Metabolic acid–base disorders
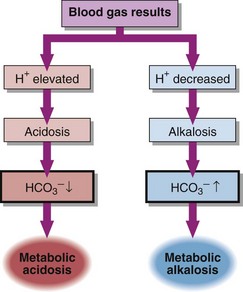
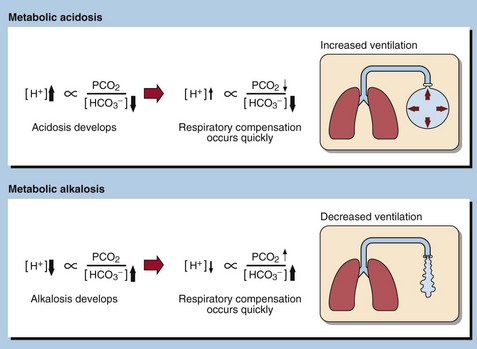
Metabolic acid–base disorders are caused by an increase in H+ production or a loss of H+ triggering compensatory mechanisms that result in the loss or gain of HCO3−. Direct loss or gain of HCO3− will also cause metabolic acid-base disorders. Primary metabolic acid–base disorders are recognized by inspecting the bicarbonate concentration (Fig 21.1). Respiratory compensation takes place quickly so patients with metabolic acid–base disorders will usually show some change in blood PCO2 because of hyperventilation or hypoventilation (Fig 21.2).
Metabolic acidosis
In a metabolic acidosis the primary problem is a reduction in the bicarbonate concentration of the extracellular fluid. The main causes of a metabolic acidosis are shown in Figure 21.3. These are:
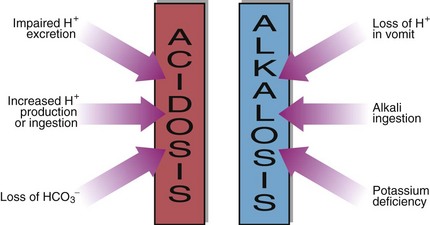
 increased production of hydrogen ions
increased production of hydrogen ions
 ingestion of hydrogen ions, or of drugs that are metabolized to acids
ingestion of hydrogen ions, or of drugs that are metabolized to acids
 impaired excretion of hydrogen ions by the kidneys
impaired excretion of hydrogen ions by the kidneys
 loss of bicarbonate from the gastrointestinal tract or in the urine.
loss of bicarbonate from the gastrointestinal tract or in the urine.

Causes of metabolic acidosis






Clinical effects of acidosis
A raised [H+] leads to increased neuromuscular irritability. There is a hazard of arrhythmias progressing to cardiac arrest, and this is made more likely by the presence of hyperkalaemia, which will accompany the acidosis (pp. 22–23). Depression of consciousness can progress to coma and death.
Metabolic alkalosis
The causes of a metabolic alkalosis are shown in Figure 21.3. The condition may be due to:
 Loss of hydrogen ion in gastric fluid during vomiting. This is especially seen when there is pyloric stenosis preventing parallel loss of bicarbonate-rich secretions from the duodenum.
Loss of hydrogen ion in gastric fluid during vomiting. This is especially seen when there is pyloric stenosis preventing parallel loss of bicarbonate-rich secretions from the duodenum.


 Clinical note
Clinical note






