[level-membership-for-radiology-category] Can occur in either superior lumbar triangle of Grynfeltt-Lesshaft or inferior lumbar triangle of Petit
– Superior lumbar triangle of Grynfeltt-Lesshaft defined by 12th rib superiorly, superior border of internal oblique inferiorly, and erector spinae medially
– Inferior lumbar triangle of Petit defined by latissimus dorsi muscle medially, iliac crest inferiorly, and free border of external oblique muscle laterally



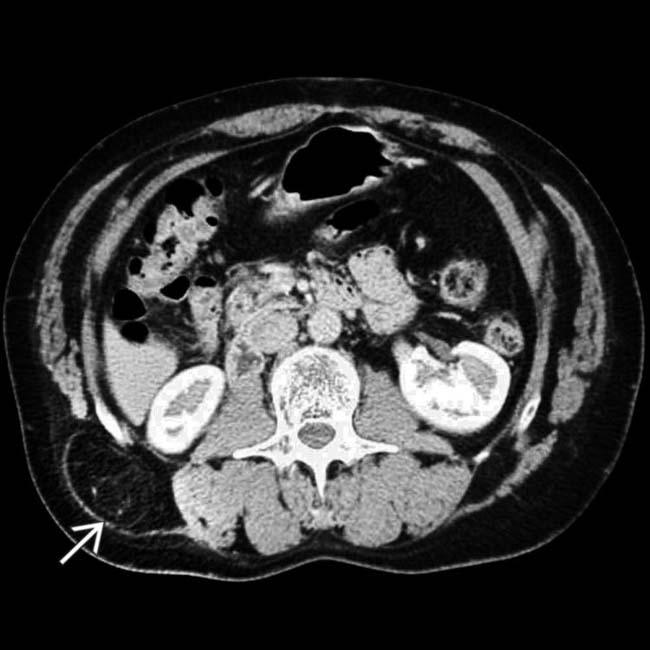
 in a patient with right flank discomfort.
in a patient with right flank discomfort.
 in the aponeurosis of the internal oblique and transverse abdominal muscles, which should insert on the thoracoabdominal fascia that envelops the quadratus lumborum and erector spinae muscles.
in the aponeurosis of the internal oblique and transverse abdominal muscles, which should insert on the thoracoabdominal fascia that envelops the quadratus lumborum and erector spinae muscles.
 in the left thoracolumbar fascia through which the descending colon
in the left thoracolumbar fascia through which the descending colon  herniates dorsally. The thoracolumbar fascia should be a strong sheet of tissue that inserts on the iliac crest.
herniates dorsally. The thoracolumbar fascia should be a strong sheet of tissue that inserts on the iliac crest.
 and colon
and colon  . Notice that while the liver is diffusely steatotic, the liver within the lumbar hernia is higher in density, probably as a result of differential perfusion due to entrapment in the hernia.
. Notice that while the liver is diffusely steatotic, the liver within the lumbar hernia is higher in density, probably as a result of differential perfusion due to entrapment in the hernia.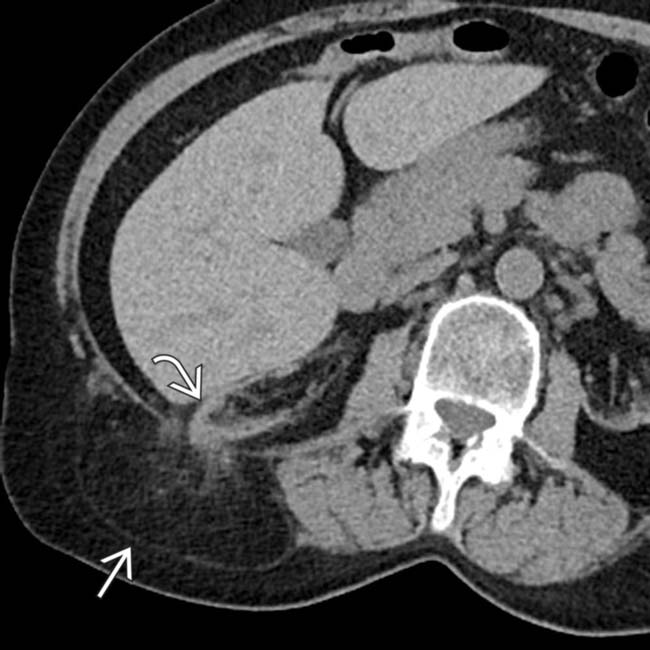
 with extension of the right kidney
with extension of the right kidney  into the hernia sac.
