Chapter 17 Managing Pediatric and Neonatal Abdominal Wall Defects 
1 Clinical Anatomy
 In a patient with an omphalocele (also known as exomphalos) (Fig.17-1), the bowel and viscera, covered by a membrane composed of visceral peritoneum, Wharton jelly, and amnion, herniate through a central defect (≥4 cm) at the umbilical ring. The viscera extend into the base of the umbilical cord and the umbilical cord inserts into the apex of the omphalocele sac. The sac may contain loops of small bowel, large intestine, stomach, and liver (in 50% of cases). These viscera are otherwise functionally normal.
In a patient with an omphalocele (also known as exomphalos) (Fig.17-1), the bowel and viscera, covered by a membrane composed of visceral peritoneum, Wharton jelly, and amnion, herniate through a central defect (≥4 cm) at the umbilical ring. The viscera extend into the base of the umbilical cord and the umbilical cord inserts into the apex of the omphalocele sac. The sac may contain loops of small bowel, large intestine, stomach, and liver (in 50% of cases). These viscera are otherwise functionally normal.
 In patients with gastroschisis (Fig.17-2), the small bowel freely protrudes, without an overlying sac, through a smaller defect (<4 cm) at the junction between the umbilicus and the skin. The defect is almost always to the right of the umbilicus. The herniated contents may include small bowel, stomach, bladder, fallopian tubes, ovaries, and testes.
In patients with gastroschisis (Fig.17-2), the small bowel freely protrudes, without an overlying sac, through a smaller defect (<4 cm) at the junction between the umbilicus and the skin. The defect is almost always to the right of the umbilicus. The herniated contents may include small bowel, stomach, bladder, fallopian tubes, ovaries, and testes.



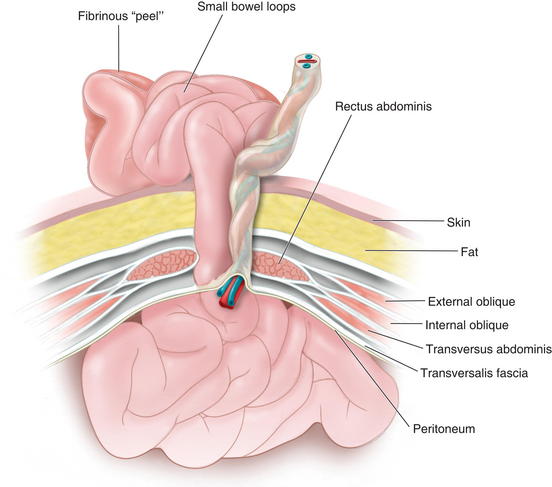
 In gastroschisis, due to exposure to amniotic fluid and compromised blood supply, the small bowel may become thick, shortened, edematous, discolored, and covered with fibrinous exudates (also known as a “peel”). This may reduce the malleability of the bowel and make manual reduction more difficult. Furthermore, extensive peel is thought to lead to a prolonged ileus after bowel reduction.
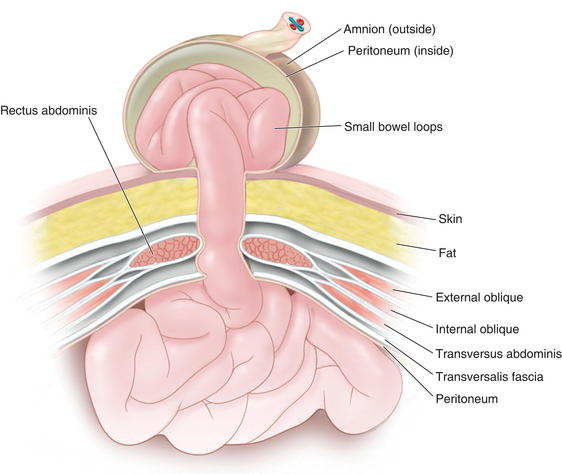
In gastroschisis, due to exposure to amniotic fluid and compromised blood supply, the small bowel may become thick, shortened, edematous, discolored, and covered with fibrinous exudates (also known as a “peel”). This may reduce the malleability of the bowel and make manual reduction more difficult. Furthermore, extensive peel is thought to lead to a prolonged ileus after bowel reduction. Omphalocele is due to the primary failure of the developing intestines to return to the abdominal cavity after migration into the umbilical cord during weeks 6 to 12 of gestation. Figure 17-3 depicts a cross-sectional diagram of the anatomy seen in omphalocele. The abdominal muscles are otherwise normally developed.
