CHAPTER 2 Meningeal Anatomy
THE MENINGEAL COVERINGS
The brain and spinal cord are covered by layers of connective tissue called meninges, from the Greek word meninx, which means membrane. In fishes, only a single layer, the primitive meninx, is present. Amphibians and reptiles have two meningeal layers, the outer dura mater (meaning “hard mother”) and an inner, thin layer the secondary meninx. In mammals and birds, three meningeal layers are present. The pia mater (meaning “tender mother”) is thin, vascular, and closest to the brain. The arachnoid membrane, which has a spider web–like appearance, is the middle, avascular layer. The space between the pia mater and arachnoid is the subarachnoid space. The outermost layer is the dura mater, composed of two layers. Therefore, the meningeal coverings consist of three membranous layers, composed primarily of fibroblasts, varying amounts of extracellular connective tissue and one well-organized fluid-containing space. The membranes are the dura mater (pachymeninx) and the leptomeninges (arachnoid and pia mater). The use of the word mater (“mother”) to describe these membranes comes from the ancient notion that they were the origin, or mother, of all membranes in the body.1
THE LEPTOMENINGES
Leptomeninx is the term used when the pia mater and arachnoid are considered together as a functional unit and contraposed to pachymeninx (from the Greek packys, meaning thick), designates the finer meningeal coverings.2
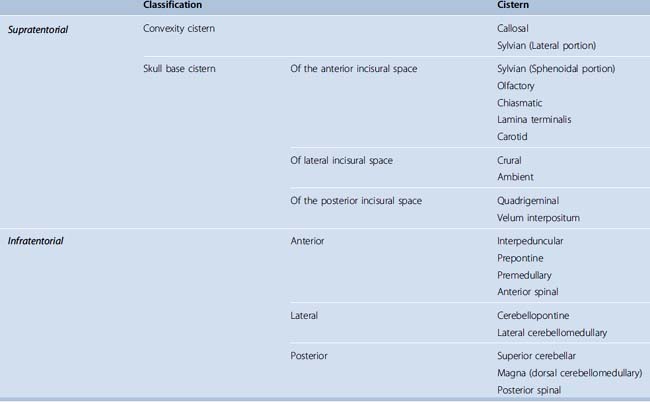
The arachnoid is attached to the overlying dura mater. It consists of several layers of translucent cells that follow with the dura and a contingent of cells that form spindly trabeculae that bridge the subjacent space and attach to the pia mater on the surface of the brain. The subarachnoid space is bordered outside by the layer of arachnoid cells attached to the dura and on the inside by pial cells on the surface of the neural tissue. These structural relationships form the basis for the occurrence of the subarachnoid cisterns, which are dilations of the subarachnoid space containing arteries, veins, and neural structures (see Table 2-1 later).
GENERAL STRUCTURE OF THE DURA MATER: ENDOSTEAL AND MENINGEAL LAYERS
The dura is composed of an endosteal layer that faces the bone and a meningeal layer that faces the brain.3 These layers are distinguished as separate sheaths at the venous sinuses, foramen magnum, and optic canal. The meningeal layer is continuous with the dural covering of the spinal cord and optic nerves, providing tubular sheaths for the cranial nerves as they pass through the cranial foramina. These sheaths fuse with the epineurium as the cranial nerves emerge from the skull, except at the optic nerve, where the dural sheath blends into the sclera. At the vascular foramina, the meningeal layer fuses with the adventitia of the vessel. The meningeal layer folds inwards to form the falx cerebri, the tentorium cerebelli, the falx cerebelli, and the diaphragm sellae, which partially divide the cranial cavity into freely communicating spaces. The endosteal layer of dura is continuous through the cranial sutures and foramina with the pericranium and through the superior orbital fissure and optic canal with the periorbita.3
The walls of the cavernous sinus are formed by the dura lining the internal surface of the calvaria. In the lateral portion of the middle cranial fossa, the meningeal and endosteal layers are tightly adherent, but at the lateral aspect of the trigeminal nerve they are separated into two layers. At the upper border of the maxillary nerve, which is the most inferior limit of the cavernous sinus, the meningeal layer extends upward to form the outer part of the lateral wall of the cavernous sinus, and it wraps around the anterior petroclinoid fold, extending medially to form the roof of the cavernous sinus and the upper layer of the diaphragm sellae. The endosteal layer, at the upper border of the maxillary nerve and the lower margin of the carotid sulcus, divides into two layers. One layer adheres to the sphenoid bone, covering the carotid sulcus and the floor of the sella, and the other layer extends upward to constitute the internal layer of the lateral wall and roof of the cavernous sinus and diaphragm sellae. The endosteal layer invests the cranial nerves coursing in the lateral wall of the cavernous sinus. The thin layer in the sellar part of the medial wall of the cavernous sinus is thought to represent a continuation of the meningeal dural layer that faces the brain. Thus, two layers line the sellar floor and the lower surface of the pituitary gland, one that is adherent to the sphenoid bone and the other that comes from the diaphragm and wraps around the pituitary gland. Therefore, with the exception of the paired lateral aspects of the sella and pituitary gland that are covered by one layer, two layers cover the other sellar surfaces. The meningeal and endosteal layers of the lateral wall and cavernous sinus roof and diaphragm sellae continue anteriorly to line the anterior cranial fossa and posteriorly as the covering of the dorsum sellae and clivus. The meningeal layer also continues anteriorly to form the upper (distal) dural ring around the carotid artery and the optic sheath, whereas the endosteal layer continues anteriorly and medially to form the lower (proximal) dural ring around the carotid artery.4
VASCULAR ORGANIZATION OF DURA
The origin of the membranes of the skull starts when the embryo has a crown-to-rump length of 12 to 20 mm, at which time differentiation of the skull, dura mater, arachnoid, and pial membranes begins. The gradual cleavage of the vascular system into external, dural, and cerebral layers also takes place at this stage, which has been referred to as the third stage of cerebrovascular development.5 As the membranes covering the brain differentiate, the anastomosing channels that connect the deep capillary plexus with the superficial vessels close, thus separating the vessels surrounding the brain from those belonging to the skull and its coverings.5,6 The major meningeal arteries originating from this cleavage give rise to a rich anastomotic network that may enlarge after various insults7 and play a role in the genesis of dural arteriovenous malformations. This anastomotic network divides progressively into primary, secondary, and penetrating vessels.
The primary anastomotic vessels change little in diameter as they course over the dural surface and anastomose frequently with each other. They cross the superior sagittal sinus, connecting the dura over the paired cerebral hemispheres into a single vascular unit. Crossing vessels are particularly large when one middle meningeal artery is hypoplastic. The primary anastomotic arteries have a straight course and measure 100 to 300 μm in diameter, whereas the main meningeal feeders have a diameter of 400 to 800 μm. The primary anastomotic arteries give rise to arteries to the skull, secondary anastomotic arteries, penetrating dural vessels, and arteriovenous shunts.8
Secondary anastomotic arteries also lie on the outer dural surface. They measure 20 to 40 microns in diameter, are short, and their anastomotic pattern form a regular polygonal network.8 Penetrating vessels arise from primary and secondary anastomotic arteries, leave the dural surface and extend to within 5 to 15 μm of inner and juxta-arachnoid surface of dura, to end in the capillary network. Capillaries, 8 to 12 μm in diameter, are present throughout dura, including the falx and tentorium, and are especially rich parasagittally, where they may form several layers. The capillary bed is located on the inner or cerebral surface of dura and is separated from arachnoid by only a few microns.8
Overview of Dural Supply
The dural arteries arise from the internal and external carotid, vertebral, and basilar arteries (Table 2-1) and may be the site of formation of saccular aneurysms, pseudoaneurysms, and arteriovenous fistulas and the source of traumatic and spontaneous hemorrhage into the epidural, subdural, and intraparenchymal area, in addition to the well known role in the vascularization of meningiomas, other tumors, and parenchymal arteriovenous malformations (AVMs).
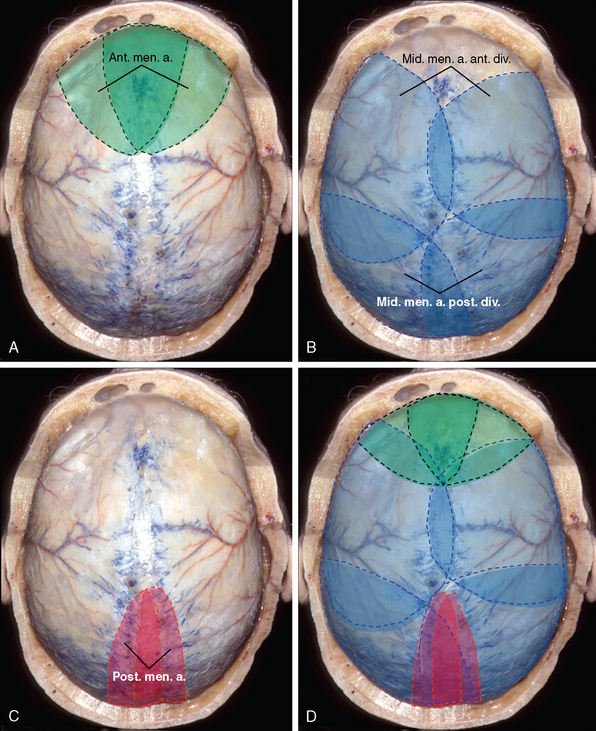
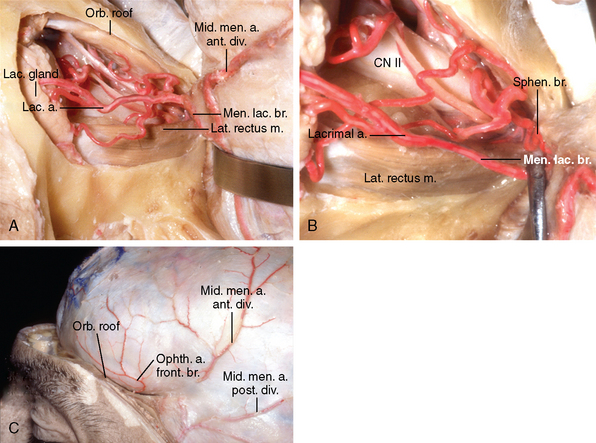
The dura covering the anterior fossa floor draws its supply from the anterior and posterior ethmoidal arteries, the superficial recurrent ophthalmic artery, and the middle meningeal artery (Fig. 2-1). The middle meningeal artery will not contribute to the supply of the dura lining the floor of anterior fossa if the artery or its anterior branch arises from the ophthalmic arterial system. The territory of the anterior convexity and parasagittal area is supplied by both the anterior branch of the middle meningeal artery and the anterior meningeal branch from the ophthalmic artery (Fig. 2-2).
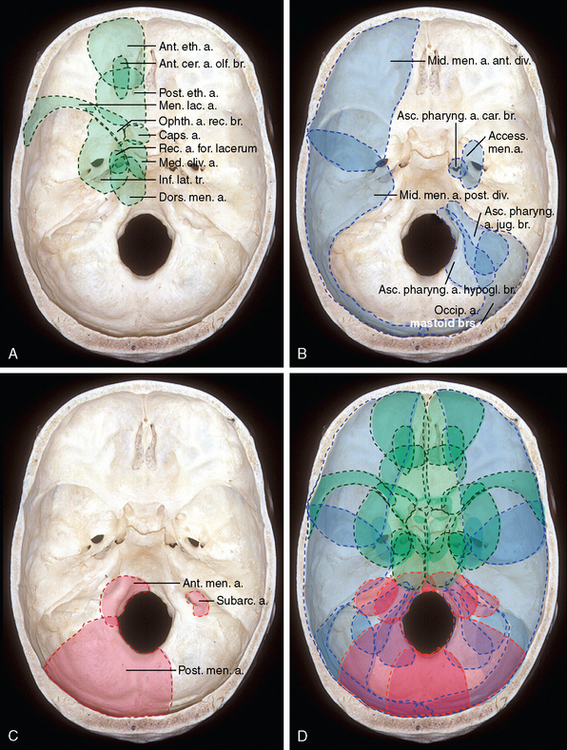
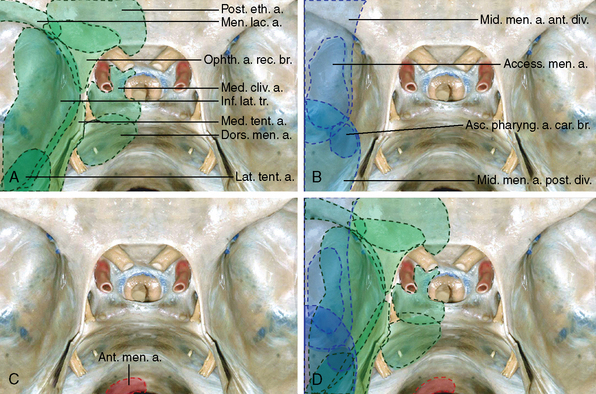
The supply to middle fossa and paracavernous dura derives laterally from the middle meningeal, accessory meningeal, and ascending pharyngeal arteries. In an anterior to posterior direction, it receives contributions from the recurrent branches of the ophthalmic and lacrimal arteries, as well as from the medial tentorial artery (Figs. 2-1 and 2-3). Medially those arteries anastomose with the cavernous branches of the internal carotid artery. In this system, dominance of a particular vessel can lead to unusual anatomic variants. The sellar dura has a bilateral supply from the paired capsular, inferior hypophyseal, medial clival, and dorsal meningeal arteries that anastomose across the midline in front and behind the dorsum sellae9,10 (Figs. 2-1, 2-3, and 2-4). The inferior hypophyseal artery can supply pituitary adenomas and tumors of the sphenoid sinus.11–13
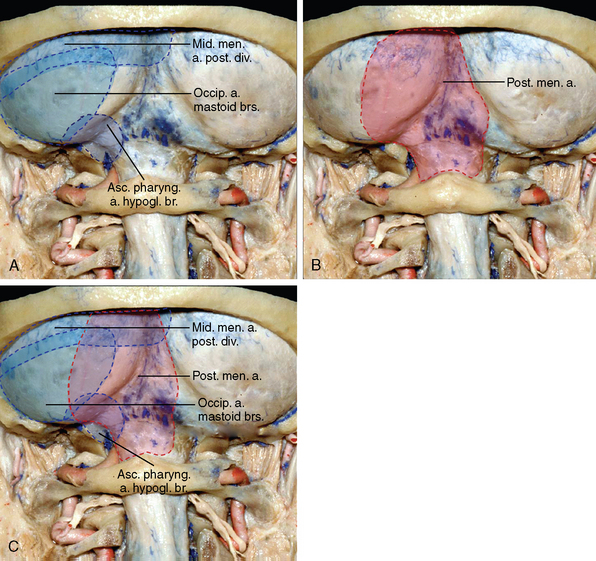
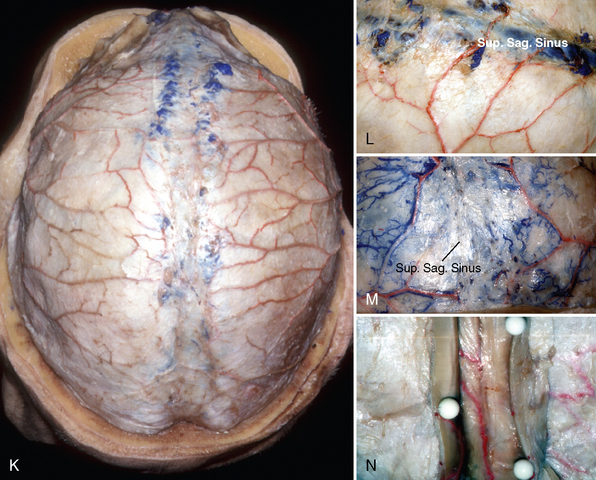
The convexity dura is supplied predominantly by branches of the middle meningeal arteries. These branches course toward the superior sagittal sinus, where they are distributed to the sinus walls and give off descending branches to the adjacent falx cerebri. The scalp arteries, through the emissary foramina, also send branches to the convexity dura. The dura over the frontal convexity is supplied by the anterior meningeal branch of the anterior ethmoidal artery and branches of the anterior division of the middle meningeal artery that also distributes to the dura in the anterior parietal region. The dura over the posterior convexity is supplied by the parieto-occipital an petrosquamosal branches of the posterior division of the middle meningeal artery.9,10 This area also receives a contribution from the posterior meningeal branch of the vertebral artery, when this vessel extends above the torcular14 (see Fig. 2-2).
