[level-membership-for-radiology-category] Soft tissue, fat, or air density along heart border
Usually located in right cardiophrenic angle and anterior to heart on lateral view
Smoothly marginated with silhouetting of heart border
• CT and MR Findings
Defect in retrosternal part of diaphragm with hernia sac extending upwards anterior to heart
Hernia sac most often contains only omental fat
Can also contain: Transverse colon > liver > small bowel > stomach
Hernias in adults usually contain omental fat; involvement of bowel or liver more likely in children
With pericardial defect, hernia sac may protrude into pericardial cavity or heart may protrude downwards
TOP DIFFERENTIAL DIAGNOSES
• Pericardial fat pad
• Mediastinal and thoracic masses
• Pulmonary parenchymal lesions
CLINICAL ISSUES
• Rare, 3-4% of all diaphragmatic hernias
• Most cases are diagnosed in adults
• Often asymptomatic in adults, and more likely symptomatic in children
Symptoms often include chronic GI complaints
Rarely acute symptoms due to incarceration, strangulation, obstruction, or volvulus
• Surgical repair in symptomatic patients via thoracotomy, laparotomy, or laparoscopic approach
• Surgical repair in asymptomatic patients more controversial
(Left) Frontal radiograph shows a large, relatively lucent mass in the right costophrenic angle.
(Right) Axial NECT in the same patient shows that the opacity on the radiograph corresponds to a fat-containing mass in the right cardiophrenic angle.
(Left) Sagittal NECT in the same patient shows that the previously visualized fatty mass actually represents a Morgagni hernia with omental fat herniating into the chest. Notice the discrete defect in the diaphragm and the numerous small omental vessels extending upwards into the hernia sac.
(Right) Coronal NECT in the same patient again demonstrates the Morgagni hernia with a discrete diaphragmatic defect and omental fat herniating into the chest.
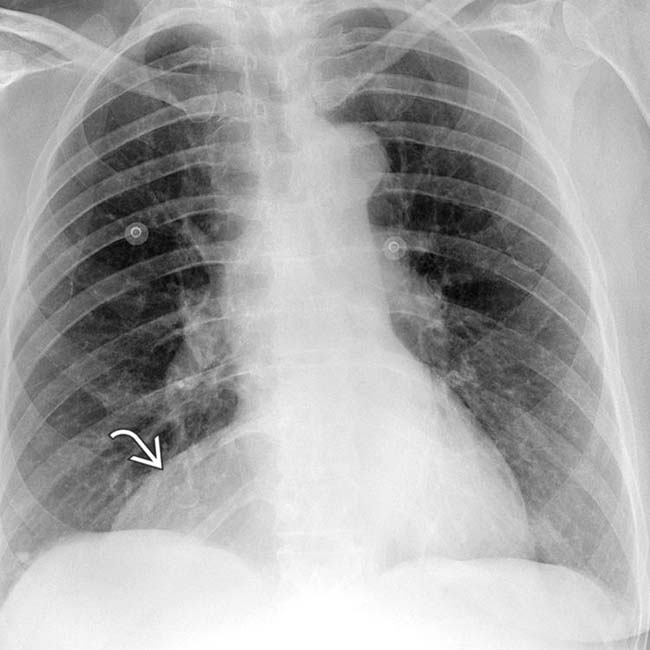
Frontal radiograph shows an abnormal opacity in the right costovertebral angle , which widens the right heart contour.
Axial CECT image demonstrates herniation of omental fat through the Morgagni hiatus in the right cardiophrenic angle, in keeping with a Morgagni hernia. Most Morgagni hernias contain only omental fat without involvement of the bowel or liver.
AP chest radiograph in a 71-year-old man with “bloating” shows intrathoracic gas bubbles superolaterally and centrally . The location and etiology of these are uncertain.
Lateral chest radiograph shows intrathoracic gas bubbles both anteriorly, representing a herniated colon in a large Morgagni hernia and more centrally in the stomach within a large hiatal hernia .
Axial CT in the same patient shows the large hernias. The hiatal (paraesophageal) hernia contains fat and much of the stomach, while the Morgagni hernia contains fat and colon.
Coronal reformat of CT shows the Morgagni hernia and its contents. The paraesophageal hernia is not included in this plane.
Frontal radiograph shows a large mass within the right anterolateral thorax.
Lateral radiograph in the same patient again shows that the previously seen mass is located anterior to the heart and contains several air-filled loops of bowel. This constellation of findings is diagnostic of a Morgagni hernia.