Omphalocele is due to the primary failure of the developing intestines to return to the abdominal cavity after migration into the umbilical cord during weeks 6 to 12 of gestation. Figure 17-3 depicts a cross-sectional diagram of the anatomy seen in omphalocele. The abdominal muscles are otherwise normally developed. Gastroschisis is believed to be caused by involution of the right umbilical vein during the fourth week of development. The resulting ischemia leads to a full-thickness defect in the musculature of the abdominal wall. Figure 17-4 shows a cross-sectional diagram of the anatomy seen in gastroschisis.
Gastroschisis is believed to be caused by involution of the right umbilical vein during the fourth week of development. The resulting ischemia leads to a full-thickness defect in the musculature of the abdominal wall. Figure 17-4 shows a cross-sectional diagram of the anatomy seen in gastroschisis.

2 Preoperative Considerations
 Both omphalocele and gastroschisis may be suspected prenatally with an elevated maternal serum α-fetoprotein (although this level can be normal or elevated because of other conditions) and can be diagnosed readily by prenatal ultrasonography in 75% to 80% of cases (after 14 weeks’ gestation when the fetal midgut returns to the abdomen). They can be differentiated sonographically by the presence of a sac, location of the defect, and presence of additional abnormalities. These methods have increasingly led to detection before birth and allow for prenatal education and family counseling.
Both omphalocele and gastroschisis may be suspected prenatally with an elevated maternal serum α-fetoprotein (although this level can be normal or elevated because of other conditions) and can be diagnosed readily by prenatal ultrasonography in 75% to 80% of cases (after 14 weeks’ gestation when the fetal midgut returns to the abdomen). They can be differentiated sonographically by the presence of a sac, location of the defect, and presence of additional abnormalities. These methods have increasingly led to detection before birth and allow for prenatal education and family counseling.


 With omphalocele, patients can undergo primary closure, staged closure, or nonoperative management with late closure. Those with gastroschisis may similarly undergo primary closure, or, if the abdominal cavity is too small to accommodate the protuberant bowel, staged closure. Infants with gastroschisis also may be able to undergo the recently developed sutureless repair.
With omphalocele, patients can undergo primary closure, staged closure, or nonoperative management with late closure. Those with gastroschisis may similarly undergo primary closure, or, if the abdominal cavity is too small to accommodate the protuberant bowel, staged closure. Infants with gastroschisis also may be able to undergo the recently developed sutureless repair.3 Operative Steps