The falx cerebri, falx cerebelli, and tentorium are supplied by basal and convexity branches of the meningeal arteries and receive a contribution from the cerebral arteries, making these structures an anastomotic pathway between dural and parenchymal arteries. Most of the vascular supply of the falx cerebri comes through its insertion on the vault, with the anterior basal insertion, the falcotentorial angle, and the free margin receiving independent contributions15 (Figs. 2-3 and 2-5). The dural walls of the superior sagittal sinus, the site of insertion of the falx on the dura of the convexity, are supplied by the middle meningeal arteries, which form two paramedial arcades, and are reinforced anteriorly, at the level of the insertion of the falx on the crista galli, by the anterior falcine arteries (see Fig. 2-5).
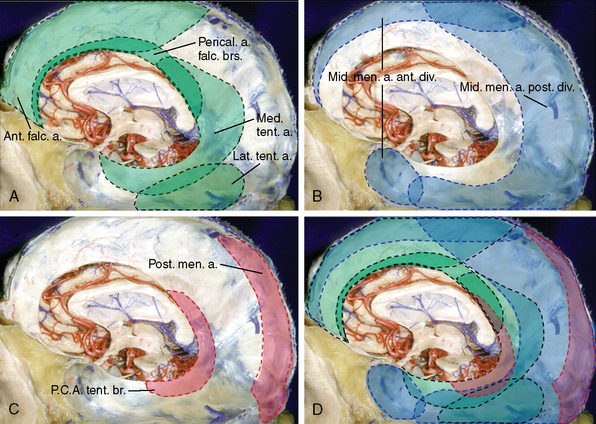
Posteriorly, at the falcotentorial junction, the paramedial arcades are reinforced from three sources: the posterior meningeal artery from the vertebral artery, medial tentorial artery from the cavernous carotid, and an occasional branch of the posterior cerebral artery. The posterior meningeal artery, the major contributor, extends along the insertion of the falx cerebri after coursing into the insertion of the falx cerebelli. The medial tentorial artery, which supplies the medial third of the tentorium, reaches the straight sinus and torcular and may ascend in the posterior portion of the falx cerebri9,10 (see Fig. 2-5). The pericallosal branches of the anterior cerebral artery may also pierce the falx at or near its free edge to reinforce the arterial network along the deep edge of the falx.
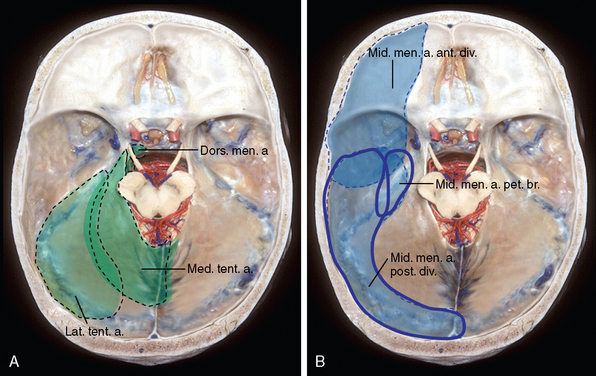
The tentorium receives supratentorial and infratentorial contributions (Figs. 2-3, 2-5, 2-6). The supratentorial sources are the marginal and lateral tentorial branches of the cavernous carotid medially and the branches of the middle meningeal artery anterolaterally. The infratentorial components are the superior extensions of the jugular branch of the ascending pharyngeal artery and the tentorial branch of the posterior cerebral artery medially, the occipital artery laterally, and the posterior meningeal artery posteriorly (see Fig. 2-3). The lateral two thirds of the tentorium and its edge along the transverse sinus derive their supply mainly from two arterial arcades, petrosal and occipital. The petrosal arcade follows the superior petrosal sinus and is composed of the lateral tentorial artery, branches from the petrous and petrosquamosal trunk of the middle meningeal artery, and the lateral branch of the dorsal meningeal artery. The occipital arcade is composed above the tentorium by the petrosquamosal trunk and occipital branchs of the middle meningeal artery, and the occipital and posterior meningeal arteries form its infratentorial limb9,10 (see Fig. 2-6). The medial third of the tentorium is supplied by the medial tentorial artery from the internal carotid artery. This artery may receive a contribution from the posterior cerebral artery through the artery of Davidoff and Schechter (see Figs. 2-3 and 2-6).
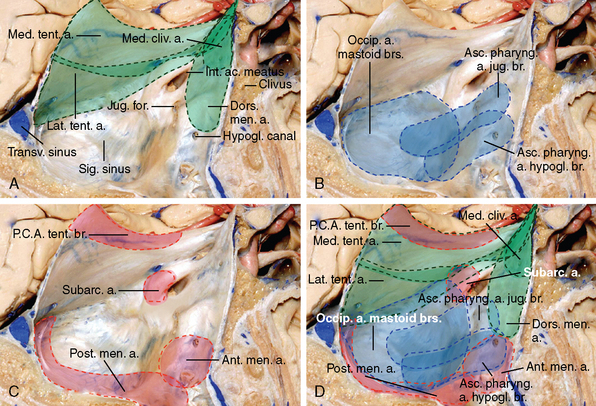
The clival area derives its supply from the medial clival and dorsal meningeal, branches of the internal carotid artery, the anterior meningeal branch of the vertebral artery, and branches of the ascending pharyngeal artery. The dura over the posterior surface of the petrous bone is supplied by the dorsal meningeal and subarcuate arteries and branches of the middle meningeal, occipital, and ascending pharyngeal arteries (see Figs. 2-1 and 2-6). The dura of the lateral portion of the cerebellar fossa receives its supply from the ascending pharyngeal, occipital, and vertebral arteries. The posterior meningeal artery is the major supplier of the paramedial and medial portions of the cerebellar dura, but this area also receives contributions from the middle meningeal and occipital branches to the region of the torcular (Fig. 2-7).
In this discussion, the dura of the posterior fossa has been subdivided into several areas. The clival dura extends from the dorsum sellae to the anterior border of foramen magnum and is limited laterally by the petroclival fissure. The posterior petrous dura extends from the petroclival fissure to the sigmoid and superior petrosal sinuses. The cerebellar fossa dura is limited laterally by the sigmoid sinuses and extends over the cerebellar surface from the transverse sinus to the foramen magnum. The dura on each side of the midline has been further subdivided into a medial region, adjacent to the falx cerebelli; a lateral region, adjacent to the sigmoid sinus; and a paramedial region between the two. At the level of the foramen magnum, the dural supply arises predominantly from the external carotid and vertebral arteries16 (see Fig. 2-6). The anterior and posterior meningeal arteries, branches of the vertebral artery, anastomose with the jugular and hypoglossal branches of the ascending pharyngeal artery and the mastoid branch of the occipital artery. The cavernous carotid may also contribute through the clival branches of the dorsal meningeal arteries.12 The dural branches of the vertebral artery are usually small but may enlarge to supply dura-based lesions. Enlargement of the anterior meningeal artery is seen with meningiomas, glomus jugulare tumors, recurrent hemangioblastomas, and metastatic tumors.17
Dural territories often have overlapping supply from several sources. A reciprocal relationship between the territories of adjacent arteries is common so that when the area supplied from one source is small another artery enlarges to supply the area. This reinforces the need to see all possible sources of supply to a lesion before any surgical or endovascular treatment. Areas supplied from several overlapping sources are the tentorium and adjacent falx, the walls of the cavernous sinus, and the dura around the gasserian ganglion.18
Dural Arteries
External carotid artery branches
Ascending pharyngeal artery
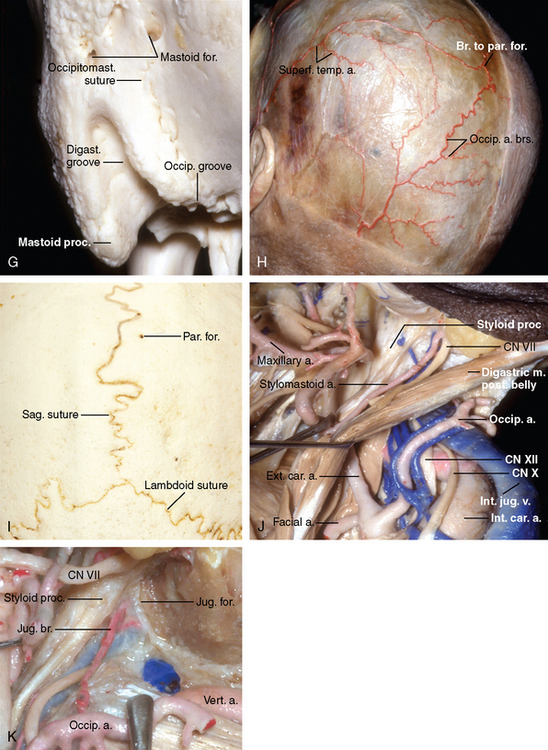
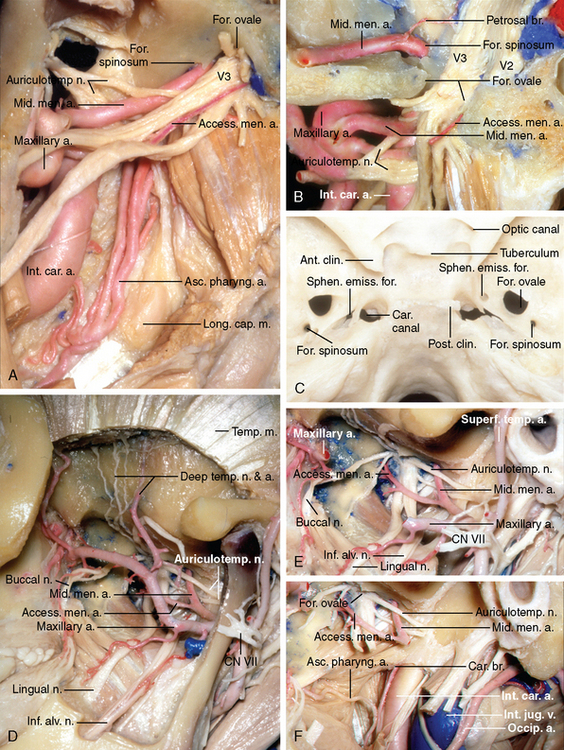
The ascending pharyngeal artery, the smallest branch of the external carotid artery, usually arises from the proximal portion of the external carotid artery. It has an ascending vertical course, along the posterolateral wall of pharynx, anterior to the longus capitis muscle, and medial to the styloglossus and stylopharyngeus muscles (Fig. 2-8A, B). This initial segment of the artery can be seen, in the lateral angiogram, in front of the vertebral column, and medial to the main external carotid trunk on the anteroposterior view.