Axial CECT sections in the same patient show herniation of abdominal fat and a portion of the colon into the right anterior chest, in keeping with a Morgagni hernia.
[/level-membership-for-radiology-category][not-level-membership-for-radiology-category] Soft tissue, fat, or air density along heart border
Usually located in right cardiophrenic angle and anterior to heart on lateral view
Smoothly marginated with silhouetting of heart border
• CT and MR Findings
Defect in retrosternal part of diaphragm with hernia sac extending upwards anterior to heart
Hernia sac most often contains only omental fat
Can also contain: Transverse colon > liver > small bowel > stomach
Hernias in adults usually contain omental fat; involvement of bowel or liver more likely in children
With pericardial defect, hernia sac may protrude into pericardial cavity or heart may protrude downwards
TOP DIFFERENTIAL DIAGNOSES
• Pericardial fat pad
• Mediastinal and thoracic masses
• Pulmonary parenchymal lesions
CLINICAL ISSUES
• Rare, 3-4% of all diaphragmatic hernias
• Most cases are diagnosed in adults
• Often asymptomatic in adults, and more likely symptomatic in children
Symptoms often include chronic GI complaints
Buy Membership for Radiology Category to continue reading. Learn more here








 in the right costophrenic angle.
in the right costophrenic angle.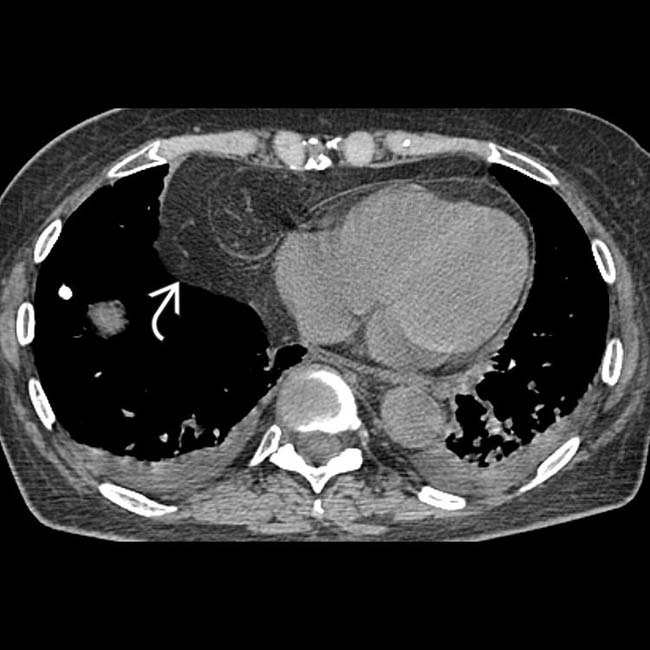
 in the right cardiophrenic angle.
in the right cardiophrenic angle.
 in the diaphragm and the numerous small omental vessels
in the diaphragm and the numerous small omental vessels  extending upwards into the hernia sac.
extending upwards into the hernia sac.
 and omental fat herniating into the chest.
and omental fat herniating into the chest.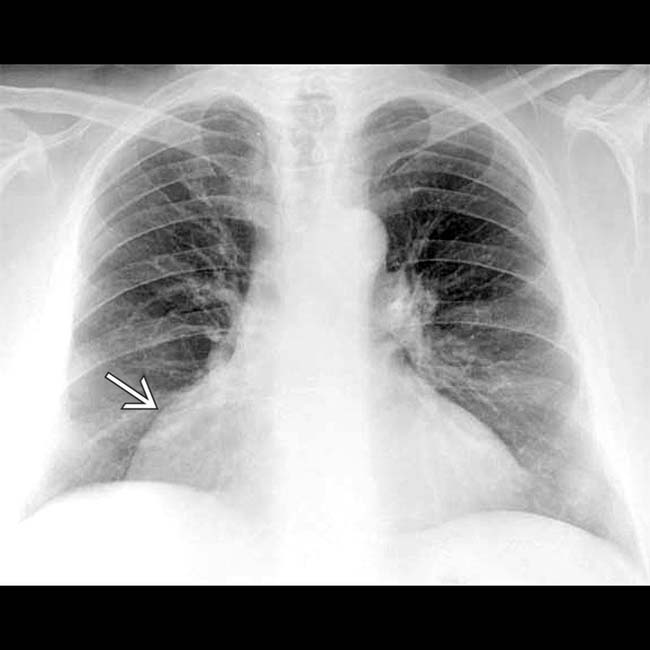
 , which widens the right heart contour.
