Chapter 10 Minor complications of pregnancy
DISPLACEMENT OF THE UTERUS
Uterovaginal prolapse
In multiparous women, particularly in the developing countries, uterovaginal prolapse may complicate pregnancy. In the early weeks of pregnancy the prolapse may become more prominent. As the uterus becomes an abdominal organ the pressure on the vagina is relieved to some extent, and the prolapse becomes less obvious. Occasionally a swollen, infected cervix may protrude through the vulva. The prolapse causes few problems during labour and cervical dilatation is usually rapid. Pregnancy after a vaginal repair for prolapse is considered on page 307.
NAUSEA AND VOMITING
Nausea and vomiting may be graded as mild, moderate or severe.
OEDEMA
Oedema associated with a rise in blood pressure requires further investigation, particularly when the hands or face become oedematous (see Ch. 14).
PUBIC SYMPHYSIS DIASTASIS (PELVIC OSTEOARTHROPATHY)
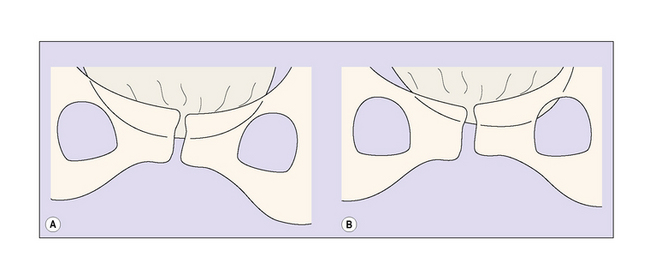
In a few women abnormal relaxation of the ligaments surrounding the pubic joint permits the pubic bones to move on each other when the woman walks or exerts herself. This movement may put strain on the sacroiliac joints. Pubic symphysis diastasis may occur during pregnancy or start in the puerperium. The pain may persist for the remainder of the pregnancy or for several weeks after the birth, which makes care of the neonate difficult. The patient complains of severe pubic pain, backache and sacral pain. Examination shows that the pubic joint is very tender when pressed. The diastasis can be confirmed by ultrasound or X-ray examination (Fig. 10.1). Treatment consists of bed rest on a firm mattress, with the patient nursed as far as is possible on one or other side.
VAGINAL DISCHARGES
In pregnancy the quantity of normal vaginal secretions increases and many women complain of a non-irritant vaginal discharge. Vaginal infections, particularly candidiasis, are more frequent in pregnant women than in non-pregnant women. Vaginal discharges are discussed on pages 260–262.