6 Mixed aortic valve lesion
Salient features
• Pulse may be bisferious, small volume or large volume depending on the dominant lesion
• There is a displaced apex beat (remember a small LV is inconsistent with chronic severe aortic regurgitation)
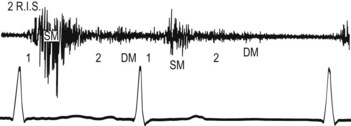
• Early diastolic murmur of aortic regurgitation (Fig. 6.1)
• Ejection systolic murmur of aortic stenosis
• Proceed by telling the examiner that you would like to check the BP, in particular to determine the pulse pressure (systolic minus diastolic pressure).
Questions
What is the pathophysiology of mixed aortic valve disease?
• In mixed aortic valve disease, one lesion usually predominates over the other and the pathophysiology resembles that of the pure dominant lesion. When aortic stenosis predominates, the pathophysiology and, therefore, the management resembles that of pure aortic stenosis (J Am Coll Cardiol 1998;32:1486–588). The LV in these patients develops concentric hypertrophy rather than dilatation. The timing of aortic valve replacement (like pure aortic stenosis) depends on symptoms (Circulation 1998;98:1949–84).
• When aortic regurgitation is more than mild and the aortic stenosis is predominant, the concentrically hypertrophied and non-compliant LV is on the steeper portion of the diastolic pressure–volume curve, resulting in pulmonary congestion. Therefore, although neither lesion by itself is severe enough to merit surgery, both together produce substantial haemodynamic compromise requiring surgery (Circulation 1998;98:1949–84).
• When the aortic regurgitation is severe and the aortic stenosis is mild, the high total stroke volume caused by extensive regurgitation may produce a substantial transvalvular gradient. Because the transvalvular gradient varies with the square of the transvalvular flow (Am Heart J 1951;41:1–29), a high gradient in predominant regurgitation may be predicted primarily on excess transvalvular flow rather than on a severely compromised orifice area (Circulation 1998;98:1949–84).
In mixed aortic valve disease is cardiac catheterization more accurate than Doppler echocardiography to measure valve area?
How would you manage such a patient?
• Surgical correction of disease that produces more than mild symptoms
• When the aortic stenosis is dominant, surgery in the presence of even mild symptoms
• When the aortic regurgitation is dominant, surgery can be delayed until symptoms develop or asymptomatic LV dysfunction become apparent on echocardiography.