1 Omphalocele
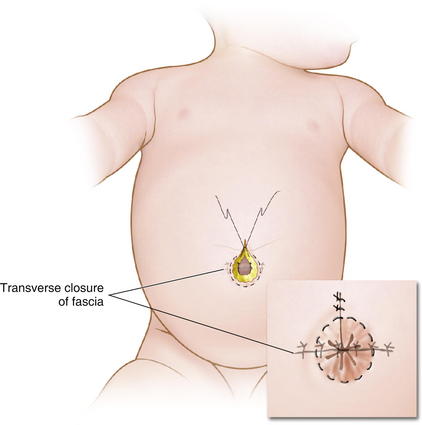
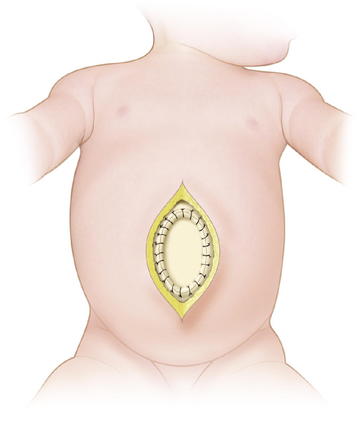
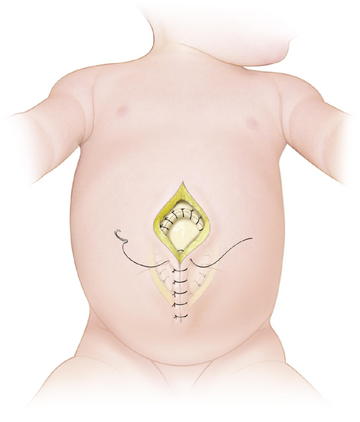
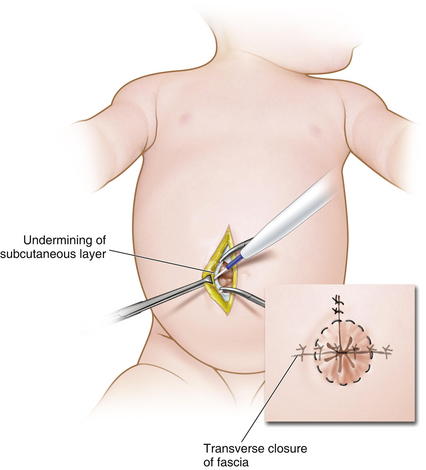
 When possible, primary closure should be performed. This is sometimes possible for small or moderately sized defects. The omphalocele sac is excised (Fig.17-5). The umbilical arteries and vein are identified and ligated. The skin is then undermined enough for a secure fascial closure. The viscera are reduced. And the fascia is closed, usually in a transverse fashion. The skin often can be closed using a purse-string suture to try to recreate an umbilicus (Fig.17-6).
When possible, primary closure should be performed. This is sometimes possible for small or moderately sized defects. The omphalocele sac is excised (Fig.17-5). The umbilical arteries and vein are identified and ligated. The skin is then undermined enough for a secure fascial closure. The viscera are reduced. And the fascia is closed, usually in a transverse fashion. The skin often can be closed using a purse-string suture to try to recreate an umbilicus (Fig.17-6).
 For the Gross technique, developed in 1948, the omphalocele sac is excised. The skin is undermined enough to provide minimal tension. Prosthetic material may be needed to bridge the fascial defect (Fig.17-7). The skin is then closed over the defect (Fig.17-8). The resulting ventral hernia is then repaired at a later time. In recent years, many surgeons who use this approach are using biologic mesh material for closure.
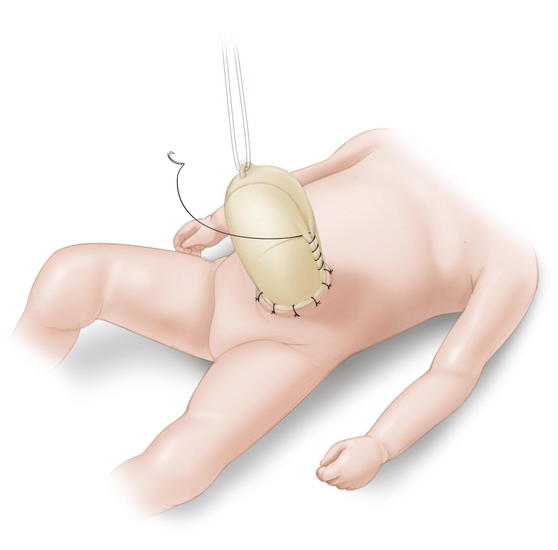
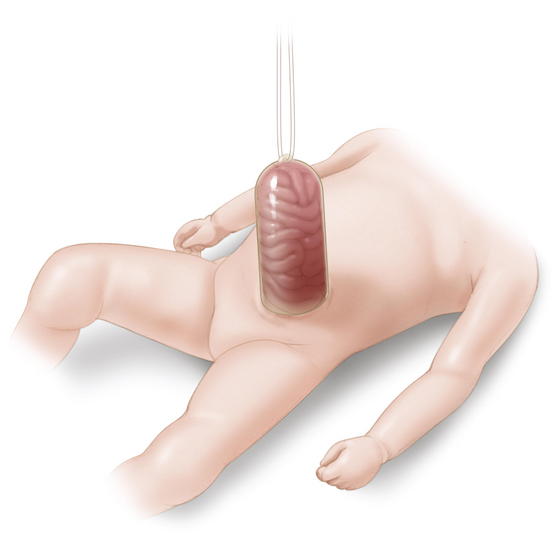
For the Gross technique, developed in 1948, the omphalocele sac is excised. The skin is undermined enough to provide minimal tension. Prosthetic material may be needed to bridge the fascial defect (Fig.17-7). The skin is then closed over the defect (Fig.17-8). The resulting ventral hernia is then repaired at a later time. In recent years, many surgeons who use this approach are using biologic mesh material for closure. The Schuster technique, developed in 1967, is particularly useful for large or ruptured omphaloceles. This technique involves using a silo to gradually reduce the herniated viscera over several days to a week. As much of the viscera as possible are returned to the abdomen. A nonabsorbable material such as silastic sheeting can be used as a silo, secured to either the fascia or skin with nonabsorbable suture. The silo is then closed over the top of the viscera and suspended perpendicularly to avoid kinks in the intestine, allowing gravity to pull the viscera back into the abdomen (Fig.17-9). The silo is tightened daily to assist in visceral reduction. Once the viscera are reduced within the abdominal cavity, the silo is removed and the fascia and skin are closed.