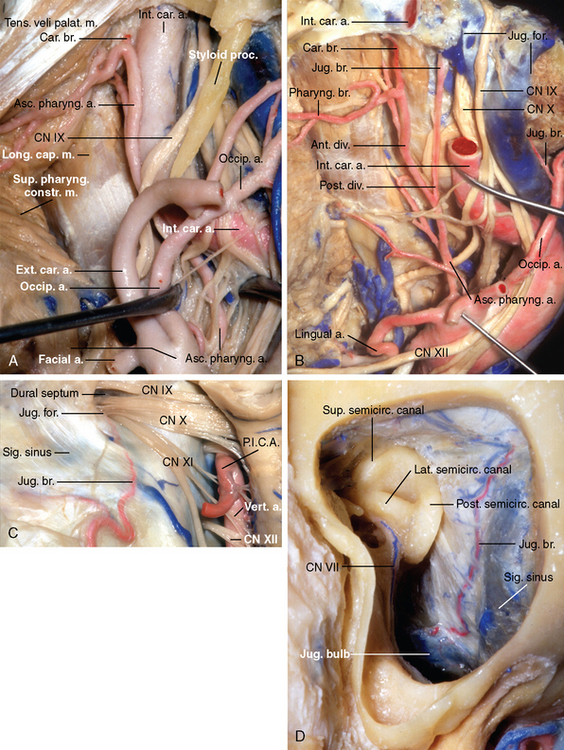
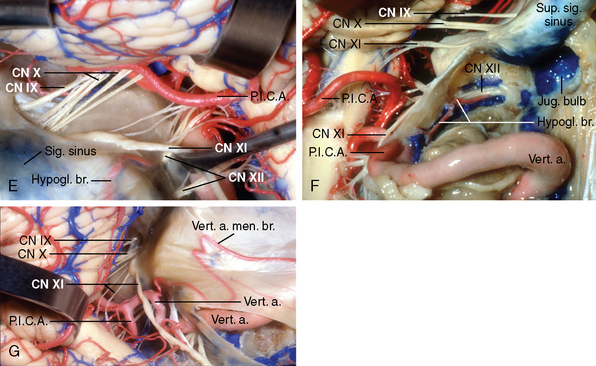
The meningeal contribution of the ascending pharyngeal artery is via three branches: hypoglossal, jugular, and carotid (see Fig. 2-8A). The hypoglossal and jugular branches, the more constant, originate from the posterior division,10 and the carotid branch from the anterior division (Fig. 2-8C–G). The hypoglossal branch accompanies the hypoglossal nerve and enters the skull through the hypoglossal (anterior condylar) canal, to be distributed to the dura surrounding the foramen magnum and clivus, where it anastomoses with the branches arising from the ipsilateral cavernous carotid and vertebral arteries, and its mate from the opposite side. The hypoglossal artery may also arise from the vertebral artery (see Fig. 2-8G). The area of supply of the hypoglossal branch (see Figs. 2-1, 2-6, and 2-7) may extend to the dura of the lateral portion of the cerebellar fossae, where it borders and has a reciprocal relationship with the territory supplied by the mastoid branch of the occipital artery and the posterior meningeal artery of the vertebral artery. In the clival area it may anastomose superiorly with the medial clival branch of the inferior hypophyseal artery and the dorsal meningeal artery and inferiorly with the anterior meningeal artery of the vertebral artery.9,10
The jugular branch enters the jugular foramen with cranial nerves IX, X, and XI, where it divides into medial and lateral branches. The lateral branch courses along the dural wall of the sigmoid sinus (see Fig. 2-8D), where it anastomoses with the jugular branch of the occipital artery (Fig. 2-9). The medial branch courses along and supplies the dura bordering the inferior petrosal sinus. Its territory (see Figs. 2-1, 2-6, and 2-7) borders the area supplied by the dorsal meningeal artery and medial clival artery from the cavernous carotid. Superiorly, it anastomoses with the subarcuate artery and the petrosquamosal branch of the middle meningeal artery and laterally with the mastoid branches of the occipital artery. The jugular branch distal to the jugular foramen supplies the dura facing the inferior part of the cerebellopontine angle9,10 (see Fig. 2-6). The hypoglossal and jugular branches also supply of the adjacent segments of cranial nerves IX through XII.10,19,20 On lateral angiograms, the posterior division of the ascending pharyngeal artery ascends besides and overlaps the foramen magnum. On anteroposterior views, the hypoglossal is the most medial of the terminal branches of the posterior division.
The carotid ramus originates from the anterior branch of the ascending pharyngeal artery. It courses in the periosteal lining of the carotid canal and anastomoses, at the level of the foramen lacerum, with branches arising from the carotid siphon9,10 to form the recurrent artery of the foramen lacerum. This recurrent artery also anastomoses at the lower edge of the trigeminal ganglion with the posterior branch of the inferolateral trunk and the cavernous branch of the middle meningeal artery. The carotid branch usually does not extend to the dura of clivus and cerebellopontine angle as do the other dural branches of the ascending pharyngeal artery.9,10 The recurrent artery of foramen lacerum may be involved in the supply of angiomas, lymphoid tumors, angiofibromas of the nasopharynx, and tumors of the cavernous sinus and caroticocavernous fistulas.9,10
Occipital artery
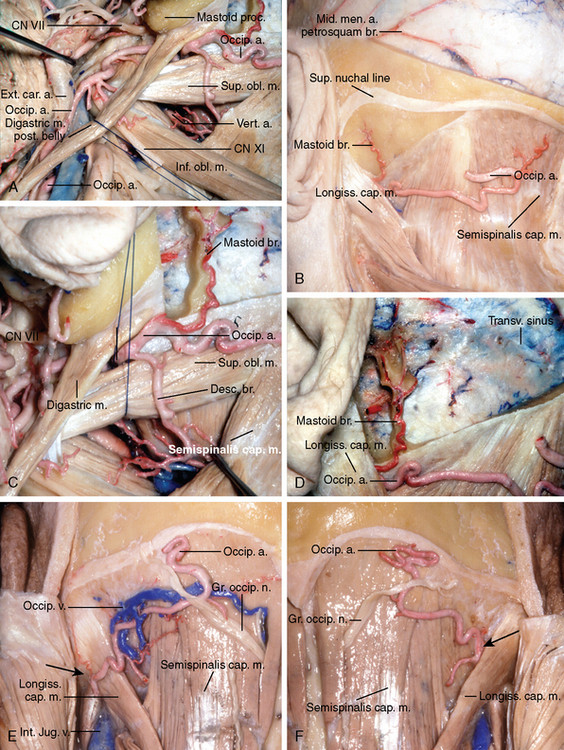
The occipital artery originates from the posterior surface of the external carotid artery, at the level of the angle of the mandible, and courses posteriorly and upward, being crossed superficially by the hypoglossal nerve. It passes deep to the posterior belly of the digastric muscle and lateral to the internal jugular vein, vagus nerve, internal carotid artery, and accessory nerve (see Fig. 2-9A). At the level of a vertical plane crossing the posterior border of the external auditory canal, the occipital artery can be found in a tunnel formed above by the occipital groove of the temporal bone—a prominent sulcus on the undersurface of the temporal bone, medial to the digastric groove—medially by the attachment of the superior oblique muscle on the transverse process of atlas, and laterally by the cranial insertion of the posterior belly of the digastric muscle in the digastric groove (see Fig. 2-9B–F). The presence of the occipital groove is dependent on whether the artery courses superficial or deep the longissimus capitis muscle. The groove is present if the artery courses deep to the longissimus capitis muscle along the lower surface of the skull base and is absent if the artery courses inferior to the skull base or lateral to the longissimus capitis muscle (see Fig. 2-9E–G).12
The occipital artery at the level of the posterior border of the upper insertion of the longissimus capitis muscle courses in the upper part of the space between the occipital bone and C1 and lateral to the rectus capitis posterior major and semispinalis capitis muscle. It is covered by a deeper layer formed by the splenius capitis muscle and a more superficial layer formed, from lateral to medial, by the sternocleidomastoid and trapezius. The occipital artery pierces the fascia between the trapezius and sternocleidomastoid, near the superior nuchal line and ascends in the superficial fascia of the scalp, where it is accompanied by the greater occipital nerve (see Fig. 2-9H).
The occipital artery gives rise to the auricular branch, which anastomoses with the posterior auricular artery behind the ear; the stylomastoid artery, muscular branches to the sternocleidomastoid, digastric, stylohyoid, splenius, and longissimus capitis muscles; and meningeal branches to the posterior fossa that enter the skull through the jugular foramen and condylar canal and to inconstant branches that runs through the mastoid foramen (see Fig. 2-9B, D, G).
The occipital artery is divided into three portions: (1) ascending cervical, (2) cervico-occipital or horizontal, and (3) ascending occipital21 (see Fig. 2-9A). The meningeal branches most frequently originate from the second and third arterial segments.
The mastoid branch, present in about one half of specimens21 (see Fig. 2-9B, D, G), also called the transmastoid branch or the artery of the mastoid foramen,3,9,10 originates from the second segment of occipital artery, at the level of the insertion of the semispinalis capitis muscle, midway between the inferior and superior nuchal lines. From its origin, the mastoid branch courses between the splenius capitis muscle and the junction of the mastoid and occipital bones. It enters the cranial cavity at the level of the superior nuchal line, by passing through the mastoid foramen. Intracranially, the superior nuchal line corresponds to the level of the transverse sinus. The mastoid branch emerges intracranially at the posterior border of the upper end of the sigmoid sinus and divides into three groups of branches: descending, ascending, and posteromedial.21 The descending branches are directed toward the jugular foramen and border the dural territory supplied by the jugular branch of the ascending pharyngeal artery (see Fig. 2-8D). The posteromedial branches anastomose with the petrosquamous branch of the middle meningeal artery and constitute the main supply to the lateral part of the cerebellar fossae that borders the territory of the hypoglossal branch of the ascending pharyngeal artery or the posterior meningeal branch of the vertebral artery, or both. The ascending branches, which are directed to the dura covering the superior part of the posterior surface of the temporal bone that faces the cerebellopontine angle, anastomoses with the subarcuate branch of the anterior inferior cerebellar artery (see Figs. 2-1 and 2-6), and can supply acoustic neurinomas, meningiomas, and arteriovenous fistulas. The mastoid branches also supply the endolymphatic duct and sac.22
The third or ascending occipital portion gives rise to the terminal branches of the occipital artery, which supply the musculocutaneous structures of the posterior portion of the cranial vault, and anastomoses with the branches of the superficial temporal artery (see Fig. 2-9H). The parietal foramen (see Fig. 2-9J), which is an inconstant opening located near the sagittal suture, about 3 to 5 cm in front of the lambda,3 transmits a meningeal branch of the ascending occipital segment and a small emissary vein.21
Maxillary artery
The maxillary artery, through its middle meningeal and accessory meningeal arteries (Figs. 2-10 and 2-11), provides almost all of the supply to the dura over the convexity and important contributions to the supply of the basal dura (see Figs. 2-1,2-3, and 2-4).
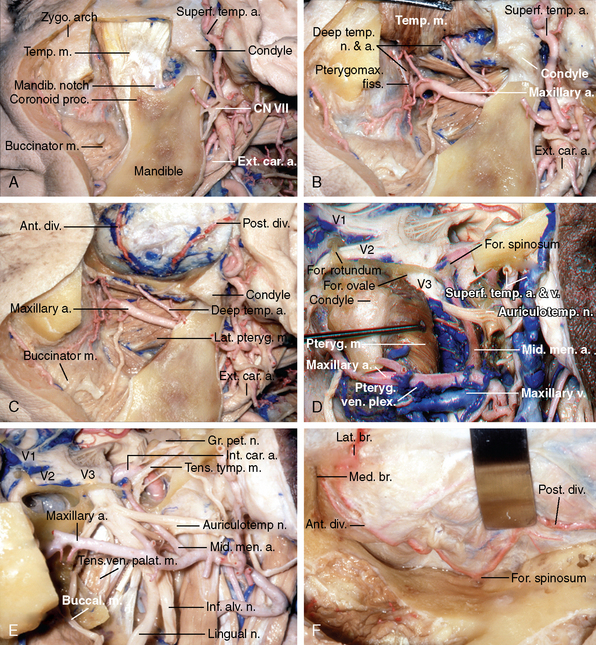
Middle meningeal artery
The middle meningeal artery normally arises from the first or mandibular segment of the maxillary artery, just behind the condylar process of the mandible, and enters the skull through the foramen spinosum (see Fig. 2-10A–H). After passing through the foramen spinosum, the main stem courses laterally, grooving the greater sphenoid wing, where it divides in its anterior and posterior divisions, which supply the dura of frontal, temporal, and parietal convexity; the upper surface of the temporal bone; and the adjacent walls of the transverse and sigmoid sinus as well as the middle fossa dura adjacent to the cavernous sinus (see Fig. 2-10F–N). In its path between the anterosuperior angle of the greater sphenoid wing and the sphenoid angle of the parietal bone, the anterior division, and sometimes the sphenoparietal sinus, can be encased in a bony canal that varies in extension from 1 to greater than 30 mm.23 The anterior division is usually single but may be composed of two branches (duplicated) in 0.8%, or absent in 0.7% of cases, while the posterior division is duplicated in 8.1%.23 At the level of the superior sagittal sinus the middle meningeal artery anastomoses with the anterior falcine branch of the ophthalmic artery to supply the dural layers of the falx (see Fig. 2-5).
