Chapter 16 Lower Limb Neuromuscular Control and Strength in Prepubescent and Adolescent Male and Female Athletes
INTRODUCTION
An estimated 30 million children aged 5 to 18 years participate in organized sports programs each year in the United States.1 Unfortunately, approximately one third of these athletes sustain injuries frequently in the ankle or knee that require medical treatment.1,47,62,78 Several studies have reported that female athletes have a four- to eightfold higher incidence of serious knee ligament injury than males participating in the same sport.4,15,36,51 The mechanisms responsible for the disparity between genders in knee ligament injury rates, especially in regard to the anterior cruciate ligament (ACL), are controversial and not scientificallydefined at present. Theories have included anatomic variations, environmental influences, hormonal fluctuations, and genetic factors.34 Investigators have described gender differences in neuromuscular indices including muscle strength, running, cutting, sidestepping, and landing characteristics in adolescent and adult populations that are believed to be at least partially responsible for the differences in knee ligament injury rates.*
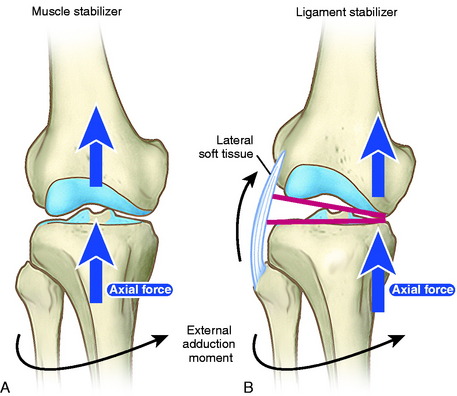
A valgus lower limb alignment commonly occurs during noncontact ACL injuries, when an athlete either lands from a jump or attempts to accelerate into a jump.11,28,30 Scientists have reported significant differences between genders in knee and hip flexion angles44 and ground reaction forces placed on the lower extremity upon landing.42,57,68,69,76 Experimental studies show that, in a cadaver model, a valgus torque combined with an anterior tibial force results in statistically significant larger strain in the ACL than that produced from an anterior tibial force alone (P < .0001).10 Markolf and coworkers54 measured in vitro forces in the ACL during isolated and combined loading states in cadaver knees. Increases in ACL forces occurred when a valgus or varus moment was applied with an anterior tibial load compared with those measured when an anterior tibial load only was applied. In addition, high valgus or varus moments increase the risk for medial or lateral tibiofemoral joint lift-off and the potential for a knee ligament rupture (Fig. 16-1).54 It is unknown whether one can extrapolate these laboratory findings to an increased risk of ACL injury when an athlete lands or collapses into a valgus position, with little distance separating the right and the left knee.
This chapter summarizes a series of four studies conducted by the authors that measured the effects of chronological age and gender in athletes 9 to 17 years of age on isokinetic lower extremity strength, lower limb alignment during a drop-jump test, and lower limb symmetry during single-leg-hop tests. The ages for the hypotheses developed for the studies were based on the mean time to achieve peak height velocity (mean, 11.5 yr for girls and 13.5 yr for boys88) and skeletal maturity (mean, 13.3 yr for girls and 14.3 yr for boys3). All studies were approved by a local hospital’s institutional review board.
