20 Mitral valve prolapse
Instruction
Examination
• Midsystolic click followed by late or midsystolic murmur
• Look for features of Marfan syndrome (high arched palate, arm span greater than height).
Notes
• Squatting will bring the midsystolic click closer to the second heart sound and decrease the duration of the murmur.
• A Valsalva manoeuvre and standing have the opposite effect.
• The midsystolic murmur begins after the first heart sound; the late systolic murmurs begin after the first heart sound but continue to or through the second heart sound (S2). Both types of murmur may have a crescendo–decrescendo configuration
Questions
What are eponyms for mitral valve prolapse?
Barlow syndrome (Br Heart J 1968;30:203), click–murmur syndrome, floppy mitral valve.
What is the prevalence in the normal population?
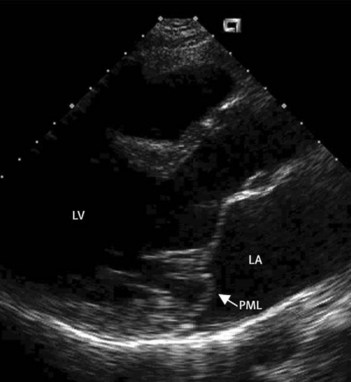
The new awareness that the mitral valve is saddle shaped rather than a planar valve has resulted in new echocardiographic definition for mitral valve prolapse as one or both mitral leaflets exhibit at least 2 mm displacement superior to the long-axis annular plane (a line connecting the annular hinge points), with or without leaflet thickening (Fig. 20.1). With this new description, the prevalence of prolapse is estimated at 2–3%, and is equally distributed between men and women.
How would you manage such patients?
• Reassure the asymptomatic patient
• Relief of atypical chest pain with analgesics or beta-blockers (empiric treatment)
• Aspirin or anticoagulants in those with transient ischaemic attacks
• Antiarrhythmics in those with frequent tachyarrhythmias or ventricular premature contractions
• Prophylaxis for infective endocarditis (see Case 17)
• Consider surgery in those with severe mitral regurgitation.
Advanced-level questions
Which segments of the mitral valve commonly prolapse?
• Most cases of prolapse involve the posterior middle scallop (easily identified on long-axis echocardiographic images)
• Lateral scallop prolapse (not clearly seen on long-axis images; this aspect is best seen in the apical four-chamber view).
Notes
• Superior leaflet displacement in a four-chamber view should not be judged diagnostic of prolapse. Therefore, transthoracic echocardiography can confirm the diagnosis of prolapse but may not be able to exclude lateral scallop prolapsed without taking into account several planes of imaging. Transoesophageal echocardiography is, consequently, very effective in identifying prolapsing segments.