into the hernia sac.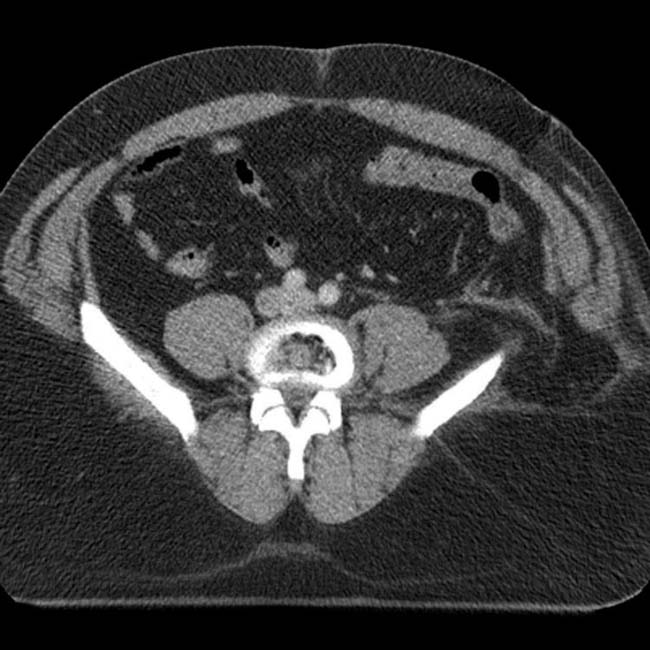
 . Post-traumatic lumbar hernias are rare but much more likely to be associated with strangulation or incarceration.
. Post-traumatic lumbar hernias are rare but much more likely to be associated with strangulation or incarceration.
 of the muscular and tendinous insertions of the abdominal wall muscles from the left iliac wing and thoracolumbar fascia, with creation of a post-traumatic lumbar hernia. Post-traumatic lumbar hernias are rare but much more likely to be associated with strangulation or incarceration.
of the muscular and tendinous insertions of the abdominal wall muscles from the left iliac wing and thoracolumbar fascia, with creation of a post-traumatic lumbar hernia. Post-traumatic lumbar hernias are rare but much more likely to be associated with strangulation or incarceration.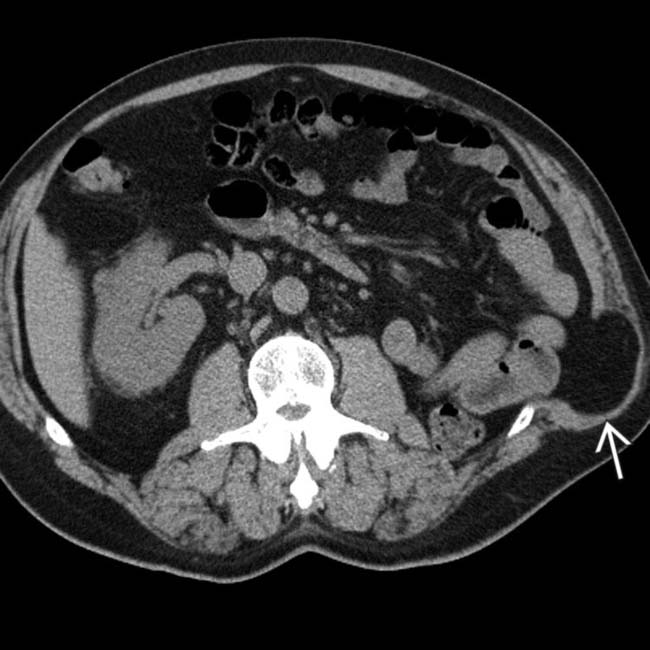
 of abdominal fat through the site of the incision. The hernia is covered mostly by the thin latissimus dorsi muscle. The defect, a variant of a lumbar hernia, is through the aponeuroses of the abdominal oblique and transverse muscles.
of abdominal fat through the site of the incision. The hernia is covered mostly by the thin latissimus dorsi muscle. The defect, a variant of a lumbar hernia, is through the aponeuroses of the abdominal oblique and transverse muscles.[/level-membership-for-radiology-category][not-level-membership-for-radiology-category] Can occur in either superior lumbar triangle of Grynfeltt-Lesshaft or inferior lumbar triangle of Petit
– Superior lumbar triangle of Grynfeltt-Lesshaft defined by 12th rib superiorly, superior border of internal oblique inferiorly, and erector spinae medially
– Inferior lumbar triangle of Petit defined by latissimus dorsi muscle medially, iliac crest inferiorly, and free border of external oblique muscle laterally
PATHOLOGY
• 80% of lumbar hernias are acquired
 Can be spontaneous (especially in older patients and patients with excessive weight loss) or secondary to trauma, infection, or previous surgery in flank
Can be spontaneous (especially in older patients and patients with excessive weight loss) or secondary to trauma, infection, or previous surgery in flank

Can be spontaneous (especially in older patients and patients with excessive weight loss) or secondary to trauma, infection, or previous surgery in flank
Buy Membership for Radiology Category to continue reading. Learn more here
[/not-level-membership-for-radiology-category]