NEUROMUSCULAR TESTING METHODS
The goal of the SIT was to collect data on a large number of young athletes that included
Videographic Drop-Jump Screening Test
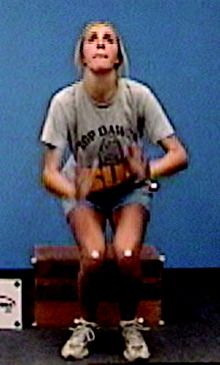
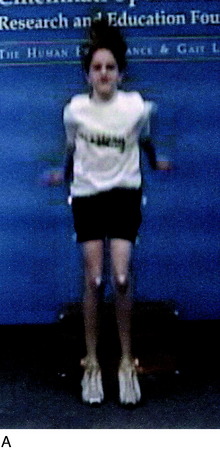
A drop-jump videographic screening test was developed as described in detail previously.65 Minimal equipment is required and the software is available from the authors’ nonprofit foundation. A camcorder equipped with a memory stick is placed on a stand 102.24 cm (40.25 inches) in height. The stand is positioned approximately 365.76 cm (12 ft) in front of a box 30.48 cm (12 inches) inheight and 38.1 cm (15 inches) in width. One-inch Velcro circles are placed on each of the four corners of the box that faces the camera. Athletes wear fitted, dark shorts and low-cut gym shoes. Reflective markers are placed at the greater trochanter and the lateral malleolus of both the right and the left legs, and Velcro circles are placed on the center of each patella. A research assistant demonstrates the jump-land sequence, and one practice trial is done to ensure the athlete understands the test. No verbal instruction regarding how to land or jump is provided. Athletes are told only to land straight in front of the box to be in the correct angle for the camera to record properly. The athletes perform a jump-land sequence by first jumping off the box, landing, and immediately performing a maximum vertical jump. This sequence is repeated three times.
Critical Points NEUROMUSCULAR TESTING METHODS
Sports injury test done on 1140 athletes (916 female, 224 male) 9–17 yr of age.
Videographic Drop-Jump Screening Test
Isokinetic Evaluation of Knee Extensor and Flexor Strength
The absolute centimeters of separation distance between the right and the left hip and normalized separation distances for the knees and ankles, standardized according to the hip separation distance, are analyzed. Normalized knee separation distance is calculated as knee separation distance divided by hip separation distance and normalized ankle separation distance is calculated as ankle separation distance divided by hip separation distance (Fig. 16-2).
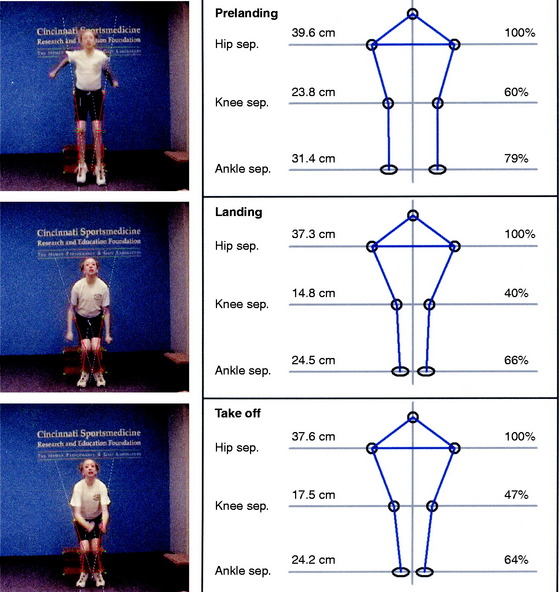
The reliability of the drop-jump videographic test was determined in 17 female athletes who underwent the test twice, 7 weeks apart.65 The reliability of the absolute centimeters of hip separation distances was evaluated. Hip separation distance was expected to be highly reliable, thus providing the basis for normalization of knee and ankle separation distances. Then, in 10 other subjects, reliability within the videographic test was assessed by capturing two of the three jump-land sequence trials and comparing the absolute centimeters of hip, knee, and ankle separation distances between the two sequences on the same day of testing. For the test-retest trial, the intraclass correlation coefficients (ICC) for the hip separation distance demonstrated high reliability (pre-land, .96; land, .94; take-off, .94). For the within-test trial, the ICC for the hip, knee, and ankle separation distance were all .90 or higher, demonstrating excellent reliability of the videographic test and software capturing procedures.
