CHAPTER 16 Malrotation
Ladd Procedure
Step 1: Surgical Anatomy
♦ The term malrotation describes several related abnormalities characterized by the failure of the intestine to assume its normal anatomic position.
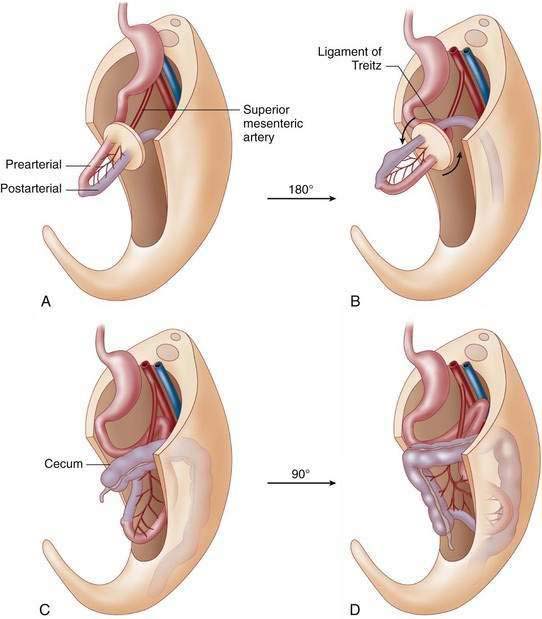
♦ The normal anatomic position of the intestine is achieved during the 10th week of gestation when the herniated intra-abdominal contents return to the abdominal cavity and begin a counterclockwise rotation about the superior mesenteric artery (Fig. 16-1).
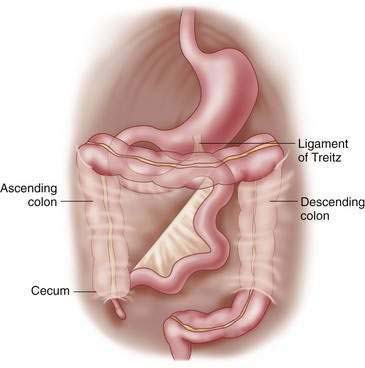
♦ The final result of this normal rotational process is a retroperitoneal duodenum with the ligament of Treitz in the left upper quadrant at or close to the level of the antrum of the stomach. The beginning of the small intestine (jejunum) is located to the left of midline in the left upper quadrant and the cecum fixed in the right lower quadrant. The mesentery of the normally fixed small intestine is broad based, extending from the left upper quadrant to the right lower quadrant of the abdomen and is at low risk for volvulus (Fig. 16-2).
Step 2: Preoperative Considerations
♦ The presentation of malrotation ranges from the acute onset of bilious emesis in the infant or child, feeding intolerance caused by duodenal obstruction, or an incidental finding on imaging studies.
♦ Bilious emesis in the neonate is a surgical emergency until proven otherwise and mandates an upper gastrointestinal evaluation with a contrast study regardless of findings on plain films. The diagnosis of volvulus in this setting is made by demonstration of obstruction with contrast tapering to a bird’s beak.
Step 3: Operative Steps
♦ In the case of the child with volvulus, adequate volume resuscitation should occur before the induction of general anesthesia.
♦ Prophylactic antibiotics for skin flora are adequate in the setting of an elective Ladd procedure; a broad-spectrum antibiotic should be given to the patient with volvulus.
♦ The infant or child is placed in the supine position, and a transverse right upper quadrant incision is made. The level of the incision is at the midway point between the subcostal margin and the umbilicus.
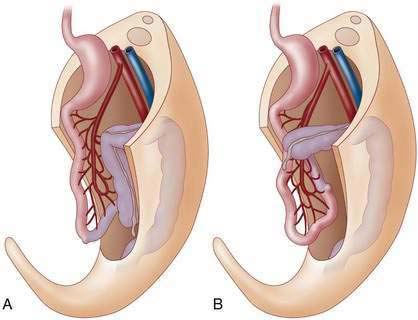
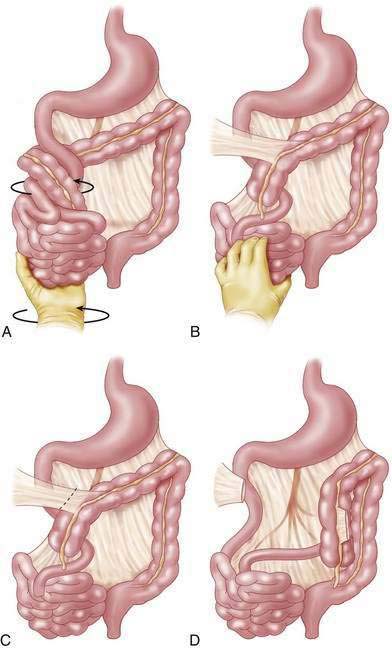
♦ The bowel is eviscerated and, if a volvulus is encountered, the intestine is rotated counterclockwise and inspected for evidence of ischemia (Fig. 16-4). If the bowel is not obviously necrotic, it should be covered with warm moistened laparotomy pads and re-examined after 10 to 15 minutes. Grossly necrotic bowel should be resected. If the remaining intestine is questionable, a second-look laparotomy is scheduled 24 to 48 hours later.
♦ A Ladd procedure is then performed by dividing the peritoneal attachments between the cecum and the retroperitoneum that overlies the duodenum, so called Ladd bands (see Fig. 16-4).
♦ The duodenum is then mobilized, followed by widening of the narrow small bowel mesentery to reduce the risk of volvulus (see Fig. 16-4).
♦ The mesoappendix is then taken using electrocautery in the infant or ties in the older child. The appendix itself is then inverted with a lacrimal probe and double-ligated with a 2-0 absorbable suture.
Step 4: Postoperative Care
♦ The infant or child with a volvulus and compromised bowel requires monitoring, nasogastric decompression, intravenous antibiotics, and further resuscitation in an intensive care setting.
♦ In the patient with questionable or a large amount of ischemic bowel, a second-look laparotomy is typically undertaken on postoperative day 1 or 2, and decisions then must be made with regard to further resection, stoma formation or, unfortunately, in some situations redirection of care when the insult is deemed incompatible with life.
Step 5: Pearls and Pitfalls
Aiken JJ, Oldham KT, Ashcraft KW, Holcomb GW, Murphy JP, editors. Pediatric surgery, 4th ed. 2005. Saunders Elsevier, Philadelphia:435-447
Spitz L, Bax NM, van der Zee DC. Malrotation. In: Spitz L, Arnold G, Coran AG, editors. Operative pediatric surgery. 6th ed. New York: Hodder Arnold; 2006:383-392.