The middle meningeal artery, and the osseous groove in which it courses, begins at the foramen spinosum and divide into anterior and posterior divisions 15 to 30 mm anterolateral to foramen spinosum (see Fig. 2-10F–I). The anterior division and its groove divide behind the lateral part of the greater wing into a lateral branch, which passes across the pterion to reach the dura of the lateral convexity, and a medial branch, which courses medially along the lower surface of the sphenoid ridge where it anastomoses with the recurrent branch of the lacrimal artery. In 9 out of 10 orbits dissected, Liu and Rhoton24 reported the presence of anastomotic connections between the recurrent meningeal branch of the lacrimal artery and the medial branch of the anterior division of the middle meningeal artery. Occasionally, the recurrent meningeal branch of the lacrimal artery gives rise to the anterior segment of the middle meningeal artery or more rarely, the ophthalmic artery can give rise to the main stem of the middle meningeal artery itself. In these cases, with an ophthalmic or lacrimal origin of the middle meningeal artery, the grooves marking the course of the main stem of the middle meningeal artery will originate at the lateral edge of the superior orbital fissure25 and the foramen spinosum will be hypoplastic or absent.26 Another, less frequent, site of origin of the middle meningeal artery is from the petrous portion of the internal carotid artery, referred to as a stapedial-middle meningeal artery, an anomaly that results from failure of the embryonic stapedial branch of the internal carotid artery to regress and allow the middle meningeal artery to become connected to the external carotid artery.26
Angiographically, in the anterior view, the middle meningeal artery is easily recognized by a sharp turn along the floor of the middle fossa after passing through the foramen spinosum. Its course along the inner table is characterized by smooth curves, in contrast with the sinuous course of the overlapping superficial temporal artery. This initial intracranial portion of the middle meningeal artery can be elevated and stretched by lesions arising at the skull base (see Fig. 2-5B). Radiographically, the grooves for the meningeal branches can become tortuous and the foramen spinosum can enlarge in meningiomas and vascular malformations.27,28
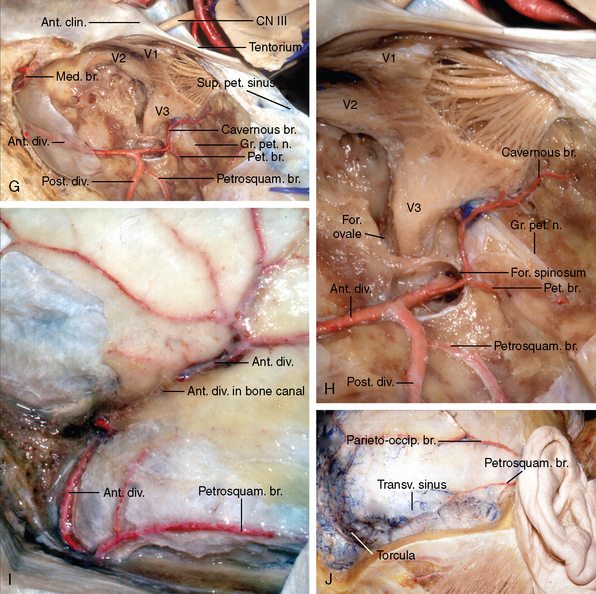
Immediately adjacent to the foramen spinosum the middle meningeal artery gives off a short branch, which divides into the petrosal artery laterally and a branch to the trigeminal ganglion medially (see Fig. 2-10G, H). The trigeminal branch has been referred to as the cavernous branch of the middle meningeal artery. The petrosal branch runs with the greater petrosal nerve and penetrates the temporal bone by passing through the facial hiatus and supplies the facial nerve and walls of the tympanic cavity.29,30 Damage to the petrosal branch occurring as the dura is elevated in a subtemporal extradural approach to the trigeminal nerve, cavernous sinus, or internal acoustic meatus may result in a facial nerve deficit. Bleeding at this site should be controlled by a method other than coagulation in order to avoid damaging the facial nerve, which may be exposed in the floor of the middle fossa at the level of the hiatus fallopii.25,30
The posterior branch of the middle meningeal artery gives rise to the petrosquamosal branch at the junction of the skull base and convexity (see Fig. 2-10I, J). It supplies the insertion of the tentorium along the petrous ridge and groove for the transverse sinus; the dura of the torcular; and the junction of the sigmoid, transverse, and superior petrosal sinuses, and extends to the dura of the posterior fossa bordering the area supplied by the other branches of the external carotid artery31 (see Fig. 2-7). The petrosquamosal artery may infrequently supply almost all the posterior fossa dura, including the cerebellar fossa and tentorium cerebelli.31 The parieto-occipital branch of the middle meningeal artery supplies the dura over the posterior convexity (see Fig. 2-10J).
The middle meningeal artery in the middle fossa has anastomotic connections with the ophthalmic system and the meningeal branches of the cavernous carotid artery (see Fig. 2-1). The middle meningeal artery may contribute to the supply of the second and third trigeminal divisions in addition to the facial nerve.19 It may supply most of the tentorium when giving rise to a medial tentorial branch. The medial tentorial artery may arise from either the main divisions of the middle meningeal artery or from the accessory meningeal artery,31 described in the next section.
The middle meningeal artery may also anastomose with a branch of the basilar artery.32,33
Accessory meningeal artery
The accessory meningeal artery, also called the lesser or small meningeal artery34,35 (see Table 2-1), may arise from either the maxillary or middle meningeal artery depending on the relationship of the maxillary artery to the pterygoid muscles.10,34 It arises from the maxillary artery if the maxillary artery courses deep to the pterygoid muscles and from the middle meningeal artery if the maxillary artery passes superficial to the pterygoid muscle. In the cases in which the middle meningeal artery arises from the ophthalmic, internal carotid or basilar artery, the accessory meningeal artery will arise directly from the trunk of the maxillary artery.36 The caliber of the accessory middle meningeal artery is about one third to one half of the middle meningeal artery (see Fig. 2-11A, B, D–F) and in 30% to 45% of the cases it is formed by of multiple small arteries,34,35 especially if it arises from the maxillary artery.34
From its origin, the accessory meningeal artery courses toward the angle between the posterosuperior edge of the lateral pterygoid plate and the infratemporal surface of the sphenoid bone. It usually passes posterior to the inferior alveolar and lingual nerves34 (see Fig. 2-11A, E). In 78% of the cases, the accessory meningeal artery enters the cranium through the foramen ovale. In the remaining 22%, it passes through the emissary sphenoid foramen (foramen of Vesalius), an opening occasionally found 2 to 3 mm medial to the anterior edge of foramen ovale that also transmits an emissary vein linking the pterygoid plexus and the cavernous sinus34,36 (see Fig. 2-11C).
The extracranial segment of the accessory meningeal artery has anastomoses with the ascending pharyngeal artery and pterygopalatine arteries9,10,36 (see Fig. 2-11A, F). It supplies the membranous portion of the Eustachian tube and external acoustic meatus, the lateral pharyngeal wall and medial pterygoid muscle, the mandibular nerve below the foramen ovale, and sphenoid periosteum. It has been suggested that it be called the pterygomeningeal artery because the extracranial structures receive the predominance of its flow while the intracranial branch receives only 10%.36
The intracranial territory of the accessory meningeal artery includes the gasserian ganglion and adjacent middle fossa dura, where it anastomoses with the meningeal branches from the ophthalmic and middle meningeal arteries and the carotid siphon. The accessory meningeal artery has a reciprocal relationship with the inferolateral trunk of the internal carotid artery in the supply of the mandibular nerve and the dura adjacent to the cavernous sinus. It has prominent anastomoses with the posterolateral branch of the inferolateral trunk (see Fig. 2-1). Lasjaunias and Theron36 found that the accessory meningeal artery was small in 25% of the cases that it anastomoses with the inferolateral trunk of the cavernous carotid artery, had a size similar to the inferolateral trunk in 59%, and that it was the only supply to the cavernous sinus area in 16%. In the latter case, the diameter of this accessory meningeal artery approaches that of the middle meningeal artery.9,36 Occlusion of this artery during endovascular procedures may result in cranial nerve deficits because of its supply to the oculomotor, trochlear, trigeminal, abducens and facial nerves.10,36
Dilenge and Geraud35 found that the artery could be identified in lateral angiograms throughout its extracranial course in 60% of 100 selective angiographies, but was recognizable intracranially in only six cases because of its small size. It was more easily identified when it was part of an anastomotic network between the carotid siphon and the internal maxillary artery. On the anteroposterior angiographic view, the accessory meningeal artery slants medially, above the skull base, toward the cavernous sinus at the point of arborization of the inferolateral trunk. It may contribute to the vascular pedicle of meningiomas and schwannomas of the gasserian ganglion,35 and can be involved in paracavernous arteriovenous malformations.
Internal carotid artery branches
Cavernous segment
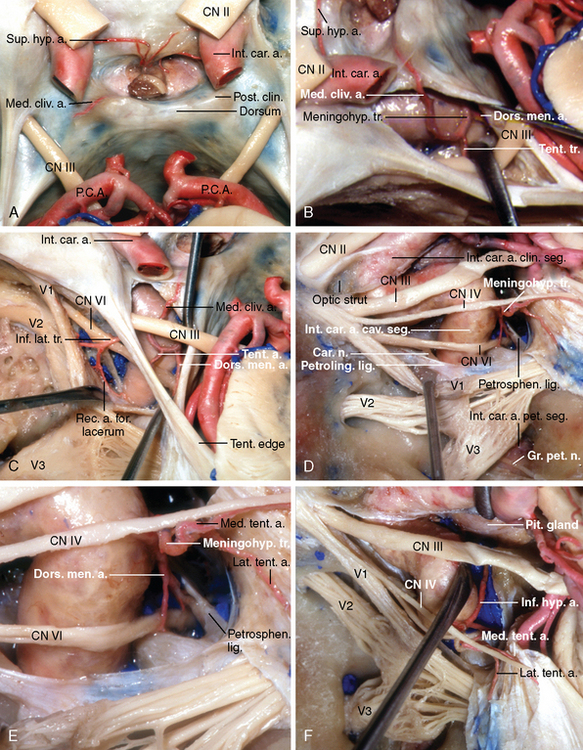
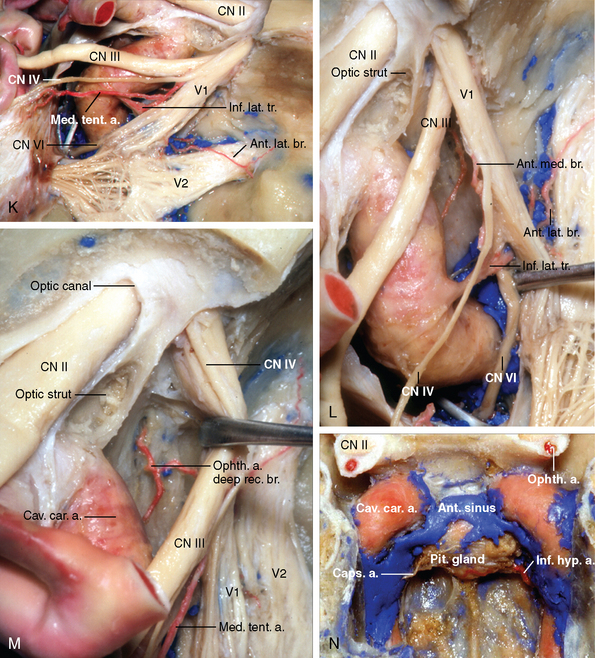
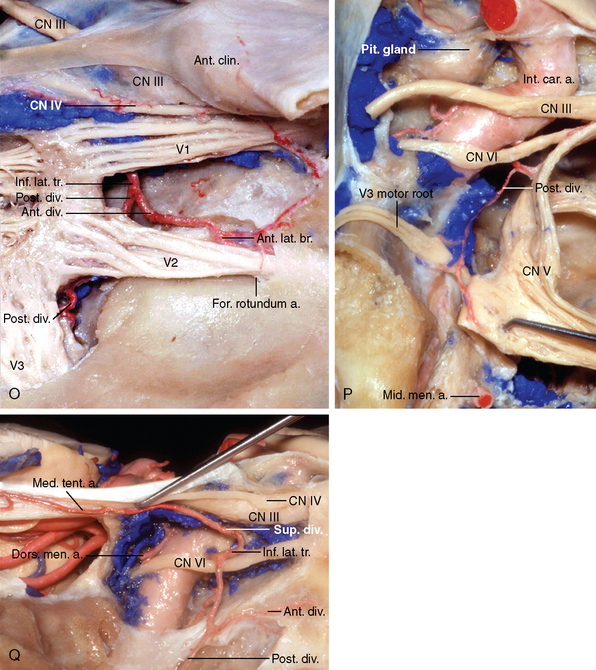
The cavernous portion of the internal carotid artery gives rise to branches that supply the walls and enclosed structures of sella, cavernous sinus, and the tentorium (see Figs. 2-3 and 2-4). The branches can be divided based on the direction of their course into a medial group that includes the inferior hypophyseal, medial clival, and capsular arteries; a lateral group that includes the inferolateral trunk, also called artery of the inferior cavernous sinus, and its branches and the lateral tentorial artery; and a posterior group that includes the dorsal meningeal artery and medial tentorial artery (Fig. 2-12A–L). The medial branches, including the inferior hypophyseal and medial clival artery, derive from the primitive maxillary artery, while the dorsal meningeal artery is the adult remnant of the primitive trigeminal artery. When these two embryonic vessels originate in a single trunk, the meningeal, hypophyseal, and neural branches will arise from a single source, referred to as the meningohypophyseal trunk.9,10
The meningohypophyseal trunk and the inferolateral trunk are the most consistent branches of the cavernous segment of the internal carotid artery. They arise from a single trunk in 6% of the cavernous sinus.37 These vessels anastomose with their mates of the opposite side and with the meningeal branches of the external carotid, ophthalmic, and vertebral arteries13 (see Figs. 2-1 and 2-4). The communication between the external carotid and internal carotid through the cavernous branches is of significance in the management of carotid cavernous fistulae, which must be based on evaluation of all these communicating channels. Increase in opacification of the cavernous carotid branches may occur with alteration of cerebral dynamics associated with increased intracranial pressure, a distant intracranial lesion, and in cerebrovascular disease in which the cavernous branches act as the rete mirabili.13
Meningohypophyseal trunk
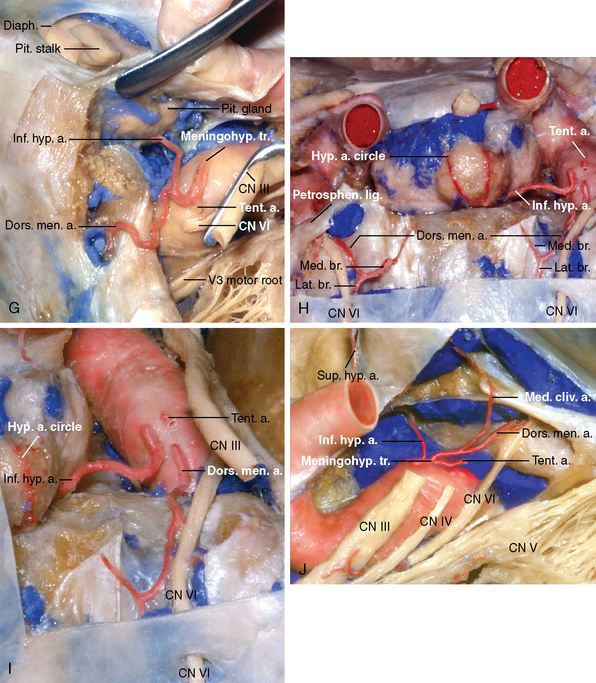
The meningohypophyseal trunk is the largest intracavernous branch of the internal carotid artery.38–40 It arises lateral to the dorsum sellae at or just proximal to the apex of the first curve of the intracavernous carotid (see Fig. 2-6). It is approximately the same size as the ophthalmic artery.38 In its most complete form it gives rise to the tentorial, inferior hypophyseal, and dorsal meningeal arteries (see Fig. 2-12B–G, I, J). However, these branches can arise separately from the internal carotid artery or in different combinations,9,36,37 and the origin of some secondary arteries directly from the meningohypophyseal trunk can give the appearance of more than the usual number of branches (see Fig. 2-12H). The posterior bend of the internal carotid artery and the origin of the meningohypohyseal trunk can be exposed through Parkinson’s triangle, located in the lateral view between the trochlear and ophthalmic nerves, except when the carotid is elongated and tortuous, causing the posterior bend to rise above the trochlear nerve11,12 (see Fig. 2-12D–F). The oculomotor and trochlear nerves enter the dural roof of the cavernous sinus just above or slightly behind the trifurcation of the meningohypophyseal trunk. According to Harris and Rhoton,11 the meningohypophyseal trunk provides a branch to the tentorium in 100% of 50 cavernous sinuses examined, making the tentorial artery the most constant branch leaving this trunk.