Isokinetic Evaluation of Knee Extensor and Flexor Strength
Isokinetic knee extensor and flexor testing was conducted (concentric mode) at 300°/sec (Fig. 16-3) in athletes over the age of 11 years. For the children who were 9 to 10 years of age, this test was performed at 180°/sec. Other investigators have reported acceptable reliability of isokinetic measurements in children and adults at these test velocities.48,58,60 The athletes first completed a dynamic warm-up session that lasted 5 minutes. They were then positioned in the chair of the device with appropriate torso, pelvis, and thigh straps placed according to the manufacturer’s protocol. The lever arm of the dynamometer was aligned with the lateral epicondyle of the knee, with the knee flexed to 90°. The chair was adjusted for each athlete as required to ensure proper positioning. The range of motion during the test was fixed from 90° to 0°. Gravitational factors were calculated by the dynamometer and automatically compensated for during the tests. The athletes performed three to four submaximal trials to become familiar with the machine and test velocity. A total of 10 repetitions were completed and the highest peak torque value used for analyses. Mean peak torque values (in Newton-meters [Nm]) were normalized for body weight (BW) in kilograms. Verbal encouragement was given throughout the tests, because the athletes were told to kick as hard and as fast as possible, but no visual feedback was available.

Isokinetic Evaluation of Internal and External Tibial Rotation Strength
An isokinetic assessment of knee internal tibial rotation (IR) and external tibial rotation (ER) strength was conducted on a calibrated Biodex System 3 (Biodex Medical Systems, Inc., Shirley, NY). The IR and ER peak torques of each limb were obtained at 120°/sec and 180°/sec. Testing was preceded by a dynamic warm-up that lasted approximately 5 minutes. The patients were positioned in the device in a partial supine position with the hip flexed 60° and the knee flexed 90° as described by Hester and Falkel (Fig. 16-4).39 Appropriate torso, pelvis, and thigh straps were placed according to the manufacturer’s protocol. In addition, the foot and ankle were tightly secured to a footplate using Velcro (VELCRO USA, Manchester, NH) straps.39 The athletes were instructed to relax so that the neutral position with regard to tibial rotation and the range of internal and external tibial motion could be obtained.72,89 Five submaximal repetitions were done before each test to promote familiarization with the dynamometer velocity speeds and to set the range of motion limits for both IR and ER.


There were 2-minute rest periods between the two velocity speed tests. The testing sequence of the dominant and nondominant limbs was randomized among the subjects. Verbal encouragement was given throughout the tests, because the athletes were told to rotate their lower leg through full range with maximal effort, but no visual feedback was available. A total of eight repetitions were completed at each speed and the single highest peak torque value used for analyses. Peak torque values were normalized for BW in kilograms and were expressed as (Nm/BW). Time-to-peak torque was measured in milliseconds (msec). The ratio of the mean peak torque of IR was calculated relative to that of ER (ratio IE = IR/ER × 100) in a manner described by Segawa and associates.82 The ratio of the mean peak torque of both IR and ER were also calculated relative to that of knee flexion. The ratio IR-F was calculated as IR/flexion × 100, and the ratio ER-F was calculated as ER/flexion × 100. The ratio of the mean peak torque of IR (IR-E) and ER (ER-E) were also calculated relative to that of knee extension in a manner similar to that described for knee flexion.
Single-Leg Functional Hop Testing
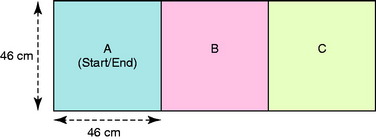
Two single-leg functional hop tests were conducted: a timed side-hop and a crossover hop for distance. The athletes were provided with instructions and one practice trial was conducted for each test. In the timed side-hop test, a course was created on the floor using masking tape to mark three boxes that were 46 × 46 cm (Fig. 16-5).7 The athletes were encouraged to hop as fast as possible, but to maintain balance to be able to complete the test. If the athlete did not clear the lines, double-bounced between hops, or could not hold balance on landing, a zero was recorded. Two tests were completed for each limb, with mean times calculated with a standard stopwatch to the nearest .01 sec.
