Chapter 52 Mesotherapy for body contouring and cellulite
• Mesotherapy is a specialty that is practiced worldwide by over 18 000 physicians for cosmetic applications such as cellulite, spot weight reduction and facial rejuvenation.
• Mesotherapy uses combinations of homeopathic and pharmaceutical medications as opposed to injection lipolysis, which uses a single substance.
• Patient selection is key for success.
• Medication used must be isotonic, biocompatible and sterile, with a pH between 5 and 7.
• Number of treatments is determined by patient’s severity of symptoms and how they respond to therapy.
• Absence of double-blind studies has caused the United States medical community to be slow in its acceptance.
Introduction
Mesotherapy is a nonsurgical cosmetic treatment invented by Michael Pistor in France in 1952 after he completed research in intradermal therapy and research in treating disorders in the mesoderm layer.1 By choosing mesotherapy, the patient is not subjected to oral or intravenous medication, as it treats the problem at its source by local action. The French Academy of Medicine recognized mesotherapy as a specialty of medicine in 1987. The International Society of Mesotherapy has members in 14 countries throughout Europe and South America. Over the past 50 years, in excess of 18 000 physicians worldwide have used mesotherapy on a daily basis for a variety of purposes, including treatment of cellulite, spot weight reduction, overall weight loss, hair loss, facial rejuvenation, correction of liposuction errors, pain management, and sports injuries. This chapter will only deal with the cosmetic applications of mesotherapy for body contouring and cellulite.2
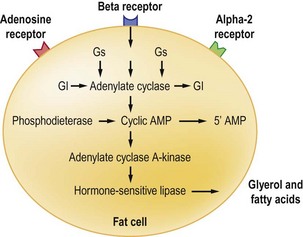
Mesotherapy employs multiple injections of a combination of homeopathic and pharmaceutical medication, plant extracts and vitamins that are injected into the mesoderm layer targeting the adipose fat cells, dermal vasculature, and connective tissue septae. The medications selected for use are based on the intent of the treatment. Injection lipolysis (Fig. 52.1) using a single substance like Lipodissolve™ should not be confused with mesotherapy that uses combinations of medications.3 The injections are performed with a special needle that varies from 0.4 to 0.6 cm, spaced approximately 1.5–2.5 cm apart. Sometimes the technique of Nappage is used; this is a series of injections of small amounts of substance into superficial concentrated areas of the skin with a longer needle up to 13 mm used occasionally to target deeper fat.3
Mesotherapy has spurred some controversy in the American medical community even though it has been very well accepted in Europe and South America.4 Unlike recognized FDA-approved cosmetic procedures, the medications used are off-label and no double-blind studies have been completed to support mesotherapy as an effective nonsurgical alternative to liposuction. Success rates vary on the formulas used, and most users keep their formula proprietary. It is safe to say that mesotherapy should only be utilized by practitioners that are licensed to use injectable medications, and have studied the techniques and complications of the procedure.5
Selection of Patients for Mesotherapy
Cellulite can also be treated with mesotherapy. Cellulite refers to the appearance of dimpled skin referred to as “orange peel”, on the thighs, buttocks, and sometimes lower abdomen of otherwise healthy patients; 90% of cellulite cases occur in women.6 Cellulite is most common in areas of fat deposits and is the result of the unevenness of this fatty tissue beneath the skin surface. Since cellulite is largely due to a structural aberration below the skin, people who have more fat deposits have more pronounced cellulite. Most structural changes include vertical orientation of the septae with increased septal thickness, while those with less fat and more muscular definition tend to have less visible cellulite. There is still much controversy over the etiology and pathology of cellulite. Most theories postulate this condition with abnormal connective tissue organization, alterations in fat metabolism, microcirculatory/lymphatic derangements, and venous insufficiency.7
According to studies conducted using magnetic resonance imaging and sonography,8 female fat lobules are larger than males’ and compartmentalized by fibrous septae that form radial and archlike structures. The uppermost layer of subcutaneous fat has been described as “standing fat-cell chambers” separated by connective tissue. From these fat-cell chambers, small projections of fat cells protrude into the dermis. This unevenness and irregularity of the subcutaneous fat give the skin the appearance we call cellulite.
