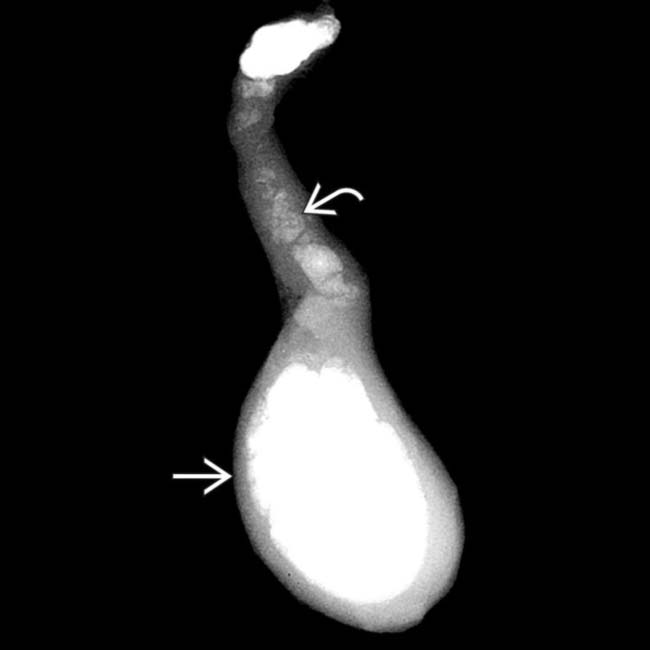
(Left) Frontal radiograph demonstrates extensive milk of calcium bile filling the gallbladder (GB) .
(Right) Specimen radiograph in the same patient after cholecystectomy demonstrates milk of calcium bile in both the GB and cystic duct .
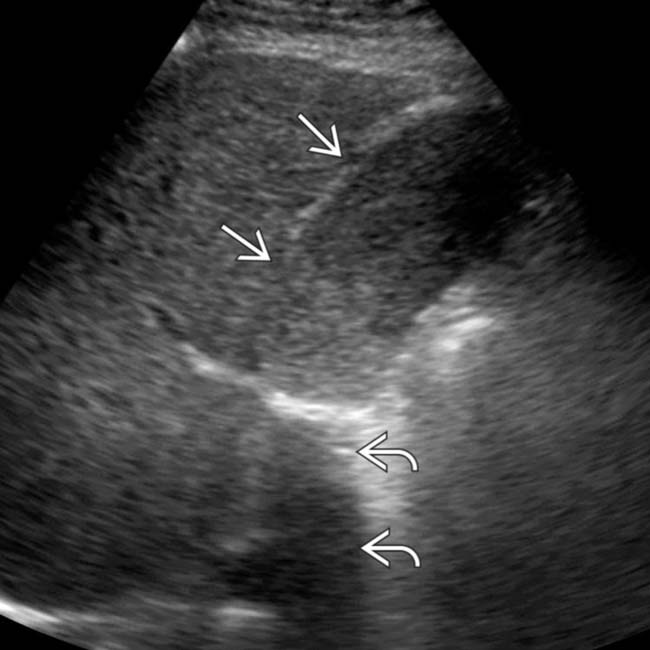
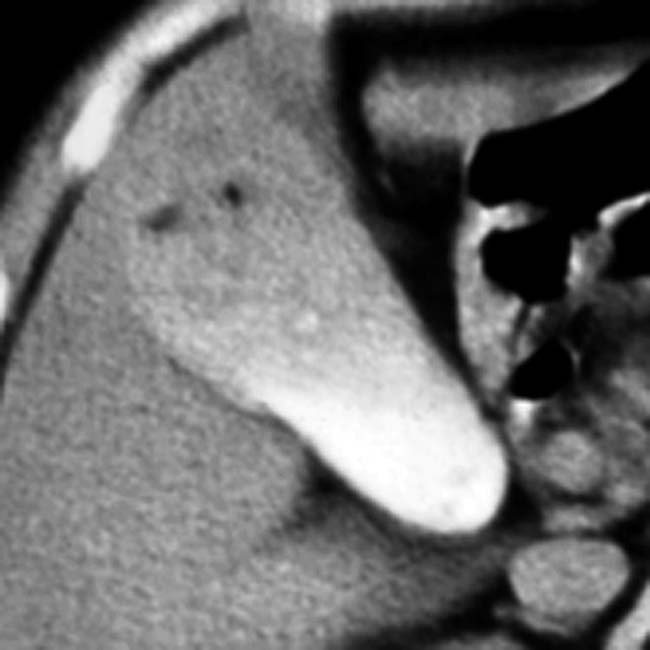
(Left) Ultrasound shows diffuse low-level echo sludge within the GB lumen with posterior acoustic shadowing . Sludge and shadowing were not present on an ultrasound performed 6 months later.