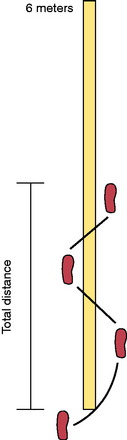
In the crossover hop for distance test, a marking strip made of masking tape was placed on the floor that extended approximately 6 m (Fig. 16-6).63 The athletes hopped three consecutive times on one foot, crossing diagonally over the tape on each hop. They were encouraged to go as far as possible while maintaining balance and control. The total distance hopped was measured and each leg tested twice, with the average distance calculated. The reliability of this test has been reported by other investigators to be excellent.5,12,29
Limb symmetry was calculated for each test by dividing the mean of the right limb by the mean of the left limb andmultiplying the result by 100. Prior studies on populations aged 17 to 34 reported that less than 85% limb symmetry on single-leg-hop tests was abnormal and representative of a general lower limb functional limitation.6,63
STUDY #1: VIDEOGRAPHIC DROP-JUMP SCREENING TEST
In this investigation, 325 female and 130 male athletes aged 11 to 19 underwent the videographic drop-jump screening test.65 A neuromuscular-training program40,42 (Sportsmetrics) was completed by 62 of the females; their jump-landing characteristics were reexamined within 1 week of the final training session. This subgroup also underwent an isokinetic evaluation of knee extensor and flexor strength before and after the neuromuscular-training program. The training sessions, described in detail in Chapter 19, Decreasing the Risk of ACL Injuries in Female Athletes, lasted approximately 1 hr/day, 3 days a week on alternating days and consisted of stretching, plyometric jump-training, and weight training under the supervision of a certified instructor. Participation in the training program was strictly voluntary and no attempt was made to influence certain individuals over others to complete the training with respect to the results of the initial videographic tests. Power and sample-size calculations were done to evaluate the primary study findings, the effect of training on absolute knee separation distance and normalized knee separation distance. With 62 trained females, it was found that this investigation had sufficient power (90%) to detect significant differences at a level of 0.05.
Hypothesis #1: Female Athletes Have an Overall Lower Limb Valgus Alignment, Indicated by Abnormally Decreased Knee Separation Distances, on Landing and Acceleration into a Vertical Jump on a Videographic Drop-Jump Test
The hypothesis was supported, because a marked overall lower limb valgus alignment (indicated by a knee separation distance of ≤ 60%) was found in 63% of the female athletes on landing (Fig. 16-7) and in 80% on take-off.
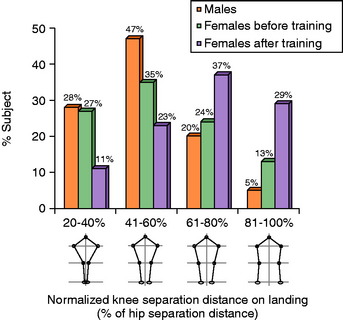
Hypothesis #2: Male Athletes Have a More Neutrally Aligned Lower Limb Position, with a Greater Amount of Separation Distance between the Knees, on Landing and Acceleration into a Vertical Jump Compared with Females on a Drop-Jump Test
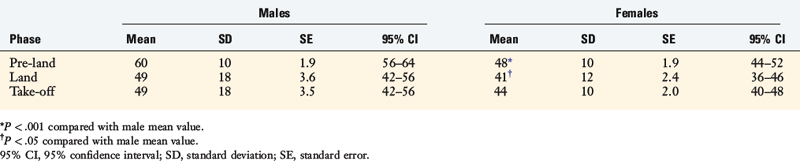
The hypothesis was not supported, as a marked overall lower limb valgus alignment was found in 75% of the male athletes on landing (see Fig. 16-7) and in 72% on take-off. There was no statistically significant difference between male and female athletes in the mean normalized knee and ankle separation distance during the landing and take-off phases. The female athletes had significantly higher mean normalized knee and ankle separation distances during the pre-land phase only.