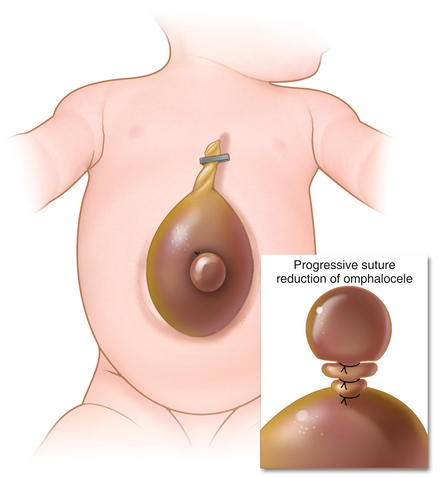
The Schuster technique, developed in 1967, is particularly useful for large or ruptured omphaloceles. This technique involves using a silo to gradually reduce the herniated viscera over several days to a week. As much of the viscera as possible are returned to the abdomen. A nonabsorbable material such as silastic sheeting can be used as a silo, secured to either the fascia or skin with nonabsorbable suture. The silo is then closed over the top of the viscera and suspended perpendicularly to avoid kinks in the intestine, allowing gravity to pull the viscera back into the abdomen (Fig.17-9). The silo is tightened daily to assist in visceral reduction. Once the viscera are reduced within the abdominal cavity, the silo is removed and the fascia and skin are closed. Sequential sac ligation is when the natural omphalocele sac itself is used as a silo. It requires a sac that is strong and not adherent to the viscera. Traction is applied to the sac to slowly reduce its contents. As the viscera are reduced into the abdominal cavity, the sac is twisted and ligated with umbilical ties (Fig.17-10).
Sequential sac ligation is when the natural omphalocele sac itself is used as a silo. It requires a sac that is strong and not adherent to the viscera. Traction is applied to the sac to slowly reduce its contents. As the viscera are reduced into the abdominal cavity, the sac is twisted and ligated with umbilical ties (Fig.17-10).
 Nonoperative (escharotic) therapy is an option for those patients who are not good candidates for surgical intervention (premature, chromosomal abnormalities, significant congenital heart disease, or pulmonary hypoplasia) and the author’s preferred option for giant omphaloceles. The omphalocele sac is painted with an escharotic material, such as silver sulfadiazine. The authors have also used an Aquacel dressing (ConvaTec, Skillman, NJ) for this purpose. These materials prevent infection, form granulation tissue, and allow the sac surface to eventually epithelialize and contract over several months. The resulting ventral hernia is then electively repaired once the underlying cardiac, pulmonary, and/or other conditions have improved.