Mesotherapy treatments for cellulite attempt to improve these four pathological aspects. Medications are selected to improve lymphatic and venous drainage, improve the connective tissue characteristics, and reduce adipose deposits that result in the dimpled look of the skin.9 Although fat reduction is important in the treatment, usually the appearance is of most concern to the patient, rather than a size change of the area.
Patients should be given full counseling on adding exercise and nutritionally sound diets to their daily routines if they are not already adhering to them. Alcohol consumption should be at a minimum, as should UV exposure for suntanning. Sun burn, concurrent skin treatments in the area, or skin infection will contraindicate treatments. Patients should not expose their skin to tanning, jacuzzis or steam following their treatments. Hot showers or baths should also be avoided for 48 hours. Exercise also should be avoided for 8 hours if excessive sweating occurs (Table 52.1).10
| Liposuction | Mesotherapy |
| Surgical procedure | Noninvasive procedure |
| Removes fat cells | Removes fat from fat cells |
| Cannot be used where there is cellulite | Used wherever there is cellulite |
| Down time (2 weeks) | No down time |
| Wear restrictive garments afterwards for weeks | Wear loose clothing after treatment |
| Weight gain back in abnormal places | Weight gain back where it was lost |
| Significant bruising & pain | Minimal bruising and pain |
| Causes divots and scarring | Reduces divots and scarring |
| Takes up to 3 months to see results | Results seen in weeks |
| Causes loose and weak skin | Tightens and strengthens skin |
Formulations
The selection of medications, herbal extracts and vitamins is generally at the discretion of the practitioner, and is learned in a course on mesotherapy. It is important to choose medication based on the reason for the treatment (Fig. 52.2). The formula for each patient will differ and medications and volume of each “cocktail” will vary from one body region to another and may change each time. Treatment for fat alone will utilize medication for lipolysis, vasodilation and perfusion, while treatments for cellulite will also include dissolution of septae and banding. Sometimes multiple medications will be used together that cause lipolysis, because they have different physiological actions. All mesotherapy mixtures must adhere to ensure patient safety. The medications used must be isotonic, biocompatible and sterile, with pH between 5 and 7. In Europe, theophylline tends to be the drug of choice for lipolysis, whereas in the Americas it is usually phosphotidylcholine.11 Usually 20–30 ml of formula are injected in each session, with the formula varying in each syringe if necessary.
Injections
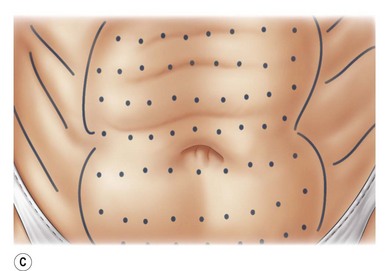
Techniques of mesotherapy injections include proper spacing with a grid-like pattern between injections 1.5 cm apart. When the face is injected, the spacing falls to 1 cm between injections. A 0.6 cm needle is used to create skin retractions and care must be taken to avoid injecting into the musculature. The area is first cleaned with alcohol, and the area to be treated is marked in a grid-like pattern. With mesotherapy “cocktails”, approximately 0.1 ml is injected into every site, so that the medication can spread evenly in the treated area. This differs significantly from fat lipolysis using only mixtures of phosphatidylcholine/deoxycholate, where up to 0.5 ml are injected into individual areas treated.12