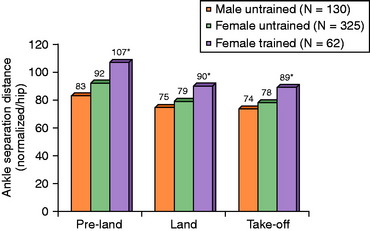
The normalized knee separation distances for both genders are shown in FIGURE 16-8, the normalized ankle separation distances are shown in FIGURE 16-9, and the absolute values for the hip, knee, and ankle separation distances are shown in Table 16-1. There were no correlations between knee and ankle separation distances for each phase of the jump-land sequence in either the female or the male athletes.
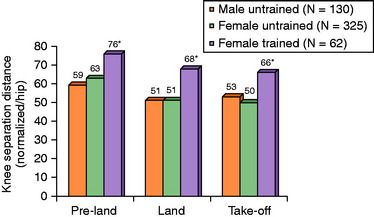

Hypothesis #3: A Neuromuscular-Training Program Will Produce Significantly Greater Knee Separation Distance in Female Athletes, thereby Producing a More Neutrally Aligned Lower Limb Position on a Drop-Jump Test
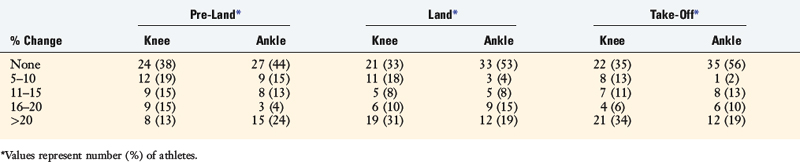
The neuromuscular-training program was effective, supporting the hypothesis, because statistically significant increases were found after training in the subgroup of 62 females in the absolute (see Table 16-1) and the normalized knee (see Fig. 16-8) and ankle (see Fig. 16-9) separation distances for all phases of the jump-land sequence (P < .001). After training, the female athletes had statistically greater mean normalized knee and ankle separation distances than the male athletes for all phases of the jump-land sequence (P < .0001). In addition, after training, a statistically significant difference was found in the distribution of female athletes who had less than 60%, 61% to 80%, or greater than 80% knee separation distance on landing (P = .003) and take-off (P = .006). The distribution in the percentage change in knee and ankle separation distances after training is shown for all three phases of the jump-land sequence in Table 16-2.
Implication of Findings
The authors developed and studied a videographic drop-jump screening test to record lower limb axial alignment in the coronal plane using a single standard videographic camera. The testing procedure was designed to be relatively easy to perform by researchers, coaches, trainers, or therapists in any facility. The goal was to provide a general indicator of an athlete’s lower limb axial alignment in the coronal plane in a straightforward drop-jump and vertical take-off task. The authors do not propose that this videographic analysis can be used as a risk indicator for a knee ligament injury. The test depicts only hip, knee, and ankle positions in a single plane during one maneuver, and it is recognized that noncontact ACL injuries may occur in side-to-side or cutting motions. A more sophisticated multicamera system would be required to measure these types of motions. The use of even just a second camera to measure the degrees of knee flexion on landing would provide additional information44; however, the goal was to use one camera to make the measurements easier to perform from a screening standpoint. Because of these limitations, it may be that the single-plane videographic drop-jump test was not sensitive enough to depict relevant differences in landing patterns between the sexes.
Authors have reported that 58% to 61% of noncontact injuries occur on landing from a jump.28,30 The final position of the knee joint on landing is influenced by the center of gravity of the upper body and the trunk over the lower extremity. Equally important are the positions of trunk-hip adduction or abduction, foot-ankle pronation-supination, and foot separation distance. These effects combine together to produce either a varus or a valgus moment about the knee joint that must be balanced by the lower limb musculature (see Fig. 16-1).42 If the athlete is off-balance, or has contact with another player, a loss of trunk and lower limb control and position may occur and the knee joint may go into a hyperextended or severe valgus position. The knee position measured in the coronal plane in the authors’ single-plane videographic analysis is a reflection of rotations in both the coronal and the transverse planes (internal-external femoral and tibial rotation). This test does not distinguish between these individual motions, which requires more sophisticated instrumentation.42
Although there are many potential mechanisms for ACL injury, it has been postulated that excessive valgus moments about the knee joint with subsequent high anterior tibial shear forces may be one of the ACL injury mechanisms in females.33,46,53 Excessive valgus loading may result in decreased tibiofemoral contact or condylar lift-off54 and a reduction in the normal joint contact geometry that contributes to knee joint stability. This position, coupled with a highly activated quadriceps muscle that produces maximum anterior shear forces with the knee joint at low flexion angles (≤30°),23,35,67 can lead to ACL rupture.