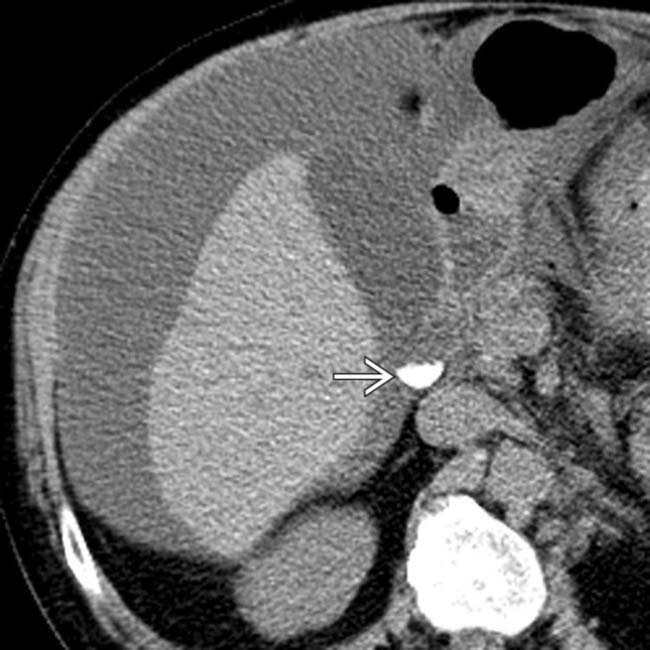
(Right) Axial CECT shows high-density milk of calcium bile filling the GB lumen. The GB also demonstrates subtle wall calcification and a gallstone . There is a frequent association of gallstones and milk of calcium bile.
TERMINOLOGY
Synonyms
• Limy bile syndrome, calcium carbonate bile
Definitions
• High-density calcium carbonate precipitate within gallbladder (GB) lumen
IMAGING
General Features
• Best diagnostic clue
High-density layering liquid/sediment within GB
• Location
GB lumen
Radiographic Findings
• Radiography
Opacification of GB with high-density, radiopaque fluid
– Fluid-fluid level on upright film
Less commonly, opacification of cystic duct &/or common bile duct
– Always occurs in patients who also have milk of calcium bile in GB
– Exclamation sign: Coexisting milk of calcium bile and gallstones in common bile duct
CT Findings
• NECT
High-attenuation (> 150 HU) sediment in GB (rarely in cystic duct and common bile duct)
MR Findings
• Calcium carbonate layers dependently in GB and shows low T2WI signal
Differentiate from gallstones, which appear as discrete nodules of low T2WI signal
Ultrasonographic Findings
• Mixed echogenicity material within GB which might cause acoustic shadowing
Echogenicity slightly higher than typical sludge, but may be indistinguishable from sludge if no shadowing
• May have associated gallstones (including chronically obstructing stones in GB neck or cystic duct)
Gallbladder wall thickening if acute cholecystitis
Nuclear Medicine Findings
• Hepatobiliary scintigraphy
Nonfilling of GB if cystic duct is obstructed
Imaging Recommendations
• Best imaging tool
NECT
DIFFERENTIAL DIAGNOSIS
Vicarious Excretion of Contrast
• Hepatic excretion of iodinated contrast
• Can be a normal finding on CT, but tends to be most conspicuous in patients with renal failure
Gallbladder Sludge
• Layering, mobile, avascular echogenic material without posterior acoustic shadowing
May appear mass-like (tumefactive sludge)
• Avascular with color Doppler
Porcelain Gallbladder
• Diffuse or focal calcification of GB wall with posterior acoustic shadowing on US
• Associated with increased risk of GB carcinoma
Gallbladder Hemorrhage
• High-attenuation (> 30 HU) fluid in GB
• Echogenic on ultrasound without acoustic shadowing
May not be easily distinguishable from sludge on US
Iatrogenic Opacification of Gallbladder
• Oral cholecystography can mimic milk of calcium bile with high-density, contrast-filling gallbladder
PATHOLOGY
General Features
• Etiology