Tentorial arteries
The tentorium has two sources of supply: the medial tentorial and the lateral tentorial arteries. The medial tentorial artery usually arises from the meningohypophyseal trunk, but may also arise from the inferolateral trunk, middle meningeal, accessory meningeal, ophthalmic, and lacrimal arteries (see Fig. 2-12E, F, K, Q). It ascends to the roof of the cavernous sinus and then posterolaterally, along the free edge of the tentorium, to contribute to the supply of the transdural segment of the oculomotor and trochlear nerves, the walls of the cavernous sinus, and the medial third of the tentorium.12,41,42 It departs from the cavernous sinus just beneath the entrance of the trochlear nerve and initially courses posteriorly about 5 mm from the free margin of the tentorium (see Fig. 2-12D, E). As it approaches the region of the straight sinus, it curves laterally, ramifying within tentorium and anastomosing along the base of the falx with branches from its mate from the opposite side12,38,41 (see Figs. 2-3 and 2-5). It may also anastomose with the meningeal branches of the ophthalmic artery. Although usually described as a branch of the tentorial division of the meningohypophyseal trunk,37 the medial tentorial artery may also arise directly from the posterior vertical or from the horizontal segment of the cavernous carotid (as a branch of the inferolateral trunk), the accessory meningeal, intraorbital ophthalmic, lacrimal, or middle meningeal arteries.18,42
The term Bernasconi’s artery is used as a synonym for the medial tentorial artery11,12,42 (see Table 2-1). Bernasconi and Cassinari (1956) were the first to describe an arterial vessel involved in the supply of the tentorium and its lesions. At that time, they thought the vessel originated from the external carotid artery39,41,43,44 but its true origin from the internal carotid artery later became apparent.38,41,44
When visible during normal angiography, the medial tentorial artery ranges in length from 5 to 35 mm. A pathologic lesion has been considered a possibility if the tentorial artery can be followed, in the angiogram, for a distance longer than 40 mm.12,39 Other aspects such as increased diameter, undulating course, and multiple branching also suggest the presence of a lesion.13 Its presence on angiograms is not diagnostic of a tentorial meningioma as first suggested, because it can be seen in arteriovenous malformations, gliomas with tentorial invasion, trigeminal neuromas, and even in normal patients.12,41,43,45
The lateral tentorial artery commonly arises as a single trunk with the medial tentorial artery (see Fig. 2-12D, E). From its origin, it passed backward, upward, and slightly laterally to enter the tentorium along its attachment to the petrous ridge, and continued backward to supply the tentorial area lateral to that supplied by the medial tentorial artery.28,42,45 The lateral tentorial artery anastomoses with the petrosal and petrosquamosal branches of the middle meningeal artery and the lateral branch of the dorsal meningeal artery (see Figs. 2-3 and 2-6).
Dorsal meningeal artery
The dorsal meningeal artery, also called lateral clival artery, is the adult remnant of the trigeminal artery.31,36 It arises from the meningohypophyseal trunk in most cases and passes posteriorly through the cavernous sinus, to supply the dura of the dorsum sellae and clivus and anastomose with its mate from the opposite side across midline (see Fig. 2-12B–E, G–J). It arose from the meningohypophyseal trunk in 90% of the 50 cavernous sinus studied by Rhoton and Harris.11 In 6% of cases, it arises directly from the lateral surface of the posterior ascending portion of the cavernous carotid, just below the meningohypophyseal trunk.11,12,46
The dorsal meningeal artery divides into medial and lateral branches (see Fig. 2-12H, I). The medial branch passes below the petrosphenoid ligament, which roofs Dorello’s canal, to accompany and supply the abducens nerve into the canal31,36,38 and anastomoses with the clival ramus of the jugular branch of the ascending pharyngeal artery (see Figs. 2-1 and 2-6). The medial branch of the dorsal meningeal artery has a reciprocal relationship with the medial clival artery, which arises as a direct or as a secondary branch of the internal carotid artery from the inferior hypophyseal artery. The medial clival arteries initial course is anterior to the posterior clinoid process, but it also distributes to the dura over the posterior surface of dorsum sellae, where it anastomoses, across the midline, with its counterpart from the opposite side and also with the medial branch of the dorsal meningeal artery (see Fig. 2-12A–C). If no medial clival artery is found, a branch arises directly from the dorsal meningeal artery or its medial branch and courses medially and superiorly, on the posterior aspect to the posterior clinoid process and dorsum sellae, supplying part of the territory of the medial clival artery (see Fig. 2-12H, I).
The lateral branch of the dorsal meningeal artery passes above the trigeminal cistern (Meckel’s cave) and accompanies the superior petrosal sinus along the petrous ridge, thus participating in the basal arterial arcade of the tentorium cerebelli (see Fig. 2-3). This branch anastomoses, lateral to the trigeminal ganglion, with the lateral tentorial artery and branches of the middle meningeal artery running over the superior surface of the temporal bone.
Inferior hypophyseal artery
The inferior hypophyseal artery arises most frequently from the meningohypophyseal trunk (see Fig. 2-12F, G) or directly from the medial surface of the posterior ascending segment of the cavernous carotid artery (see Fig. 2-12H–J, N).11,31,36 It passes medially across the cavernous sinus to reach the lateral surface of the posterior lobe and capsule of pituitary gland. The artery divides into superior and inferior branches that anastomose with their mates of the opposite side, forming an arterial circle anterior to the dorsum sellae (see Fig. 2-12H). The inferior branch of this arterial circle, along with the more anteriorly located capsular arteries, may supply the dura on the sellar floor.11,13,40,46 The capsular arteries usually arise directly from the medial surface of the horizontal cavernous carotid (see Fig. 2-12N), but may also be branches of the inferior hypophyseal artery.38 The dura of the posterior clinoid and cavernous sinus can also be supplied by the inferior hypophyseal branch, through the medial clival artery, which can also arise directly from the cavernous carotid.36,42
Luschka, in 186038,40 first identified the inferior hypophyseal artery in man. This artery is the adult remnant of the primitive maxillary artery. In the lateral angiogram, the inferior hypophyseal artery is superimposed on the carotid siphon and is therefore impossible to identify even after subtraction studies.36,40
Inferolateral trunk
The inferolateral trunk, also called the lateral main stem39 or the artery of the inferior cavernous sinus,38 arises from the lateral side of the midportion of the horizontal segment of the intracavernous carotid, approximately 5 to 8 mm distal to the origin of the meningohypophyseal trunk11,46 (see Fig. 2-12K, L). It arises directly from the carotid artery in 84% of the cavernous sinuses and from the meningohypophyseal trunk in another 6%.11
The inferolateral trunk passes above (96%) or below (4%) the abducens nerve47 and descends, through or lateral to the ophthalmic nerve, and supplies the dura of the inferolateral wall of the cavernous sinus and adjacent middle fossa up to the gasserian ganglion (see Figs. 2-1,2-4, and 2-12K–P). The branches of the inferolateral trunk anastomose with the middle and accessory meningeal arteries.46 The branches to the gasserian ganglion may run in the dura lateral to the ganglion or pass superior to the motor root to reach the dura on the medial side of the ganglion (see Fig. 2-12P).
In its most complete form, the inferolateral trunk gives rise to superior, anterior, and posterior branches9,48 (see Fig. 2-12Q). The superior branch supplies the roof of the cavernous sinus. It gives rise to a medial tentorial branch in approximately 40% of cases48 (see Fig. 2-12K, Q). The anterior and the posterior divisions divide into a medial and a lateral branch. The medial branch of the anterior division passes forward and supplies the oculomotor, trochlear, and abducens nerves; enters the orbit through the superior orbital fissure; and terminates as the deep recurrent ophthalmic artery (see Fig. 2-12K–M). The lateral branch passes toward the foramen rotundum and supplies the dura of the adjacent temporal fossa and maxillary nerve (see Fig. 2-12K, O, Q). The medial branch of the posterior division is distributed to the abducens nerve, medial third of the gasserian ganglion, and the mandibular nerve (see Fig. 2-12P). The lateral branch of the posterior division supplies the middle and lateral thirds of the gasserian ganglion and adjacent dura48 (see Fig. 2-12Q). Because of its reciprocal relationship with the cavernous branch of the middle meningeal artery, the posterior division may also reach the hiatus fallopi to supply the facial nerve.9,19 The posterior division of the inferolateral trunk anastomoses with the recurrent artery of foramen lacerum (see Fig. 2-4).
McConnell’s capsular arteries
The term McConnell’s capsular arteries refers to the anterior and inferior capsular arteries, tiny branches that arise distal to the origin of the inferolateral trunk. The inferior capsular artery is the more proximal of the capsular arteries. It arises from the inferomedial surface of the horizontal segment of the cavernous carotid, distal to the origin of the inferolateral trunk, or as a secondary branch of the inferior hypophyseal artery. It runs medially in the dural covering of the inferior surface of the anterior lobe, giving branches to the dura of the floor of the sella turcica (see Fig. 2-12N). The anterior capsular artery arises from the medial aspect of the internal carotid artery just before it pierces the roof of the cavernous sinus and runs medially in the dura of the anterior margin and roof of the sella turcica, anastomosing with its mate of the opposite side.
McConnell’s capsular arteries are frequently absent,11,38,40,46 being found in 8% to 50% of cavernous sinuses.37,38,40,46 This variability may be due to difficulty in injecting these arteries40 or its origin as a branch of the inferior hypophyseal artery.46 The capsular arteries have been visualized angiographically in patients with sphenoid sinus carcinoma, craniopharyngioma, and parasellar meningiomas.13
Recurrent artery of foramen lacerum
This tiny artery originates from the posterior ascending portion of the carotid siphon and descends into the foramen lacerum, supplying the pericarotid autonomic nervous plexus and the arterial wall9,48 (see Figs. 2-11F and 2-12C, Q). This artery cannot be seen angiographically after internal carotid artery injections, because of the density of the parent carotid, but is visible after ascending pharyngeal injection because of its anastomoses with the carotid branch of the ascending pharyngeal artery. The recurrent artery of the foramen lacerum also anastomoses along the inferior surface of the trigeminal ganglion with the posterior branch of the inferolateral trunk (see Figs. 2-1 and 2-4).
Supraclinoid carotid branches
The ophthalmic and anterior cerebral branches of the supraclinoid carotid may supply the dura.
Ophthalmic artery
Contributions from the ophthalmic artery to the dura derive mainly from its ethmoidal, recurrent ophthalmic and lacrimal branches (Figs. 2-13 to 2-15).
Ethmoidal arteries
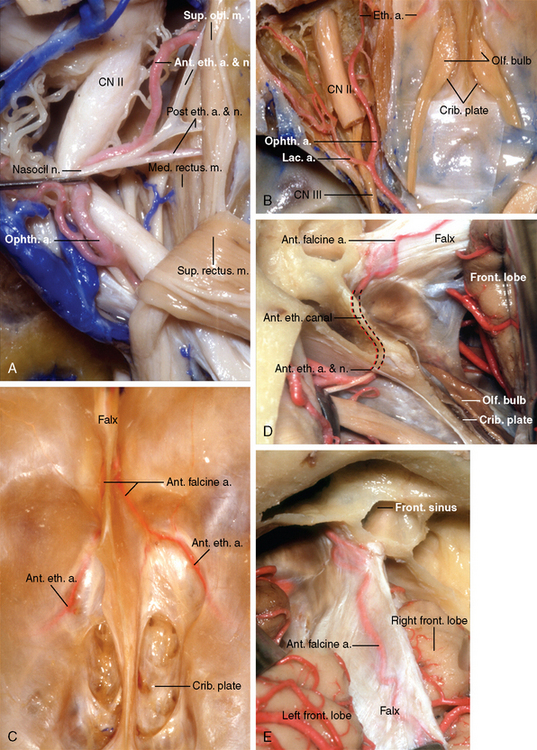
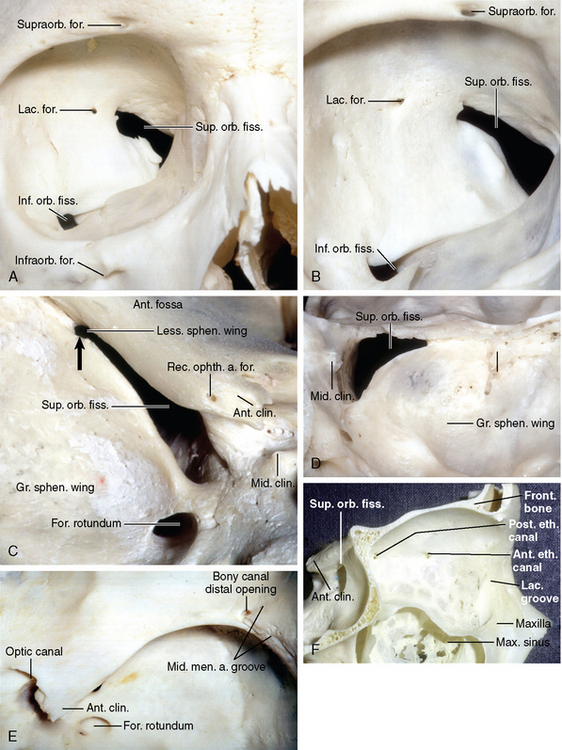
The anterior and posterior ethmoidal arteries arise from the ophthalmic artery in the medial third of the orbit (see Fig. 2-13A, B) and range in diameter between 0.5 and 1 mm in diameter.49 These arteries enter the anterior and posterior ethmoidal canals with their corresponding ethmoidal nerves and leave the canals to enter the anterior cranial fossa at the anterior and posterior ends of the lateral edge of the cribriform plate (see Fig. 2-13A–D). The orbital opening of the ethmoidal canals are located at the junction of the roof and medial wall of the orbit, along the frontoethmoid suture formed by the medial edge of the orbital plate of the frontal bone above and the perpendicular plate of the ethmoid below (see Fig. 2-14F). Intracranially, the ethmoidal canals open on the suture between the orbital part of the frontal bone and the cribriform plate. Before reaching the intracranial cavity, the ethmoidal arteries send branches to the ethmoid sinuses and nasal cavity and septum. The ethmoidal arteries are prominently enlarged in vascular tumors or dural arteriovenous malformations of the anterior fossa.