Side Effects and Treatment
Patients may develop an allergic reaction, such as wheal and flare in response to one of the components of the medication. Patch testing should be done 1 week after the reaction has occurred. Usually this will respond to Benadryl and topical cortisone cream; however, if the reaction persists or becomes painful, a Medrol Dosepack should be prescribed.13
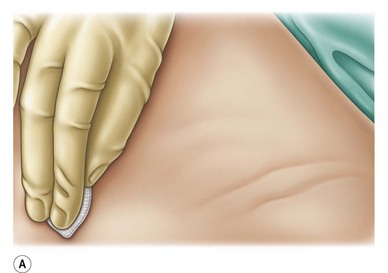
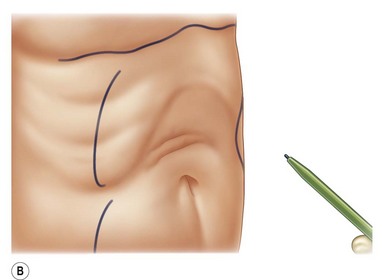
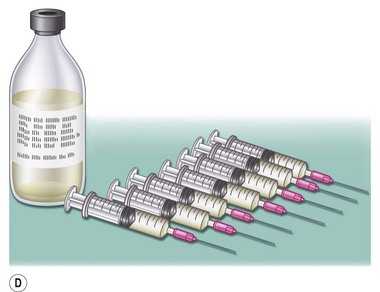
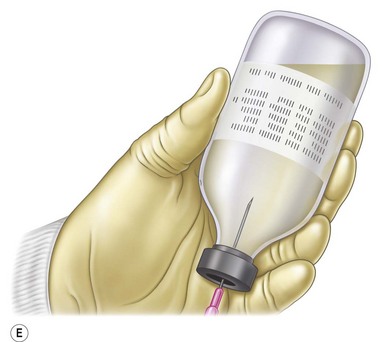
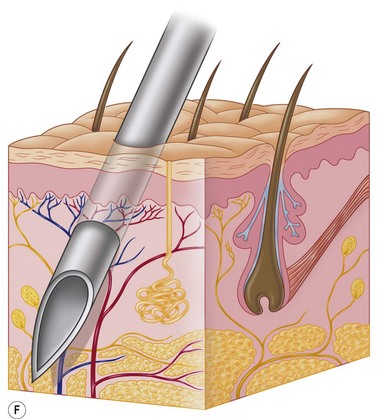
Other adverse reactions reported are cutaneous granulomas, atypical mycobacterial infections, lichenoid eruptions, ulcerations and exacerbation of psoriasis. To avoid these complications, patients need to choose physicians who have been trained in mesotherapy and perform it under sterile conditions with properly formulated sterile components14 (Fig. 52.3A–D).




Conclusion
Although mesotherapy has attracted wide acceptance in the medical community in Europe and South America, the absence of double-blind studies has caused the United States medical community to be slow in its acceptance of mesotherapy. Nonetheless, those practitioners of it who have been properly trained have consistently observed highly successful results in their patients (Fig. 52.4A–J). As a result, various pharmaceutical companies have recently conducted trials using mesotherapy medications with an expectation that FDA approval will be obtained and the medical community will be more likely to perform research on and practice mesotherapy.










1 Pistor M. What is mesotherapy? Chir Dent Fr. 1976;46:59–60.
2 LeCoz J. Traite de mesoterapie. Paris: Masson; 2004. p. 7–9
3 Rotunda AM. Mesotherapy and phosphatidylcholine injections: historical clarification and review. Dermatol Surg. 2006;23:465–480.
5 Rotunda AM. Cellulite: Is there a role for injectables? J Cosmet Laser Surg. 2005;7:147–154.
6 Kligman AM. Cellulite: facts and fiction. J Geriatr Dermatol. 1997;5:136–139.
7 Rosenbaum M, Prieto V, Hellmer J, et al. An exploratory investigation of the morphology and biochemistry of cellulite. Plast Reconstr Surg. 1998;101:1934–1939.
8 Rossi ABR, Vergnanini A. Cellulite: a review. J Eur Acad Dermatol Venereol. 2000;108:51–58.
9 Curri SB. Cellulite and fatty tissue microcirculation. Cosmet Toilet. 1993;108:51–58.
11 Rittes PG. The use of phosphatidylcholine for correction of local fat deposits. Aesth Surg J. 2003;27:315–318.
12 Duncan DI. Fat reduction using phosphatidylcholine/sodium deoxycholate injections: standard of practice. Aesthetic Plast Surg. 2008;32:858–872.
13 Urbani C. Urticarial reaction to ethynediamine in aminophylline following mesotherapy. Contact Derm. 1994;31:198–199.
14 Gokdemir G. Cutaneous granulomatous reaction from mesotherapy. Dermatolog Surg. 2009;35:291–293.