Nonoperative (escharotic) therapy is an option for those patients who are not good candidates for surgical intervention (premature, chromosomal abnormalities, significant congenital heart disease, or pulmonary hypoplasia) and the author’s preferred option for giant omphaloceles. The omphalocele sac is painted with an escharotic material, such as silver sulfadiazine. The authors have also used an Aquacel dressing (ConvaTec, Skillman, NJ) for this purpose. These materials prevent infection, form granulation tissue, and allow the sac surface to eventually epithelialize and contract over several months. The resulting ventral hernia is then electively repaired once the underlying cardiac, pulmonary, and/or other conditions have improved.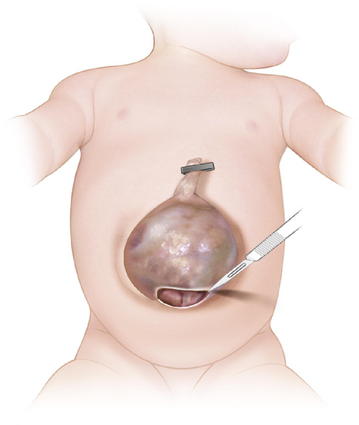
2 Gastroschisis
 Primary closure of gastroschisis is possible in a majority of cases. Muscle relaxation is often used to assist with visceral reduction. Also, decompression of the stomach or bowel may aid in reducing the volume of the intestines. It may be difficult to reduce the herniated contents through a small defect, and thus, the neck of the defect may need to be enlarged superiorly (Fig.17-11). The bowel must be examined for possible atresias or perforations. The skin is then undermined enough to provide a secure closure. Because the risk of subsequent umbilical hernia is high after gastroschisis repair, the fascia lateral to the umbilical ring should be identified and used for placement of the suture (Fig.17-12). Care must be taken to avoid abdominal compartment syndrome by putting too much pressure on the reduced intestines. If atresia is noted, the bowel is reduced at the first operation and a second operation is done 4 to 6 weeks later to correct the atresia as the intraabdominal inflammation resolves.
Primary closure of gastroschisis is possible in a majority of cases. Muscle relaxation is often used to assist with visceral reduction. Also, decompression of the stomach or bowel may aid in reducing the volume of the intestines. It may be difficult to reduce the herniated contents through a small defect, and thus, the neck of the defect may need to be enlarged superiorly (Fig.17-11). The bowel must be examined for possible atresias or perforations. The skin is then undermined enough to provide a secure closure. Because the risk of subsequent umbilical hernia is high after gastroschisis repair, the fascia lateral to the umbilical ring should be identified and used for placement of the suture (Fig.17-12). Care must be taken to avoid abdominal compartment syndrome by putting too much pressure on the reduced intestines. If atresia is noted, the bowel is reduced at the first operation and a second operation is done 4 to 6 weeks later to correct the atresia as the intraabdominal inflammation resolves. As with omphalocele, staged closure, can be used when reducing the herniated viscera is too difficult or produces too much intraabdominal pressure. A silo is used to gradually reduce the bowel by decreasing the swelling and rigidity of the inflamed bowel and progressively stretching the abdominal cavity. The silo also prevents electrolyte, fluid, and heat losses. Recently, preformed spring-loaded silos that can be placed at the bedside without sutures or anesthesia have shown to be associated with fewer ventilator days, more rapid return of bowel function, and fewer complications (Fig.17-13).
As with omphalocele, staged closure, can be used when reducing the herniated viscera is too difficult or produces too much intraabdominal pressure. A silo is used to gradually reduce the bowel by decreasing the swelling and rigidity of the inflamed bowel and progressively stretching the abdominal cavity. The silo also prevents electrolyte, fluid, and heat losses. Recently, preformed spring-loaded silos that can be placed at the bedside without sutures or anesthesia have shown to be associated with fewer ventilator days, more rapid return of bowel function, and fewer complications (Fig.17-13). Sutureless repair, developed by Sandler et al. (2004), allows the defect to naturally heal over the reduced bowel. The bowel is first manually reduced into the abdominal cavity (Fig.17-14, A, B). The umbilical cord is wrapped into a coil over the defect. The area is covered with a 2 × 2 gauze sponge and Tegaderm dressing (3M, St. Paul, MN) and allowed to heal over several days (Fig.17-14, C, D). This type of repair uses no sutures, eliminates the need for a trip to the OR, and may be cosmetically superior to traditional surgical repair.