Intracranially, the anterior ethmoidal artery has been also called the anterior meningeal artery, especially when its territory extends to the dura of the frontal convexity50 (see Fig. 2-2). It gives origin to the artery of the falx cerebri, also called the anterior falcine artery,50–52 which enters the falx at the cribriform plate and supplies the anterior portion of the falx cerebri and adjacent dura covering the frontal pole that borders with the dural territory of the middle meningeal artery (see Fig. 2-13C–E). The anterior falcine artery may be present on both sides but either the right or left may predominate.52 It artery is frequently seen, on normal carotid angiograms, ascending in the falx near its attachment to the convexity dura.52 It may enlarge in falx meningiomas and occlusive cerebrovascular diseases.51 The anterior meningeal branches of the ethmoidal arteries often supplies meningiomas from the olfactory groove and may be seen on angiography to be displaced in arch along the surface of the tumor.28 The anterior falcine artery is not shifted laterally by intracranial masses because it courses within the rigid falx.52
The posterior ethmoidal artery passes through the posterior ethmoidal canal and enters the dura at the posterior margin of the cribriform plate and supplies the dura of the medial third of the floor of the anterior cranial fossa, including the planum sphenoidale, anterior clinoid process, and chiasmatic groove (see Fig. 2-1). It anastomoses posteriorly with the branches of the internal carotid artery, laterally with branches of the middle meningeal artery, and anteriorly with the meningeal branches of the anterior ethmoidal artery (see Figs. 2-1 and 2,4).
Recurrent ophthalmic arteries
The ophthalmic arteries may give rise to two recurrent ophthalmic arteries, one superficial and one deep that supply the dura. The superficial recurrent ophthalmic artery generally arises at a sharp angle, from the proximal portion of the ophthalmic artery in the optic canal, and passes backwards, to supply the dura over the anterior clinoid, adjacent lesser sphenoid wing, and the anterior and medial parts of the middle fossa50 (see Fig. 2-14C) and anastomoses with branches of the middle meningeal artery and posterior ethmoidal artery (see Figs. 2-1 and 2-4). It supplies the dural roof of the cavernous region and may continue as the medial tentorial artery (see Table 2-1). In the lateral angiographic view it projects above the C4 portion of the carotid siphon crossing the C3 portion under or on the anterior clinoid process somewhat more cephalad than the deep recurrent ophthalmic artery.53
The deep recurrent ophthalmic artery arises from the initial intraorbital part of the ophthalmic artery, courses laterally, through the annulus of Zinn and the medial portion of the superior orbital fissure, crossing the anterior venous space in the cavernous sinus to supply the dura adjacent to the wall of cavernous sinus, bordering the territory of the inferolateral trunk (see Fig. 2-12M). The presence of the deep recurrent ophthalmic artery is closely related to the embryological process that results in the adult form of the ophthalmic artery. Initially the primitive ophthalmic artery arises from two sources, the anterior cerebral artery and the intracavernous carotid artery. The ophthalmic artery, arising from the anterior cerebral artery, undergoes a process of migration to arise from the paraclinoid internal carotid artery. The ophthalmic artery, arising from the cavernous carotid, also undergoes regression to become the deep recurrent ophthalmic artery.48 A cavernous origin of the ophthalmic artery, either with or without an ophthalmic artery arising in the usual intradural location, has been reported in 6% to 8% of the cases,11 a finding explained by the persistence of the dorsal primitive ophthalmic artery. When there are two ophthalmic arteries, one passing through the optic canal and one through the superior orbital fissure either may be dominant.
Lacrimal branch
The most important collateral blood supply to the orbit is the middle meningeal artery54 and, in reverse fashion, the ophthalmic arterial system can provide flow to the territory of the middle meningeal artery and its branches through the anastomoses between the anterior branch of the middle meningeal artery and the lacrimal branch of the ophthalmic artery (see Fig. 2-15). The presence of arterial connections between the ophthalmic arterial system and the middle meningeal artery has its origin in the embryonic development of the stapedial artery55 and involves persistence of anastomoses that are normal at one stage of the development but later regress.24,56 In a 20-mm embryo the stapedial artery (a branch of the hyoid artery) divides into maxillomandibular and supraorbital divisions. The maxillo-mandibular division penetrates the foramen spinosum and is eventually annexed by the external carotid artery, to form the maxillary artery and extracranial segment of the middle meningeal artery. The supraorbital division, arises in the middle fossa and reaches the superior orbital fissure, providing retro- and intraorbital branches that will, in the adult, become the site for the anastomose of the lacrimal with the middle meningeal artery. The supraorbital division of the primitive stapedial artery is thus responsible for formation of the intracranial segment of the middle meningeal artery and the extraocular ophthalmic artery.56,57 The supraorbital division also gives off a branch near the superior orbital fissure that courses medially along the posterior edge of the lesser wing of the sphenoid to be distributed to the anterior clinoid process and roof of the cavernous sinus, participating in the supply of the oculomotor and trochlear nerves and sometimes coursing posteriorly as the marginal artery of the tentorium. This arterial branch provides the link between the intraorbital vessels (lacrimal or ophthalmic) and the posterior branches of the carotid siphon.42,48 In the adult, this artery possibly corresponds to the superficial recurrent ophthalmic artery.
Partial or complete persistence of intraorbital and retro-orbital branches of the supraorbital artery explains both the dependence of the orbital vascularizarion on the middle meningeal artery and the variable participation of the ophthalmic artery in vascularization of the convexity dura56,58 (see Fig. 2-15C). If the proximal portion of the ophthalmic artery regresses, the adult ophthalmic artery originates, not from the internal carotid artery, but from the middle meningeal artery.24,54 Unilateral middle meningeal artery origin of the ophthalmic artery was seen in 2 of 170 anatomic specimens and 3 of 3500 cerebral angiograms. Demonstration of this anomaly bilaterally is extremely rare; only 4 cases have been reported.59 Ophthalmic origin of the middle meningeal artery can be detected in skulls by the absence or reduced size of the foramen spinosum and/or absence, attenuation or interruption of the osseous sulcus for the middle meningeal artery along the floor of the middle fossa, and has been found in 10% of specimens.44,54,60 Elevating the dura from the greater and lesser wings of the sphenoid, removing the sphenoid ridge, or embolization procedures involving the external carotid artery risk blindness in patients with a middle meningeal origin of the ophthalmic artery.24,56,59 If the supraorbital stapedial branch persists, but its embryonic anastomoses with the primitive ophthalmic artery regresses, the resultant anomaly includes an ophthalmic artery that supplies only the globe and remains separated from intraorbital extraocular branches (muscular and lacrimal branches), which are then supplied by the middle meningeal artery.
The ophthalmic artery complex can supply the dura of the convexity and related lesions by three different anomalous meningeal vessels. The commonest found, in 0.5% of angiograms, is the middle meningeal artery that originates from the ophthalmic artery. This results from failure of the proximal intraorbital stapedial branches to involute in association with the involution of the maxillomandibular division of the stapedial artery. The ophthalmic artery may also supply dural lesions through the anterior branch of the middle meningeal, as occurs if there is a partial involution of retro-orbital stapedial branches. The accessory meningeal artery can also arise from the ophthalmic artery. The anatomico–radiologic features of anomalous meningeal branches arising from the ophthalmic artery are typical. These vessels usually arise at the point that the ophthalmic artery passes above the intraorbital optic nerve near the origin of the posterior ethmoidal artery, and pass upward through the superior orbital fissure to reach the cranial dura. Meningeal vessels of ophthalmic origin and related lesions are opacified exclusively by internal carotid artery injection whereas external carotid artery injection fails to visualize them. The anterior branch of the middle meningeal artery and the accessory meningeal artery of ophthalmic origin may be distinguished on angiograms from the anterior meningeal artery or artery of the falx, because this later branch courses near the midline in anteroposterior view and a few millimeters inside the frontal convexity in the lateral view, while the anterior branch of the middle meningeal artery and the accessory meningeal artery of ophthalmic origin have a more lateral course, away from the midline in the AP view and posterior to the frontal convexity in the lateral view.56
In 30% of the cases48,53 in which the orbital branch of the supraorbital artery divides proximally, within the middle cranial fossa, the sphenoid bone, which ossifies later, will allow more than one transosseous route for these vessels. The anastomotic ramus between the lacrimal and the middle meningeal artery usually enter the orbit through the superior orbital fissure; however, in as much as 50% of dissected specimens an additional foramen can be seen in the greater wing of the sphenoid60 (see Fig. 2-14A–C). This foramen has been given several names including the lacrimal, Hyrtl, meningorbital, cranio-orbital, sinus canal, or sphenofrontal foramen.54,60
The lacrimal foramen is composed of multiple openings in 5% to 15% of the cases and occupies a variable position relative to the superior orbital fissure.54,60 The lacrimal foramen can be located lateral to the superior orbital fissure or confluent with its lateral end54 (see Fig. 2-14A–C). Two middle meningeal branches can coexist: one penetrating the orbit through the superior orbital fissure and the other, the lacrimal foramen. The branch that passes through the lacrimal foramen is referred to as the meningolacrimal artery, and the one entering the orbit through the superior orbital fissure is called sphenoidal artery or recurrent meningeal artery or orbital branch of the middle meningeal artery (see Fig. 2-15A, B).
Sometimes the meningolacrimal artery is intact distally but fails to anastomose proximally with the middle meningeal artery and instead breaks up into a fine anastomotic plexus within the dura.54 The recurrent meningeal artery runs in the sphenoparietal sulcus, on the lower edge of the sphenoid ridge, with the sphenoparietal sinus. This artery is long and tortuous while the meningolacrimal has a short, straight path to the orbit and to its anastomosis with the lacrimal artery (see Fig. 2-15A, B). The recurrent meningeal artery may be associated with a laterally expanded superior orbital fissure (see Fig. 2-14C). The meningeal branches of the ophthalmic artery, because of this variable distribution, should be carefully studied in sphenoid ridge, frontobasal, and anterior falcine tumors. A common angiographic finding in these lesions is enlargement of the ophthalmic artery.50
Anterior cerebral artery
Dural branches can arise at two levels along the anterior cerebral artery.9 The olfactory branches from the anterior cerebral artery, which course on the olfactory bulb may anastomose with the olfactory branches from the ethmoidal arteries in the region of the cribriform plate; and the pericallosal artery can send branches to the free margin of falx, anastomosing anteriorly with the anterior falcine branch of the ophthalmic artery and posteriorly with the dural branches from the posterior cerebral artery9 (see Figs. 2-1 and 2-4).
Vertebrobasilar system
Vertebral artery branches
The anterior and posterior meningeal arteries arise from the extracranial segment of the vertebral artery to supply a portion of the posterior fossa dura (Fig. 2-16).
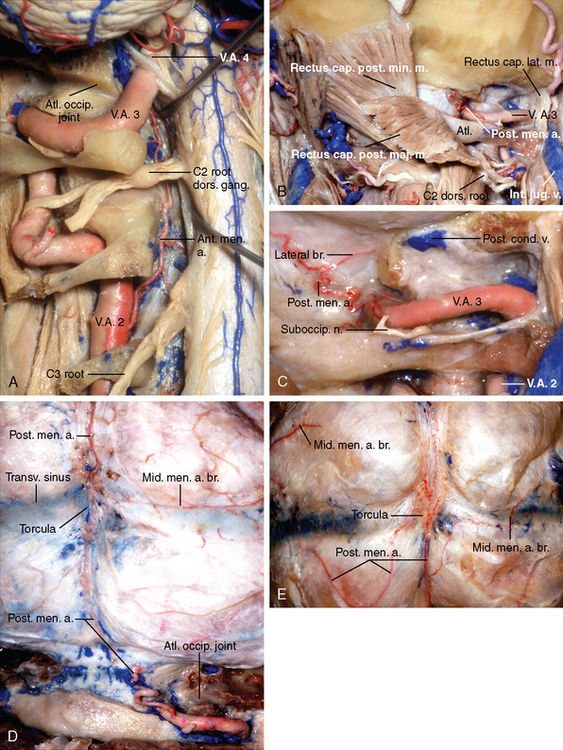
Anterior meningeal artery
The anterior meningeal artery arises from the vertebral artery at the level of the C2, passes medially through the C2–C3 foramen in front of the C3 root, and courses upward near the midline, sending several twigs to the anterior dura along its course (see Fig. 2-16A). These paired arteries join to form an arch in the dura at the level of the apex of the dens, which gives off multiple fine rami to the dura in the atlanto-occipital space.16,60–62 Intracranially, the anterior meningeal artery anastomoses with the hypoglossal branch of the ascending pharyngeal artery16,61,63,64 (see Figs. 2-1 and 2-6).
