36 Median Nerve Block
In the forearm the median nerve lies between the flexor digitorum profundus and the flexor digitorum superficialis muscles. This is where the median nerve is usually brightest on ultrasound scans.1
The two largest branches of the median nerve are the anterior interosseous nerve and the palmar cutaneous branch. About 5 to 8 cm distal to the lateral epicondyle, the anterior interosseous nerve (a purely motor nerve) branches off the median nerve. It travels deep to the median nerve between the flexor pollicis longus and flexor digitorum profundus (both of which it innervates). The palmar cutaneous branch of the median nerve arises 5 cm proximal to the wrist crease on the radial side of the nerve.2,3
Suggested Technique
With ultrasound, the median nerve is usually blocked in the mid-forearm because it is echobright without adjacent tendons.1 This location is also chosen because it is away from the carpal tunnel, proximal to the palmar cutaneous branch takeoff, but distal to the anterior interosseous motor branch takeoff. In the mid-forearm, the median nerve lies within the fascial plane between the flexor digitorum superficialis and profundus, which provides a means for targeting drug injections without nerve contact. The block is performed on the volar side of the forearm with the arm supinated. Both in-plane and out-of-plane approaches can be used for these blocks. Steep in-plane approach to the median nerve from the lateral aspect of the forearm avoids the radial artery and the superficial radial nerve.
The hand should be relaxed so that the median nerve is mobile and not under tension. Wrist hyperextension stretches the median nerve and can lead to impairment of nerve function if prolonged.4 Therefore, median nerve block should be performed with the wrist in neutral position.
Near the elbow the median nerve lies medial to the brachial artery. Median nerve block proximal to the elbow is often used in the recovery room following surgery because of the presence of surgical dressings covering the forearm. If this approach is used, care must be taken to avoid puncturing the brachial artery because this can result in median epineurial hematoma.5,6
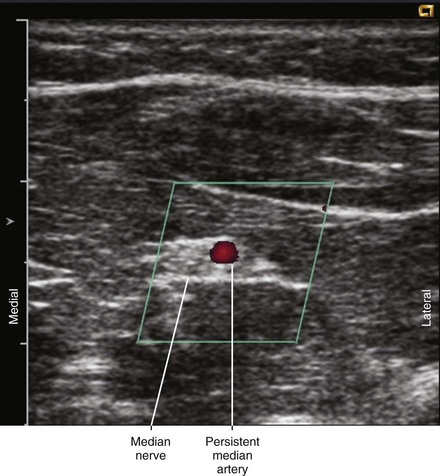
Although the median artery normally evolutes during development, persistent median artery can be detected with high-resolution ultrasound in about 25% of asymptomatic individuals.7 Persistent median artery is sometimes associated with high division or bifid median nerve, in which cases the artery is often in the middle of the divided nerve. When the persistent median artery is eccentrically located with respect to the nerve, the block should target the nonarterial side of the nerve to avoid intraneural hematoma.