Hamstrings muscle activation with the knee joint at or near full knee extension (≤30°) produces insufficient posterior tibia shear forces to protect the ACL owing to the small angle of inclination of the hamstring tendons.73 Noyes and Sonstegard66 described a decreased mechanical advantage of the inner hamstrings when the knee is extended, because the hamstring flexion force at 0° is approximately half that at 90°. Similarly, the rotation force of the inner hamstrings declines with knee extension, because the rotation force at 0° is 41% that of the rotation force that occurs at 90°. A rotation “wind-up” effect exists, in which the IR forces increase significantly with ER owing to an increase in muscle mechanical advantage.
The authors hypothesized that the majority of untrained female athletes would demonstrate an abnormal lower limb position on landing from a drop-jump and on acceleration into a vertical jump. A normalized knee separation distance of less than 60% occurred in 63% of the untrained females on landing and in 80% on take-off. It was also hypothesized that the majority of young male athletes would demonstrate a neutrally aligned lower limb position on landing and acceleration into a vertical jump. This hypothesis was not supported, because 75% of the males had marked knee separation distances on landing and 72% on take-off, indicating a valgus-aligned lower limb position. The significance of this finding is unknown and may represent an aberration requiring further study (Fig. 16-10). It may be that this single-plane videographic test was not sensitive enough to depict relevant differences in landing patterns between the sexes. Other studies that used multicamera systems or force plates to investigate the drop-jump test found significant differences between females and males regarding knee flexion angles,44 knee extension moments,16,42 knee valgus moments,16 and ground reaction forces.42 A prior investigation determined that untrained female athletes had lower knee extension moments than males and postulated that this was explained by the male subjects’ high use of the hamstrings as a knee flexor at landing.44



The authors believed that a neuromuscular-training program would increase knee separation distance in female athletes, thereby leading to a more neutral overall lower limb position during the drop-jump test (Fig. 16-11). The goals of the training program were to teach athletes to control the upper body, trunk, and lower body position; lower the center of gravity by increasing hip and knee flexion on landing; and develop muscular strength and techniques to land with decreased ground reaction forces. In addition, athletes were taught to pre-position the body and lower extremity before landing in order to land in the position of greatest knee joint stability and stiffness, with the goal of obtaining ankle and knee separation distances within approximately 80% that of the hip separation distance. The neuromuscular-training program was previously shown to be effective in inducing changes in neuromuscular indices (see Chapter 19, Decreasing the Risk of ACL Injuries in Female Athletes),42 including decreasing peak landing forces and peak adduction and abduction moments and improving hamstrings-to-quadriceps ratios. A correlation was found between the ability of the athlete to control knee adduction and abduction moments and the peak landing forces (P = .006). Decreased abduction or abduction moments may lessen the risk of lift-off of the medial or lateral femoral condyle, improve tibiofemoral contact stabilizing forces,54 and decrease the risk of ligament injury. Other training techniques that use verbal and visual feedback have also been successful in reducing ground reaction forces.25,49,57,69,76





In the female athletes, significant increases were found after training in the absolute and normalized knee and ankle separation distances for all phases of the jump-land sequence (P < .001). As a result, the female athletes had significantly greater normalized knee and ankle separation distances than the males for each phase. The neuromuscular-training program was reported to be effective in another study in decreasing the incidence of noncontact serious knee ligament injuries in female athletes.40 In that report, 8 of 463 untrained females sustained a serious noncontact knee ligament injury compared with 0 of 366 trained females and 1 of 434 untrained male athletes. Untrained females had a 3.6 times higher incidence of knee injury than trained females (P = .05) and 4.8 times higher than males (P = .03).