The anterior meningeal artery can be identified in approximately 50% of subtraction angiograms.60 Its small size, results in only the first 1 to 1.5 cm of its course being seen angiographically.17,61 In the frontal angiogram, it is seen to arise from the medial aspect of vertebral artery and courses upward toward the foramen magnum. In the lateral angiogram, its initial segment is projected behind the vertebral artery, but it is subsequently seen into the anterior portion of the spinal canal, immediately posterior to the vertebral bodies, and anterior to the anterior spinal artery.16,61,65
Posterior meningeal artery
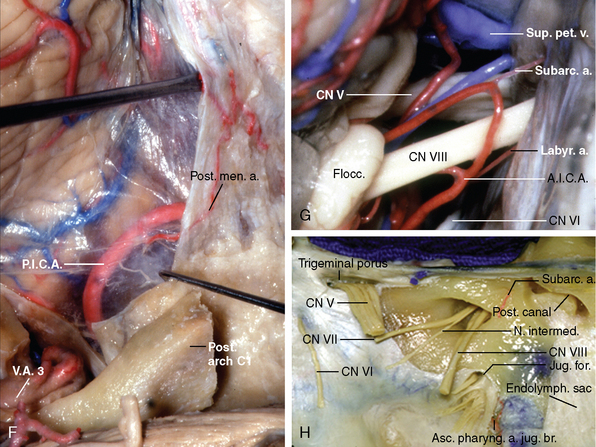
The posterior meningeal artery usually arises from the segment of the vertebral artery that runs in the groove for the vertebral artery on the upper edge of the posterior arch of atlas (V3 segment) (see Fig. 2-16B–D). Its origin is usually closer to the dural entrance than to the transverse foramen of the atlas. Its initial course is along the upper posterior aspect of the extradural vertebral artery toward the posterolateral edge of foramen magnum, where it enters the intracranial dura (see Fig. 2-16B). It ascends posterosuperiorly, nearly parallel to the internal occipital crest, to reach the attachment of the cerebellar falx. Around the level of the external occipital protuberance, the artery bifurcates and anastomoses with the meningeal branches of the occipital and middle meningeal arteries6 (see Figs. 2-7 and 2-14D).
The posterior meningeal artery can be divided into an extracranial and an intracranial portion. The extracranial portion is tortuous, probably as a response to the motility of the neck16 and extends from origin to the atlanto-occipital space. The intracranial portion shows a relatively straight configuration17 (see Fig. 2-14B–D). This pattern, on angiography, facilitates differentiation of the posterior meningeal artery from the branches of the posterior inferior cerebellar artery. The posterior meningeal artery, seen on 30% to 40% of angiograms, is easier to identify on lateral films.16,17
The posterior meningeal artery may also originate from the occipital artery, the hypoglossal branch of the ascending pharyngeal artery, the cervical internal carotid artery,66 and the posterior inferior cerebellar artery.6 Its origin from an artery supplying the brain parenchyma can result from the persistence of the preexisting anastomotic channels between the primitive cerebral and meningeal vessels, and regression of the proximal stem of the posterior meningeal artery (see Fig. 2-14F).
Anterior inferior cerebellar artery
The subarcuate artery usually originates from the lateral pontine segment of the anterior inferior cerebellar artery (AICA), medial to the porus, penetrates the dura covering the subarcuate fossa, and enters the subarcuate canal (see Fig. 2-14G). It may arise as a branch of the labyrinthine artery, which also arises from AICA or as a single trunk from a cerebellar branch of AICA (cerebellosubarcuate artery). In the few cases in which the artery arises inside the internal acoustic canal, it reaches the subarcuate canal after a short recurrent segment or by piercing the meatal roof.12 The subarcuate artery anastomoses with the branches of the stylomastoid artery within the petrous bone, the branches of the middle meningeal artery running over the superior surface of the petrous bone and the mastoid branches of the occipital artery. It supplies the dura of the internal acoustic meatus and adjacent posterior surface of the petrous bone as well as the bone in the region of the semicircular canals. Although not seen angiographically, the subarcute artery is involved in the formation of the dural collateral circulation that joins the leptomeningeal collaterals in cases of anterior inferior cerebellar artery occlusion.48,58
Posterior cerebral artery
The posterior part of the falx cerebri and the adjacent medial part of tentorium may be supplied in part by a meningeal branch of the posterior cerebral artery. Wollschlaeger and Wollschlaeger67 first described this meningeal branch during anatomical dissections and named it the artery of Davidoff and Schechter, in honor of their mentors (see Figs. 2-3 and 2-5). This artery originates from the peduncular or ambient segment of the posterior cerebral artery, courses around the brainstem to the midline and makes a sharp angulated upward turn to pierce the tentorium and supplies the tentorium and adjacent falx cerebri along the falcotentorial angle. An enlarged meningeal branch of the posterior cerebral artery has been identified angiographically in vascular tumors and arteriovenous malformations involving the falcotentorial junction.68 A meningeal branch of the posterior cerebral artery could not be identified in this study or in a prior study from this laboratory.69 However the senior author (ALR) has noted the presence of this variation in studies related to other areas.
Dural Sinuses and Veins
Superior sagittal sinuses
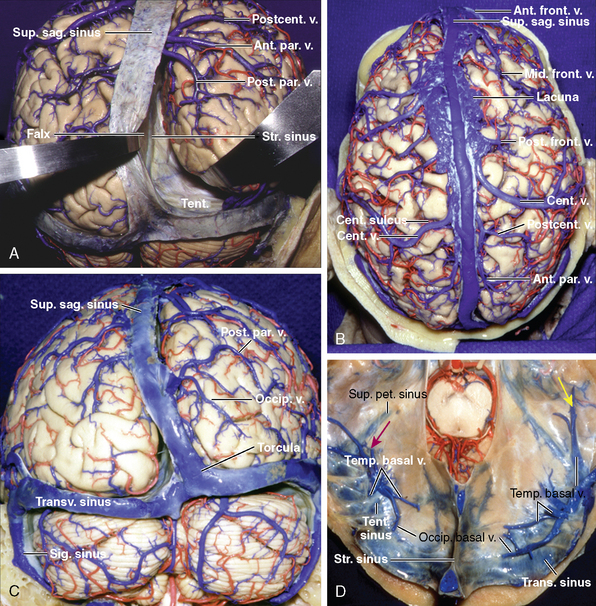
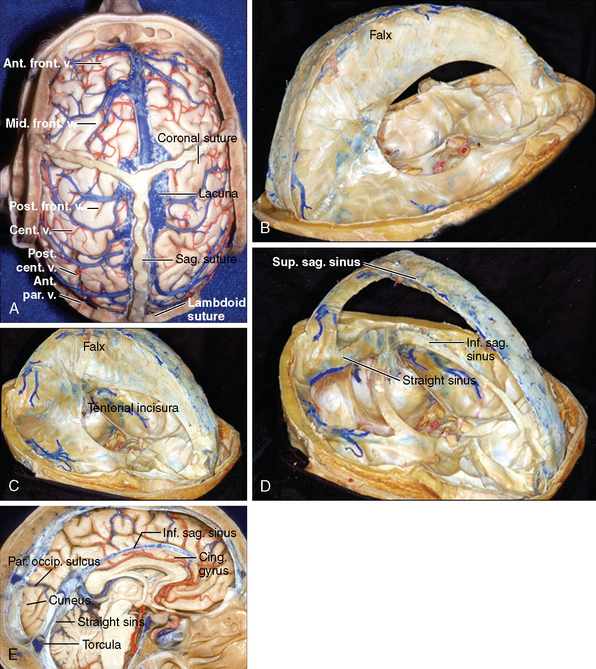
Superior sagittal sinus is attached to the falx cerebri superiorly, to crista galli anteriorly and tentorium, posteriorly. It is triangular in cross section and has right and left lateral angles at its junction with the dura mater covering the convexities and an inferior angle at its junction with the falx. The superior sagittal sinuses courses in the midline in the shallow groove on the inner table of the cranium, and grows larger as it continues posteriorly. In approximately 60% of cases, superior sagittal sinus ends by becoming the right transverse sinus.70–74 At the termination of the superior sagittal sinus is a dilatation, known as confluence of the sinuses or torcular herophili.
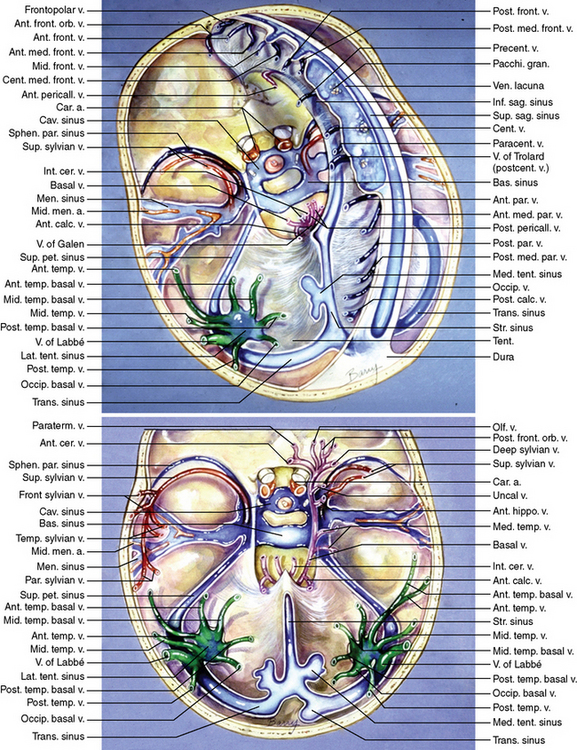
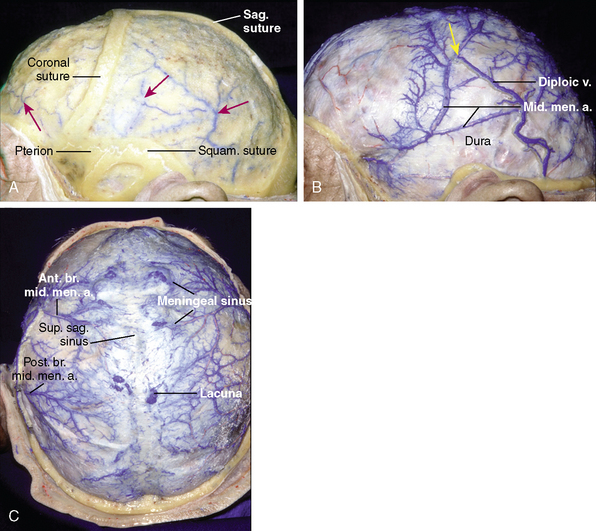
The cortical veins may pass directly to the superior sagittal sinus, or they may first join the meningeal veins. Enlarged venous spaces, called lacunae, are contained in the dura mater adjoining the superior sagittal sinus. The lacunae are largest and most constant in the parietal and posterior frontal regions. Smaller lacunae are found in the occipital and anterior frontal regions. The lacunae receive predominantly the drainage of the meningeal veins, which accompany the meningeal arteries in the dura mater but cortical veins can also pierce its deeper surface72–77 (Figs. 2-17, 2-18, and 2-19).
The inferior sagittal sinus
Inferior sagittal sinus occupies the posterior two thirds of the free inferior edge of the falx cerebri. It ends by joining the great cerebral vein to form straight sinus. It arises from the union of veins from the adjacent part of the falx, corpus callosum, and cingulated gyrus. The largest tributaries of the inferior sagittal sinus are the anterior pericallosal veins. The superior sagittal sinus may communicate through venous channels in the falx with the inferior sagittal sinus70,75 (see Figs. 2-17 and 2-19).
Straight sinuses
This venous sinus is formed by the union of the inferior sagittal sinus with the great cerebral vein. It is attached to the tentorium cerebelli and drains either into the right or, most commonly, the left transverse sinus.72–74,77 (see Figs. 2-17 and 2-19).
Transverse sinuses
The right and left transverse sinuses originate at the torcular herophili and course laterally from the internal occipital protuberance in a shallow groove between the attachments of the tentorium to the inner surface of the occipital bone. The right transverse and sigmoid sinus and the right jugular vein are the main effluent route to the superficial venous system, whereas the left transverse and sigmoid sinus and the left internal jugular vein drain the venous blood mainly from the deep venous system of the brain, which comprise the internal cerebral, basal and great veins77 (see Figs. 2-17 and 2-18).
Tentorial sinuses
These sinuses divide into the medial and lateral groups.76 The medial tentorial sinuses are formed by the convergence of veins from the superior surface of the cerebellum, and the lateral tentorial sinuses are formed by the convergence of veins from the basal and lateral surfaces of the temporal and occipital lobes. The medial group drains into transverse sinuses and the lateral group drains into both straight and transverse sinuses.77
Cavernous sinuses
These large sinuses are approximately 2 cm long and 1 cm wide. They are located on each side of sella turcica and the body of the sphenoid bone. There are many trabeculae that contain blood channels. Each cavernous sinus receives blood from the superior and inferior ophthalmic veins, the superficial middle cerebral vein in the lateral fissure of the cerebral hemispheres. The cavernous sinus communicates through the superior petrosal sinus with the junction of the transverse and sigmoid sinuses and through the inferior petrosal sinus with the sigmoid sinus77 (see Fig. 2-17).
Superior petrosal sinuses
These venous sinuses are small channels that drain the cavernous sinuses. They run from the posterior ends of the cavernous sinuses to the transverse sinuses. Both of petrosal sinuses lie in the attached margins of the tentorium cerebella to the petrous ridge. The superficial sylvian veins may empty into an infrequent tributary of the superior petrosal sinus called the sphenopetrosal sinus77 (see Fig. 2-17).