Chronic cystic duct obstruction with resultant biliary stasis
May be associated with long-term total parenteral nutrition (TPN)
• Associated abnormalities
Cholelithiasis (60-100% of cases in different series)
Chronic cholecystitis often present, but likely secondary finding that is not true cause of milk of calcium bile
Gross Pathologic & Surgical Features
• Semi-solid, paste-like material almost completely composed of calcium carbonate
CLINICAL ISSUES
Presentation
• Most common signs/symptoms
May be asymptomatic
Most patients have biliary colic similar to cholelithiasis: Intermittent RUQ pain
• Other signs/symptoms
Fever and jaundice as result of biliary obstruction
• Clinical profile
May be associated with many complications commonly seen with cholelithiasis
Usually middle-aged adults (very rare in children)
42-66 years
– Almost always occurs in adults (very rare in children)
• Gender
F > M
• Epidemiology
Found in 0.1-1.7% of cholecystectomy specimens
Natural History & Prognosis
• Incidental finding which may be asymptomatic
• Symptoms may be secondary to milk of calcium bile itself or concomitant gallstones)
Biliary colic, acute cholecystitis, cholangitis, or acute pancreatitis
Treatment
• No treatment in asymptomatic patients
• Cholecystectomy for symptomatic patients
DIAGNOSTIC CHECKLIST
Consider
• GB sludge or hemorrhage
Image Interpretation Pearls
• High-density material layering in GB on NECT
Axial NECT of milk of calcium bile in an asymptomatic patient reveals high-attenuation liquid layering posteriorly in the gallbladder .
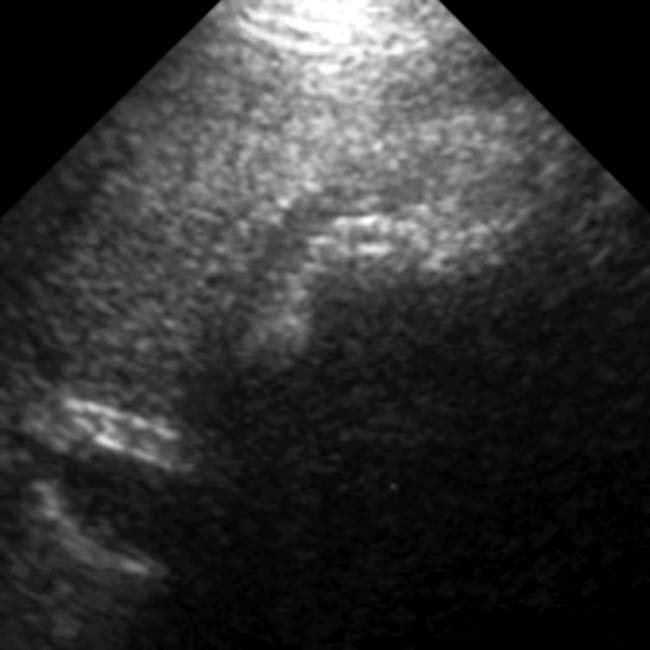
Transverse ultrasound of milk of calcium bile shows echogenic material with acoustic shadowing.
Axial NECT reveals high-attenuation milk of calcium bile in the gallbladder.
Supine frontal radiograph demonstrates a typical appearance of milk of calcium bile. There is a hazy increased density within the gallbladder . This represents limy bile, the precipitation of calcium carbonate into the bile within the gallbladder.
Axial NECT demonstrates layering hyperdense material within the gallblader consistent with milk of calcium bile. Note that the gallbladder is distended, consistent with stasis (a frequent association).
Frontal abdominal radiograph in a 79-year-old man who presented with chronic abdominal pain demonstrates the calcified appearance of the GB .
Coronal CECT in a 43-year-old man presenting with abdominal pain demonstrates layered hyperdense material within the gallbladder, findings consistent with milk of calcium bile. Note that the gallbladder is distended, consistent with stasis.