, which widens the right heart contour.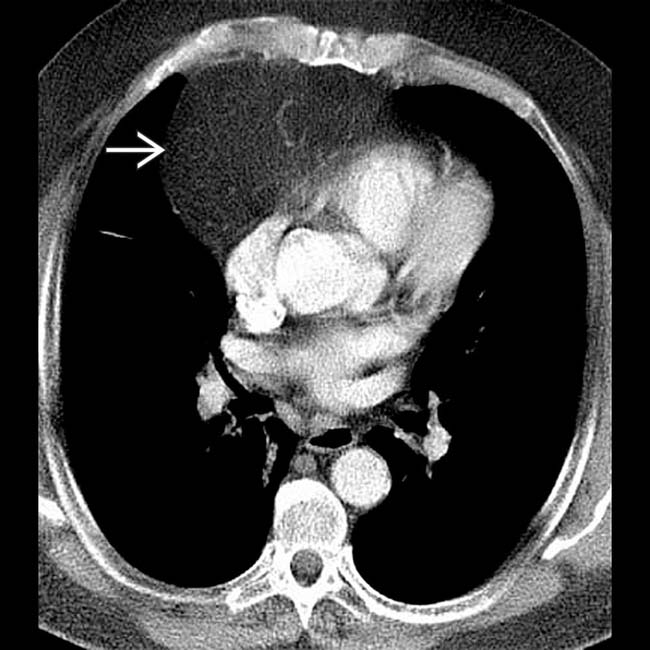
 through the Morgagni hiatus in the right cardiophrenic angle, in keeping with a Morgagni hernia. Most Morgagni hernias contain only omental fat without involvement of the bowel or liver.
through the Morgagni hiatus in the right cardiophrenic angle, in keeping with a Morgagni hernia. Most Morgagni hernias contain only omental fat without involvement of the bowel or liver.
 and centrally
and centrally  . The location and etiology of these are uncertain.
. The location and etiology of these are uncertain.
 and more centrally in the stomach within a large hiatal hernia
and more centrally in the stomach within a large hiatal hernia  .
.
 contains fat and much of the stomach, while the Morgagni hernia
contains fat and much of the stomach, while the Morgagni hernia  contains fat and colon.
contains fat and colon.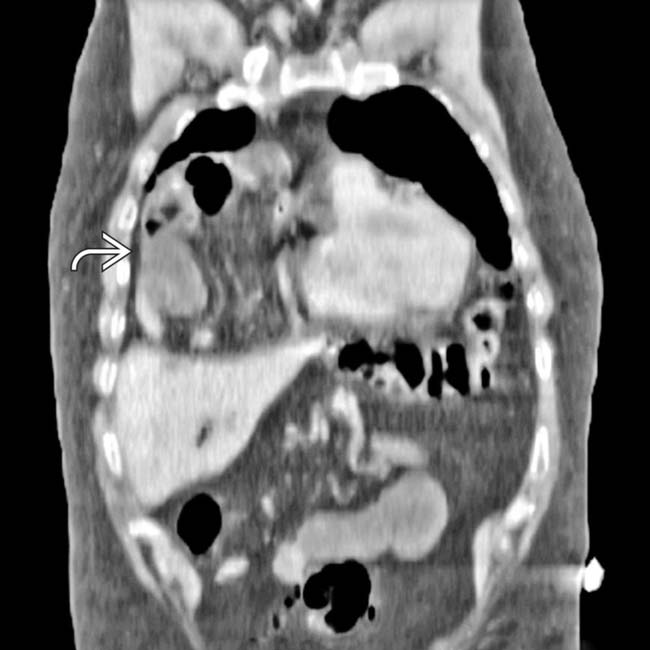
 and its contents. The paraesophageal hernia is not included in this plane.
