Bladder Masses
Synonyms/Description
Etiology
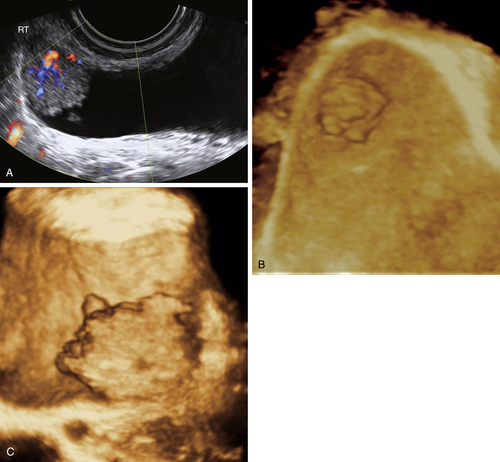
Transitional Cell Cancer
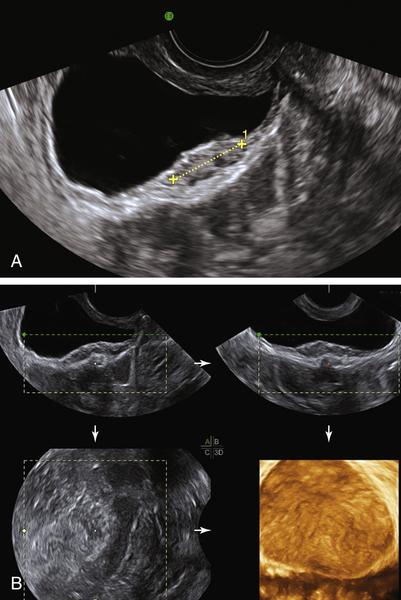
Fibroma
Endometriosis
Diffuse Bladder Wall Thickening
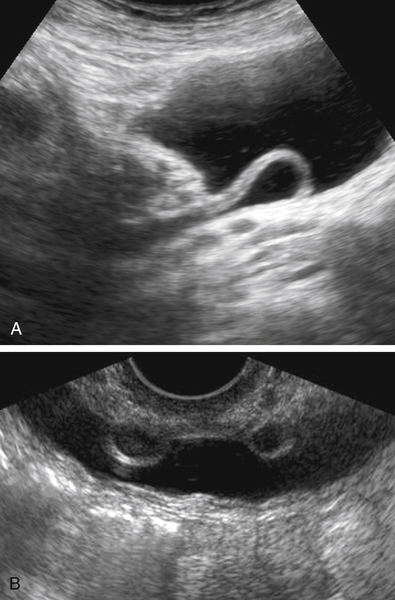
Findings Specifically Related to the Ureteral Orifice
Urethral Diverticula
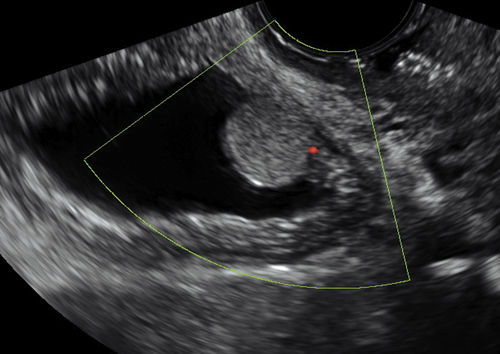
Other Bladder Masses
Ultrasound Findings
Differential Diagnosis
Clinical Aspects and Recommendations
Figures

Suggested Reading
Fasih N., Prasad Shanbhogue A.K., Macdonald D.B., Fraser-Hill M.A., Papadatos D., Kielar A.Z., Doherty G.P., Walsh C., McInnes M., Atri M. Leiomyomas beyond the uterus: unusual locations, rare manifestations. Radiographics. 2008;28:1931–1948 Review.
Kocakoc E., Kiris A., Orhan I., Poyraz A.K., Artas H., Firdolas F. Detection of bladder tumors with 3-dimensional sonography and virtual sonographic cystoscopy. J Ultrasound Med. 2008;27:45–53.
Wong-You-Cheong J.J., Woodward P.J., Manning M.A., Davis C.J. From the archives of the AFIP: inflammatory and nonneoplastic bladder masses: radiologic-pathologic correlation. Radiographics. 2006;26:1847–1868 Review.
Wong-You-Cheong J.J., Woodward P.J., Manning M.A., Sesterhenn I.A. From the archives of the AFIP: neoplasms of the urinary bladder: radiologic-pathologic correlation. Radiographics. 2006;26:553–580 Review.