[/level-membership-for-radiology-category][not-level-membership-for-radiology-category] Opacification of GB with high-density, radiopaque fluid
– Fluid-fluid level on upright film
Rarely opacification of cystic duct or common bile duct (CBD)
– Exclamation sign: Coexisting milk of calcium bile and gallstones in CBD
– Occurs only in patients who also have milk of calcium bile in gallbladder
• CT: High-attenuation (> 150 HU) sediment
• MR: Low signal on T2WI and layers dependently
Differentiate from gallstones which are discrete nodules with low T2WI signal
• Ultrasound
Mixed echogenicity, layering material within GB which might cause acoustic shadowing
Echogenicity slightly higher than typical sludge, but may be indistinguishable from sludge if no shadowing
May have associated gallstones
TOP DIFFERENTIAL DIAGNOSES
• Vicarious excretion of contrast
• GB sludge
• Porcelain GB
• GB hemorrhage
PATHOLOGY
• Etiology: Chronic cystic duct obstruction with resultant biliary stasis
CLINICAL ISSUES
• Incidental finding which may be asymptomatic
• Most patients have symptoms of biliary colic
Symptoms may be due to either milk of calcium bile or concomitant gallstones
• Associated with complications similar to cholelithiasis
(Left) Frontal radiograph demonstrates extensive milk of calcium bile filling the gallbladder (GB) .
(Right) Specimen radiograph in the same patient after cholecystectomy demonstrates milk of calcium bile in both the GB and cystic duct .
(Left) Ultrasound shows diffuse low-level echo sludge within the GB lumen with posterior acoustic shadowing . Sludge and shadowing were not present on an ultrasound performed 6 months later.
(Right) Axial CECT shows high-density milk of calcium bile filling the GB lumen. The GB also demonstrates subtle wall calcification and a gallstone . There is a frequent association of gallstones and milk of calcium bile.
TERMINOLOGY
Synonyms
• Limy bile syndrome, calcium carbonate bile
Definitions
• High-density calcium carbonate precipitate within gallbladder (GB) lumen
IMAGING
General Features
• Best diagnostic clue
High-density layering liquid/sediment within GB
• Location
GB lumen
Radiographic Findings
• Radiography
Opacification of GB with high-density, radiopaque fluid
– Fluid-fluid level on upright film
Buy Membership for Radiology Category to continue reading. Learn more here








 .
.
 and cystic duct
and cystic duct  .
.
 within the GB lumen with posterior acoustic shadowing
within the GB lumen with posterior acoustic shadowing  . Sludge and shadowing were not present on an ultrasound performed 6 months later.
. Sludge and shadowing were not present on an ultrasound performed 6 months later.
 and a gallstone
and a gallstone  . There is a frequent association of gallstones and milk of calcium bile.
. There is a frequent association of gallstones and milk of calcium bile.























 .
.

 . This represents limy bile, the precipitation of calcium carbonate into the bile within the gallbladder.
. This represents limy bile, the precipitation of calcium carbonate into the bile within the gallbladder.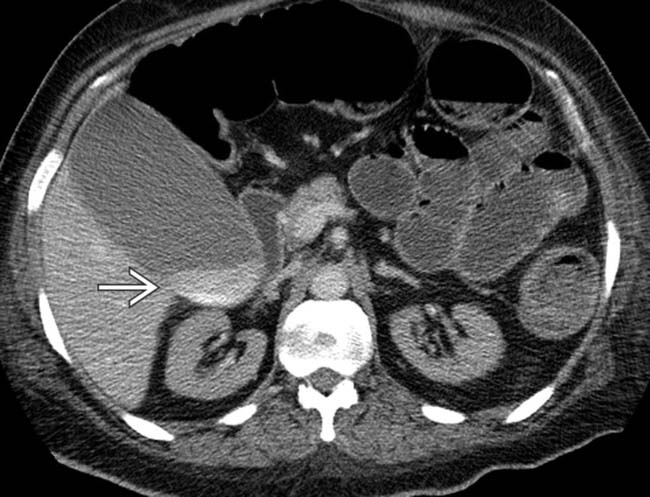
 within the gallblader consistent with milk of calcium bile. Note that the gallbladder is distended, consistent with stasis (a frequent association).
within the gallblader consistent with milk of calcium bile. Note that the gallbladder is distended, consistent with stasis (a frequent association).
 .
.
 within the gallbladder, findings consistent with milk of calcium bile. Note that the gallbladder is distended, consistent with stasis.
within the gallbladder, findings consistent with milk of calcium bile. Note that the gallbladder is distended, consistent with stasis.
