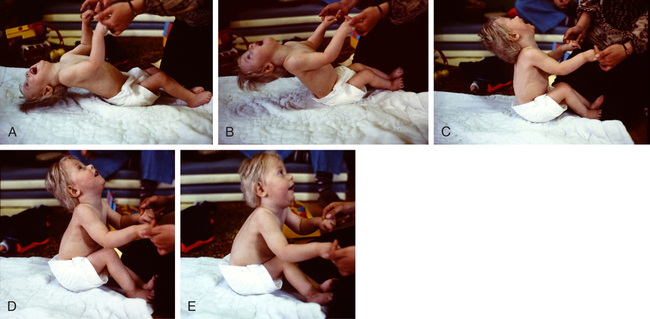

Movement demonstrates the ease or difficulty the motor system is experiencing while trying to complete an activity. The activity analyzed may be a basic pattern such as head control or a complex one as seen in Figure 3-3, E. Differentiating between the movements in Figure 3-15, A and Figure 3-25, A should guide the clinician in establishing realistic prognoses. The first child, with practice and CNS maturity, should automatically develop head control, whereas the second child has gone beyond his age-appropriate movement delays and has abnormal responses to the stretch stimuli.
Similar analysis can be made when looking at the extensor component of head control. The vertical position that optimizes extension is kneeling or standing because compression down through the joints and spine facilitates extension. Using kneeling or standing may pull in too much extension, especially if it results in hyperextension. In that case sitting may be appropriate even though it may facilitate flexion. When kneeling or standing, if inadequate extension still exists, then adding additional compression (see Chapter 9, p. 207) down though the head or shoulder girdle may help. Using an apparatus that takes away some of the weight of the head or trunk reduces the demand on the nervous system and may help the individual regain postural neck, shoulder girdle, and upper trunk control (see Chapter 9, p. 232). As the individual begins to demonstrate that control, the therapist can slowly take away the assistance with the expectations that the individual will gain independence in that activity.
As the individual ages, changes in the control of the head can lead to new problems. Figure 3-12, B, is an example of a man who has a fixed flexed posture. If the flexed posture is permanent, treatment alternatives must take into consideration the impact this posturing will have on all ADLs. As stated earlier, any patient can exhibit a range of problems in head control. How those movement impairments present themselves and which treatment alternatives a therapist might select will depend on the clinician’s ability to analyze normal movement and create an optimal environment for patients to engage and practice those patterns.
Summary
Clinicians must focus best practice toward successful client management geared toward promotion of function and prevention of chronic illness or disability for the youngest of the young to the oldest of the old. As practitioners, we must embrace tenets central to the Healthy People 2020 project. Physical and occupational therapists serve as role models for individuals of all ages and educate diverse groups of individuals about the multifaceted, interactive systems involved in the acquisition, retention, and deterioration of motor behaviors. Recognizing internal and external constraints or affordances that influence motor behaviors enables the clinician to devise a plan of care and the scientist to design a study targeting the needs of the whole person. Analyzing, understanding, and visually recognizing movement patterns that are efficient, fluid, and goal oriented and that vary across the life span are the first steps or prerequisites to evaluating abnormal movement patterns that do not fall within a normal parameter. Figure 3-26, A to G, shows an example of rolling, a basic movement strategy controlled by the child midway through the first year of life that can become an extremely challenging activity after a CNS insult. Differentiating between components of a normal movement and deviations that prohibit normal movement falls into the clinical expertise of occupational and physical therapists (see Chapter 9, Figure 1-9, p. 199) Without the knowledge of normal movement, analysis of the causation of abnormal movement would be difficult if not impossible. This chapter has been written to help the reader understand normal movement across the life span. It is the first step, and in sighted individuals the analysis begins as soon as visual images are recorded in the visual cortex.
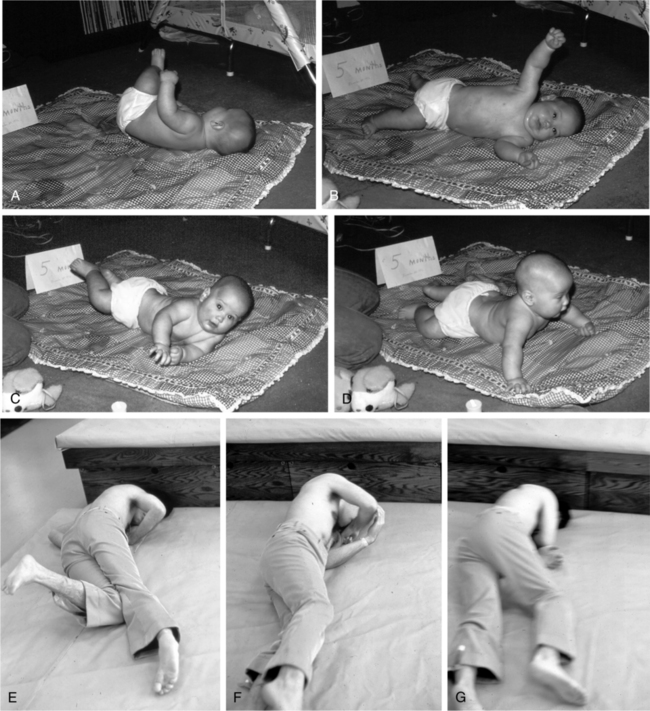

Scientists acknowledge that development is characterized as nonlinear, emergent, and dynamic, rather than sequential, predictable, and stagelike. Dynamic systems theory, although it does have certain limitations, provides a better explanation for development than do neuromaturational theories. The emphasis or responsibility does not lie with any one system but varies across different systems as a consequence of age, genetics, or experience.104 That said, future studies directed at examining human movement and optimal variability through nonlinear dynamics may provide new perspectives in motor development and control.