Neurologic Assessment
Key Points
| Median Nerve Block | The Essentials |
|---|---|
| Anatomy | The MN lies between the FDS and FDP in the mid-forearm. |
| The MN is about 3 mm in diameter. | |
| Positioning | Arm supinated |
| Operator | Standing on the lateral (cephalad) side of the armboard |
| Display | Across the armboard |
| Transducer | High-frequency linear, 23- to 38-mm footprint |
| Initial depth setting | 25 mm |
| Needle | 25 gauge, 38 mm in length |
| Anatomic location | Mid-forearm on the volar surface |
| Approach | SAX view of MN, in-plane from lateral to medial |
| Place the needle tip between the FDS and FDP at the lateral corner of the MN. | |
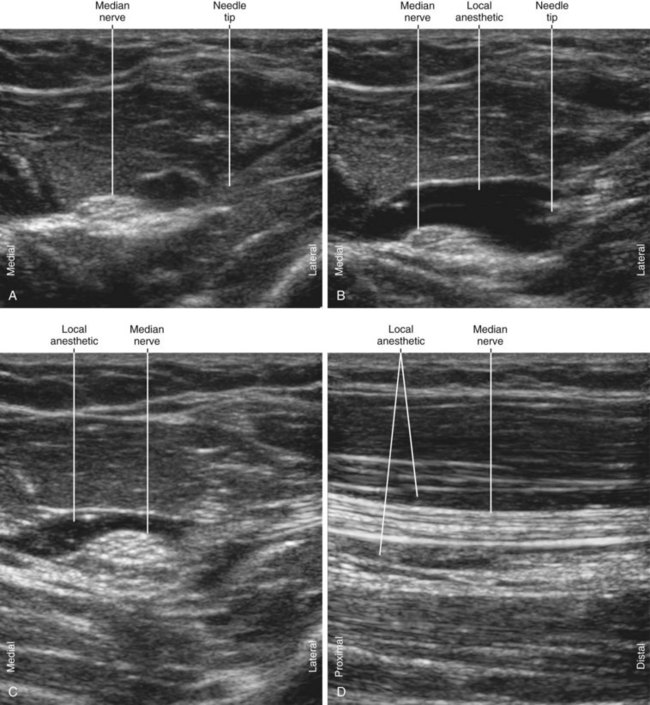
| Sonographic assessment | The injection should track distally along the MN to its palmar cutaneous branch. |
| Anatomic variation | Persistent median artery (PMA, 25%) |
| Bifid median nerve (5%) | |
| These two anomalies are associated with each other. | |
| A PMA can divide a bifid median nerve. |

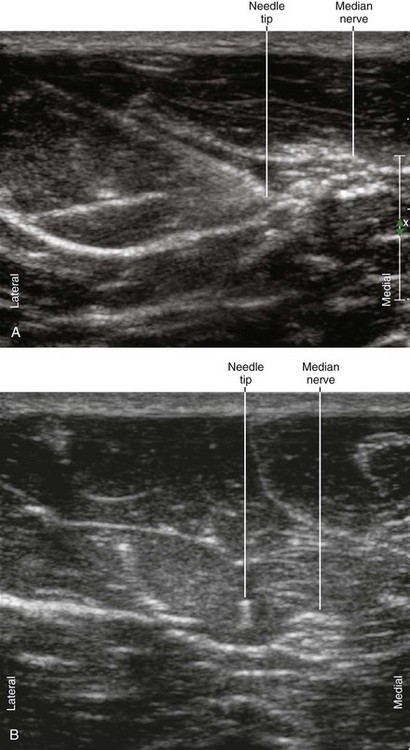
FIGURE 36-2 Sonograms illustrating the in-plane (A) and out-of-plane (B) approaches to median nerve block.
1 Jamadar DA, Jacobson JA, Hayes CW. Sonographic evaluation of the median nerve at the wrist. J Ultrasound Med. 2001;20:1011–1014.
2 Bezerra AJ, Carvalho VC, Nucci A. An anatomical study of the palmar cutaneous branch of the median nerve. Surg Radiol Anat. 1986;8:183–188.
3 Tagliafico A, Pugliese F, Bianchi S, et al. High-resolution sonography of the palmar cutaneous branch of the median nerve. AJR Am J Roentgenol. 2008;191:107–114.
4 Chowet AL, Lopez JR, Brock-Utne JG, et al. Wrist hyperextension leads to median nerve conduction block: implications for intra-arterial catheter placement. Anesthesiology. 2004;100:287–291.
5 Macon WL, 4th., Futrell JW. Median-nerve neuropathy after percutaneous puncture of the brachial artery in patients receiving anticoagulants. N Engl J Med. 1973;288:1396.
6 Chuang YM, Luo CB, Chou YH, et al. Sonographic diagnosis and treatment of a median nerve epineural hematoma caused by brachial artery catheterization. J Ultrasound Med. 2002;21:705–708.
7 Gassner EM, Schocke M, Peer S, et al. Persistent median artery in the carpal tunnel: color Doppler ultrasonographic findings. J Ultrasound Med. 2002;21:455–461.