It is unknown whether the improvement in knee separation distance after training will transfer to reduce the risk of a serious knee ligament injury in female athletes. The increased incidence of knee ligament injuries in female athletes is multifactorial and it is currently unknown which factors are dominant and which play a smaller role. A number of intrinsic factors inherent in women have been suggested, including a narrow intercondylar notch, smaller-sized ACL, pelvic-hip-knee-foot alignment, generalized knee laxity, foot pronation, and hormonal fluctuations.33 Extrinsic factors related to athletic conditioning, skill, training, and equipment have also been discussed. Although issues related to differences in neuromuscular control, muscle reaction patterns,45,93 and coordination and control of body and lower extremity positions during athletics are usually related to extrinsic factors, it may be that these factors are both intrinsic and extrinsic in their development.
It is important to note that some female athletes may require further training to demonstrate improvements in knee and ankle separation distance and land in a more neutrally aligned position. The pictorial sequence of the filmed drop-jump provides important information to athletes, parents, and coaches and can be useful in detecting athletes who require further neuromuscular training (see Fig. 16-11).
STUDY #2: NEUROMUSCULAR INDICES IN PREPUBESCENT ATHLETES
In this study, 27 girls and 25 boys who were participating in organized athletics were recruited from area schools and youth soccer leagues to participate.7 There was no difference between the girls and the boys for mean age (9.7 ± 0.5 yr and 9.6 ± 0.5 yr, respectively), height (136 ± 7 cm and 133 ± 5 cm, respectively), weight (39 ± 11 kg and 36 ± 5 kg, respectively), or BMI (18 ± 4 and 18 ± 2, respectively). There was no difference between the girls and the boys in the mean years of sports participation before testing (4.8 ± 1.4 yr and 4.6 ± 0.7 yr, respectively) or the mean age in which they had begun organized sports participation (4.8 ± 1.3 yr and 4.9 ± 0.9 yr, respectively).
Critical Points STUDY #2: NEUROMUSCULAR INDICES IN PREPUBESCENT ATHLETES
Implication of Findings
Hypothesis #1: No Significant Difference Exists between Prepubescent Boys and Prepubescent Girls in Overall Lower Limb Alignment during a Drop-Jump Test
The hypothesis was supported, because a marked decrease in normalized knee separation distance of less than 60% was found in 19 males (76%) and 25 females (93%) on landing (Fig. 16-12).

The male athletes had greater absolute ankle separation distances than the females (pre-land, 35 ± 5 cm and 28 ± 5 cm, respectively; landing, 32 ± 6 cm and 24 ± 6 cm, respectively; take-off, 32 ± 6 cm and 24 ± 5, respectively; P < .001), and greater normalized ankle separation distances as shown in Table 16-3. A wider 95% confidence interval (CI) range was noted for the male athletes than for the female values for all three phases of the test.

Male athletes also had greater absolute knee separation distances on pre-land and landing than females (pre-land, 22 ± 4 cm and 17 ± 4 cm, respectively; landing, 18 ± 7 cm and 14 ± 5 cm, respectively; P < .05), and greater normalized knee separation distances in these phases, as shown in Table 16-4. A wider 95% CI range was found for the male athletes on landing and take-off than for the females.
Hypothesis #2: No Significant Difference Exists between Prepubescent Boys and Prepubescent Girls in Knee Extensor and Flexor Strength
The hypothesis was supported, because there was no difference between genders in knee extensor and flexor peak torques (Table 16-5). No correlations were found between extensor and flexor peak torque values and overall lower limb alignment in the three phases of the drop-jump test. There was also no correlation between the isokinetic indices and BW or BMI for either gender.