and its contents. The paraesophageal hernia is not included in this plane.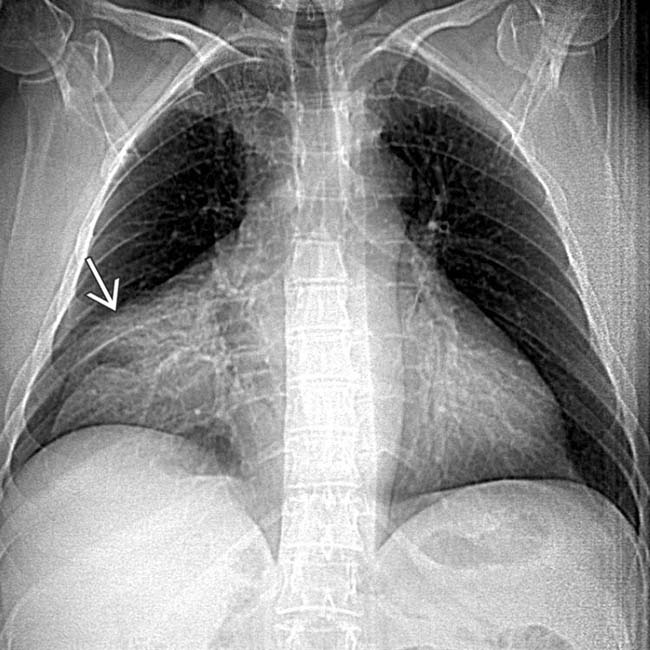
 within the right anterolateral thorax.
within the right anterolateral thorax.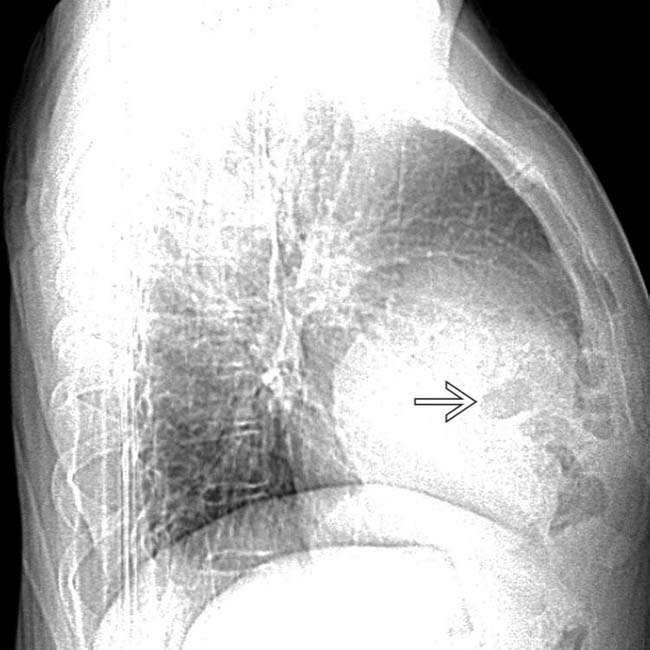
 is located anterior to the heart and contains several air-filled loops of bowel. This constellation of findings is diagnostic of a Morgagni hernia.
is located anterior to the heart and contains several air-filled loops of bowel. This constellation of findings is diagnostic of a Morgagni hernia.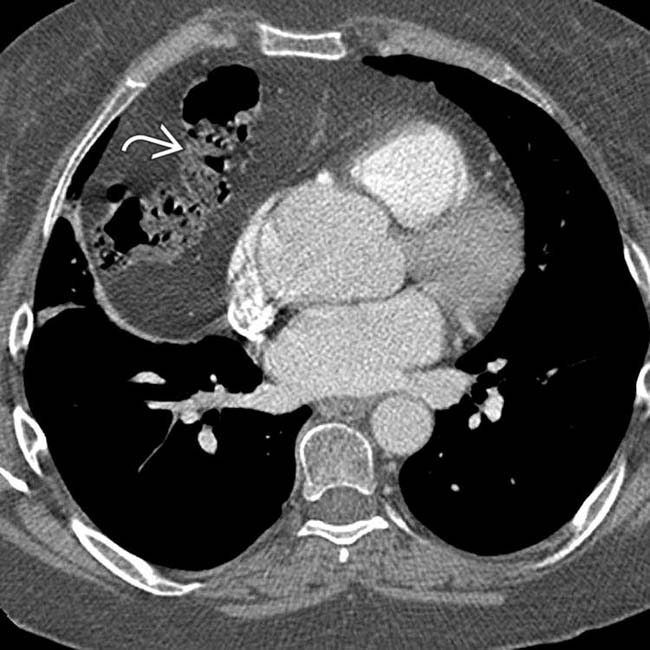
 into the right anterior chest, in keeping with a Morgagni hernia.
into the right anterior chest, in keeping with a Morgagni hernia.