Inferior petrosal sinuses
The inferior petrosal sinuses start at the posteroinferior margin of cavernous sinus and drain the cavernous sinuses into the internal jugulae veins. They run in a groove between petrous bone and occipital bone.78
Meningeal veins
The small venous channels that drain the dura mater covering the cerebrum are called the meningeal veins. They are small sinuses that usually accompany the meningeal arteries. The meningeal veins that accompany the meningeal arteries course between the arteries and the overlying bone. The fact that the artery presses into the veins gives them the appearance ofparallel channels on each side of their respective arteries. The largest meningeal veins accompany the middle meningeal artery. The meningeal veins drain into the large dural sinuses along the cranial base at their lower margin and into the venous lacunae and superior sagittal sinus at their upper margin. The veins accompanying the anterior branch of the middle meningeal artery join the sphenoparietal or cavernous sinus or may pass through the sphenoidal emissary veins. The meningeal veins accompanying the posterior branch of the middle meningeal artery join the transverse sinus. The meningeal veins may course through a superficial tunnel on the inner surface of the bone so that they have both an intradiploic and an intradural course. The meningeal veins receive diploic veins from the calvarium77 (Fig. 2-20).
NEURAL SUPPLY TO THE CRANIAL DURA MATER
The arachnoid and pia matter do not contain nerve fibers. Only dura matter and blood vessels have a neural supply.78
[1] Butler A.B., Hodos W. Comparative Vertebrate Anatomy. Evolution and Adaption. New York: Wiley-Liss, 1996.
[2] Haines D.E., Frederickson R.G. The meninges. In: Al-Mefty A., editor. Meningiomas. New York: Raven Press; 1991:9-25.
[3] Warwick R., Williams P.L. Gray’s Anatomy of the Human Body, 35th ed. New York: Churchill Livingstone, 1973.
[4] Yasuda A., Campero A., Martins C., Rhoton A.Jr, Ribas G.C. The medial wall of the cavernous sinus. Microsurgical anatomy. J Neurosurg. 2004;55(1):179-190.
[5] Streeter G.L. The developmental alterations in the vascular system of the brain of the human embryo. Contr Embryol. 1918;24:5-38.
[6] Tanohata K., Maehara T., Noda M., Katoh H., Sugiyama S., Okazaki A. Anomalous origin of the posterior meningeal artery from the lateral medullary segment of the posterior inferior cerebellar artery. Neuroradiology. 1987;29(1):89-92.
[7] Herman J.M., Spetzler R.F., Bederson J.B., Kurbat J.M., Zambramski J.M. Genesis of a dural arteriovenous malformation in a rat model. J Neurosurg. 1995;83:539-545.
[8] Kerber C.W., Newton T.H. The macro and microvasculature of the dura mater. Neuroradiology. 1973;6:175-179.
[9] Lasjaunias P., Berenstein A.. Surgical Neuroangiography, vol. 1. Springer-Verlag, New York, 1987.
[10] Lasjaunias P., Moret J. The ascending pharyngeal artery. Normal and pathologic radioanatomy. Neuroradiology. 1976;11:77-82.
[11] Harris F.S., Rhoton A.L.Jr. Anatomy of the cavernous sinus. A microsurgical anatomy study. J Neurosurg. 1976;45:169-180.
[12] Rhoton A.L.Jr. The posterior cranial fossa: microsurgical anatomy and surgical approaches. Neurosurgery. 2000;47(3):S195-210.
[13] Wallace S., Goldberg H., Leeds N., Mishkin M. The cavernous branches of the internal carotid artery. Am J Roentgenol Radium Ther Nucl Med. 1967;101:34-46.
[14] Houser O.W., Campbell J.K., Campbell R.J., Sundt T.M.Jr. Arteriovenous malformation affecting the transverse dural venous sinus-an acquired lesion. Mayo Clin Proc. 1979;54:651-661.
[15] Merland J.J., Bories J., Djindjian R. The blood supply of the falx cerebri, the falx cerebelli and the tentorium cerebelli. J. Neuroradiol. 1977;4:175-202..
[16] Manelfe C., Roulleau J., Combelles R., Grisoli F. La vascularisation de la dure-mere du trou occippital. Neurochirurgie. 1971;17(6):469-480.
[17] Newton T.H. The anterior and posterior meningeal branches of the vertebral artery. Radiology. 1968;91(2):271-279.
[18] Silvela J., Zamarron M.A. Tentorial arteries arising from the external carotid artery. Neuroradiology. 1978;14(5):267-269.
[19] Lapresle J., Lasjaunias P. Cranial nerve ischaemic arterial syndromes. Brain. 1986;109:207-215.
[20] Mujica P.H., Rosemblat A.M., Luessenhop A.J. Subarachnoid hemorrhage secondary to an aneurysm of the ascending pharyngeal artery. Case report. J Neurosurg. 1981;54:818-820.
[21] Gadre A.K., Fayad J.N., O’Leary M.J., Zakhary R., Linthicum F.H. Arterial supply of the human endolymphatic duct and sac. Otoryngol Head Neck Surg. 1993;108(2):141-148.
[22] Lasjaunias P., Theron J., Moret J. The occipital artery: anatomy, normal arteriographic aspects and embryological significance. Neuroradiology. 1978;15:31-37.
[23] Chandler S.B., Derezinki C.F. The variations of the middle meningeal artery within the middle cranial fossa. Anat Rec. 1935;62:309-316.
[24] Liu Q., Rhoton A.L.Jr. Middle meningeal origin of the ophthalmic artery. Neurosurgery. 2001;49(2):401-407.
[25] Royle G., Motson R. An anomalous origin of the middle meningeal artery. J Neurol Neurosurg Psychiatry. 1973;36(5):874-876.
[26] McLennan J.E., Rosembaum A.E., Haughton V.M. Internal carotid origins of the middle meningeal artery. Neuroradiology. 1974;7:265-275.
[27] Houser O.W., Baker H.L.Jr, Rhoton A.L.Jr, Okazaki H. Intracranial dural arteriovenous malformations. Radiology. 1972;105:55-64.
[28] Wickbom I., Stattin S. Roentgen examination of intracranial meningiomas. Acta Radiol. 1958;50:175-186.
[29] Blunt M.J. The blood supply of the facial nerve. J Anat. 1954;88:520-526.
[30] Rhoton A.L.Jr, Pulec J.L., Hall G.M., Boyd A.S.Jr. Absence of bone over the geniculate ganglion. J Neurosurg. 1968;28:48-53.
[31] Moret J., Lasjaunias P., Vignaud J., Doyon D. The middle meningeal blood supply to the posterior fossa. Neuroradiology. 1978;16:306-307.
[32] Seeger J.F., Hemmer J.F. Persistent basilar/middle meningeal artery anastomosis. Radiology. 1976;118(2):367-370.
[33] Waga S., Okada M., Yamamoto Y. Basilar-middle meningeal arterial anastomosis. Case report. J Neurosurg. 1978;49(3):450-452.
[34] Baumel J.J., Beard D.Y. The accessory meningeal artery of man. J Anat. 1961;95:386-402.
[35] Dilenge D., Geraud G. Accessory meningeal artery. Acta Radiol Suppl. 1976;347:63-69.
[36] Lasjaunias P., Theron J. Radiographic anatomy of the accessory meningeal artery. Radiology. 1976;121(1):99-104.
[37] Inoue T., Rhoton A.L.Jr, Theele D., Barry M.E. Surgical approaches to the cavernous sinus: a microsurgical study. Neurosurgery. 1990;26(6):903-932.
[38] Parkinson D. Collateral circulation of the cavernous carotid artery: anatomy. Can J Surg. 1964;7:251-268.
[39] Schnurer L., Stattin S. Vascular supply of intracranial dura from internal carotid artery with special reference to its angiographic significance. Acta Radiol (Diag). 1963;1:441-450.
[40] McConnell E.M. The arterial blood supply of the human hypophysis cerebri. Anat Rec. 1953;115:175-201.
[41] Smith D.R., Ferry D.J., Kempe L.G. The tentorial artery: its diagnostic significance. Acta Neurochir (Wien). 1969;21(1):57-69.
[42] Lasjaunias P. Anatomy of the tentorial arteries (letter). J Neurosurg. 1984;61:1159-1160.
[43] Handa H., Handa J., Tazumi M. Tentorial branch of the internal carotid artery (arteria tentorii). Am J Roentgen. 1966;98(3):595-598.
[44] Stattin S. Meningeal vessels of the internal carotid artery and their angiographic significance. Acta Radiol. 1961;55:329-336.
[45] Kramer R., Newton T. Tentorial branches of the internal carotid artery. Am J Roentgen. 1965;95:826-830.
[46] Rhoton A.L.Jr. The supratentorial cranial space. Microsurgical anatomy and surgical approaches. Neurosurgery. 2002;51(4):S1-410.
[47] Ishii R., Ueki K., Ito J. Traumatic fistula between a lacerated middle meningeal artery and a diploic vein; case report. J Neurosurg. 1976;44(2):241-244.
[48] Lasjaunias P., Moret J., Mink J. The anatomy of the inferolateral trunk (ILT) of the internal carotid artery. Neuroradiology. 1977;13(4):215-220.
[49] Vignaud J., Hasso A.N., Lasjaunias P., Clay C. Orbital vascular anatomy and embryology. Radiology. 1974;111(3):617-626.
[50] Kuru Y. Meningeal branches of ophthalmic artery. Acta Radiol. 1967;6:241-251.
[51] Handa J., Shimizu Y. Dural arteriovenous anomaly supplied by the anterior falcine artery. Neuroradiology. 1973;6:212-214.
[52] Pollock J.A., Newton T.H. The anterior falx artery: normal and pathologic anatomy. Radiology. 1968;91:1089-1095.
[53] Lasjaunias P., Brismar J., Moret J., Theron J. Recurrent cavernous branches of the ophthalmic artery. Acta Radiol Diagn (Stockh). 1978;19(4):553-560.
[54] Diamond M.K. Homologies of the meningeal-orbital arteries of humans: a reappraisal. J Anat. 1991;178:223-241.
[55] Padget D.H. The development of the cranial arteries in the human embryo. Contrib Embryol. 1949;32:205-262.
[56] Maiuri F., Donzelli R., de Divitiis O., Fusco M., Briganti F. Anomalous meningeal branches of the ophthalmic artery feeding meningiomas of the brain convexity. Surg Radiol Anat. 1998;20(4):279-284.
[57] Gabriele O.F., Bell D. Ophthalmic origin of the middle meningeal artery. Radiology. 1967;89(5):841-844.
[58] Lasjaunias P., Moret J., Manelfe C., Theron J., Hasso T., Seeger J. Arterial anomalies at the base of the skull. Neuroradiology. 1977;13(5):267-272.
[59] Watanabe A., Hirano K., Ishii R. Dural caroticocavernous fistula with both ophthalmic arteries arising from middle meningeal arteries. Neuroradiology. 1996;38:806-808.
[60] Morris P. Practical Neuroangiography. Baltimore: Williams & Wilkins, 1997.
[61] Greitz T., Lauren T. Anterior meningeal branch of the vertebral artery. Acta Radiol. 1968;7:219-224.
[62] Oliveira E., Rhoton A.L.Jr., Peace D. Microsurgical anatomy of the region of the foramen magnum. Surg Neurol. 1985;24:293-352.
[63] Haffajee M.R. A contribution by the ascending pharyngeal artery to the arterial supply of the odontoid process of the axis vertebra. Clin Anat. 1997;10:14-18.
[64] Lasjaunias P., Moret J., Theron J. The so-called anterior meningeal artery of the cervical vertebral artery. Neuroradiology. 1978;17:51-55.
[65] Nishikawa M., Hashi K., Shiguma M. Middle meningeal-middle cerebral artery anastomosis for cerebral ischemia. Surg Neurol. 1979;12(3):205-208.
[66] Kwak S., Nagashima T., Kobayashi S. Anomalous origin of the posterior meningeal artery from the internal carotid artery. Neuroradiology. 1980;19(2):103-104.
[67] Wollschlaeger P.B., Wollschlaeger G. Eine infratentorielle meningeale arterie. Radiologe. 1965;5:451-452.
[68] Wollschlaeger G., Wollschlaeger P.B. Arterial anastomoses of the human brain. A radiographic-anatomic study. Acta Radiol Diagn (Stockh). 1966;5:604-614.
[69] Zeal A.A., Rhoton A.L.Jr. Microsurgical anatomy of the posterior cerebral artery. J Neurosurg. 1978;48:534-559.
[70] Moore K.L., Dalley A.F. Clinically Oriented Anatomy, 3rd ed, Baltimore: Williams & Wilkins, 1992.
[71] Bisaria K. Anatomic variations of venous sinuses in the region of the torcular herophili. J Neurosurg. 1985;62:90-95.
[72] Browning H. The confluence of dural venous sinuses. Am J Anat. 1953;93:307-329.
[73] Huang Y., Okudera T., Ohta T., Robbins A. Anatomic variations of the dural venous sinuses. In: Kapp J., Schmidek H., editors. The Cerebral Venous System and Its Disorders. Orlando: Gune & Stratton; 1984:109-167.
[74] Kaplan H., Browder J., Knightly J., Rush B. Variation of the cerebral dural sinuses at the torcular herophili. Am J Surg. 1972;124:456-461.
[75] Seoane E., Rhoton A.L.Jr. Compression of the internal jugular vein by the transverse process of the atlas as the cause of cerebellar hemorrhage after supratentorial craniotomy. Surg Neurol. 1999;51:500-505.
[76] Braun J.P., Tournade A., Panisset J.L., Straub P. Anatomical and neuroradiological study of the veins of the tentorium and the floor of the middle cranial fossa, and their drainage to dural sinuses. J Neuroradiol. 1978;5:113-132.
[77] Albert L., Rhoton M.D.Jr. The cerebral veins. Neurosurgery. 2002;51(Suppl. 1):159-205.