Sutureless repair, developed by Sandler et al. (2004), allows the defect to naturally heal over the reduced bowel. The bowel is first manually reduced into the abdominal cavity (Fig.17-14, A, B). The umbilical cord is wrapped into a coil over the defect. The area is covered with a 2 × 2 gauze sponge and Tegaderm dressing (3M, St. Paul, MN) and allowed to heal over several days (Fig.17-14, C, D). This type of repair uses no sutures, eliminates the need for a trip to the OR, and may be cosmetically superior to traditional surgical repair.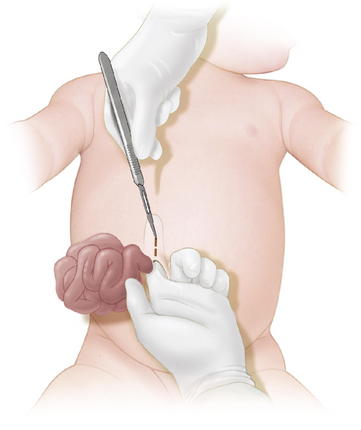




4 Postoperative Care
 Postoperative care requires the neonatal intensive care unit (NICU). Larger defects require mechanical ventilation for days to weeks. It is important to monitor for signs of abdominal compartment syndrome (hypotension, oliguria, acidosis, intestinal ischemia, liver dysfunction) with intragastric or intravesical catheters. The intraabdominal pressure should not be above 15 to 20 mm Hg.
Postoperative care requires the neonatal intensive care unit (NICU). Larger defects require mechanical ventilation for days to weeks. It is important to monitor for signs of abdominal compartment syndrome (hypotension, oliguria, acidosis, intestinal ischemia, liver dysfunction) with intragastric or intravesical catheters. The intraabdominal pressure should not be above 15 to 20 mm Hg.


 The long-term outcome for patients with gastroschisis has dramatically improved over the past few decades because of improved surgical technique and perioperative management, such as the use of staged closure and the availability of total parenteral nutrition. Overall mortality is now <10%, and is most often associated with intestinal atresia. Prognosis is most dependent on the condition of the exteriorized bowel. Those patients with intestinal atresia undergo additional surgical procedures, delayed enteral feedings, and have prolonged hospital stays.
The long-term outcome for patients with gastroschisis has dramatically improved over the past few decades because of improved surgical technique and perioperative management, such as the use of staged closure and the availability of total parenteral nutrition. Overall mortality is now <10%, and is most often associated with intestinal atresia. Prognosis is most dependent on the condition of the exteriorized bowel. Those patients with intestinal atresia undergo additional surgical procedures, delayed enteral feedings, and have prolonged hospital stays.5 Pearls/Pitfalls
 If a fetus is discovered to have an abdominal wall defect, there is no evidence to suggest that early delivery or cesarean-section is beneficial. The mode and timing of delivery should be determined by fetal well-being and obstetric considerations. Serial ultrasound exams during pregnancy can aid in evaluating the condition of the bowel and whether the fetus is at risk.
If a fetus is discovered to have an abdominal wall defect, there is no evidence to suggest that early delivery or cesarean-section is beneficial. The mode and timing of delivery should be determined by fetal well-being and obstetric considerations. Serial ultrasound exams during pregnancy can aid in evaluating the condition of the bowel and whether the fetus is at risk.


Aspelund G.L.J. Abdominal wall defects. Current Paediatrics. 2006:192-198.
Henrich K., Huemmer H.P., Reingruber B., Weber P.G. Gastroschisis and omphalocele: treatments and long-term outcomes. Pediatr Surg Int. 2008;24:167-173.
Langer J.C. Abdominal wall defects. World J Surg. 2003;27:117-124.
Ledbetter D.J. Gastroschisis and omphalocele. Surg Clin North Am. 2006;86:249-260. vii
Mann S., Blinman T.A., Douglas Wilson R. Prenatal and postnatal management of omphalocele. Prenat Diagn. 2008;28:626-632.
Molenaar J.C., Tibboel D. Gastroschisis and omphalocele. World J Surg. 1993;17:337-341.
Puri P.H.M., editor. Pediatric Surgery. Springer-Verlag Berlin Heidelberg, New York, NY, 2006;153-170.
Sandler A., Lawrence J., Meehan J., Phearman L., Soper R. J Pediatr Surg. 2004 May;39(5):738-741.