Hypothesis #3: No Significant Difference Exists between Prepubescent Boys and Prepubescent Girls in Lower Limb Symmetry on Single-Leg Function Testing
Implication of Findings
The authors hypothesized that no difference exists between genders in overall lower limb alignment during a drop-jump test. A valgus lower limb alignment assumed during athletic maneuvers has been hypothesized to increase the risk for a serious knee ligament injury, based on studies involving adolescent and adult athletes.33,46 It was believed that prepubescent children would not demonstrate these gender differences because their muscle strength and motor skills had not yet fully developed.
The data indicated that 76% of boys and 93% of girls had a marked valgus alignment (<60% knee separation distance) during the videographic drop-jump test. This valgus lower limb alignment occurred even though the boys had greater ankle and knee separation distances throughout the drop-jump sequence. For example, the boys had a mean knee separation distance on landing of 49% ± 18% (95% CI, 42%–56%) compared with the girls who had a mean knee separation distance of 41% ± 12% (95% CI, 36%–46%). The mean normalized ankle separation distance of the males of 92% on landing has a theoretical advantage in providing a broader base (Fig. 16-13). However, the majority of boys still showed an overall lower extremity valgus alignment on landing and take-off, presumably owing to hip adduction and internal rotation. The predominance of this posture in the subjects would be expected to lead them to a higher injury risk. However, this risk may be offset in children by their smaller stature and body mass and the relatively slower velocities involved in their sporting activities.

Whether neuromuscular training would be effective in improving overall lower limb alignment to a more neutral position in children on a drop-jump test is unknown. Few controlled studies have been conducted to investigate injury-prevention strategies in children.14,52,59 There are no formal national education or certification requirements for coaches in the United States, and it is unknown how many coaches have had formal training in conditioning and training, growth and development, or injury prevention.59 The continued analysis of knee ligament injury mechanisms is strongly advised, because newer coaching techniques and strategies may become effective in addressing the ACL injury problem.
The finding of a lack of a difference in all of the isokinetic muscle strength values between the boys and the girls agrees with other studies in children of similar ages.21,22,86 Gender-related strength differences are not expected to become apparent until the mid-teens.21,22,38,43,79,83 One purpose of conducting isokinetic testing in the study was to assess whether a correlation existed between knee extensor and flexor strength and knee or ankle separation distances, of which none was found.
The authors hypothesized that there would be no difference between boys and girls in lower limb symmetry as determined by single-leg-hop tests. One previous study assessed the reliability of two sports-related functional tests that involved speed and agility during double-legged activities (slalom and hurdle tests) in 11 athletes (8 boys and 3 girls) who were all 11 years of age.2 The intraclass correlation coefficients (ICCs) demonstrated adequate reliability of these tests. The standing balance of children 10 years of age and younger has been shown to be poorer than that of adults owing to their developing vestibular system.17 Postural sway has been shown to be greater in children 9 to 10 years of age than in those 15 to 18 years of age.95 In our study, abnormal limb symmetry was found in 77% of the females and 84% of the males in the timed side-hop test and in 55% of the females and 56% of the males in the triple-hop test. The timed side-hop test induced medial and lateral forces, and the children had a difficult time maintaining balance on one leg while hopping in these directions.
There was no correlation between knee extensor and flexor strength and lower limb symmetry on the single-leg-hop tests. Prior studies have shown a relationship between extensor strength and single-leg-hop testing in older populations 16 to 48 years of age.6,63 The results of the functional tests could be due to motor development skills and neuromuscular indices such as balance, proprioception, and hip muscle strength not analyzed in this study. Cross-sectional investigations using single-leg-hop tests on children and adolescents up to 18 years of age are necessary to determine whether an age effect exists similar to those that exist for isokinetic muscle strength19 and standing balance.17
STUDY #3: NEUROMUSCULAR INDICES IN ATHLETES 9 TO 17 YEARS OF AGE
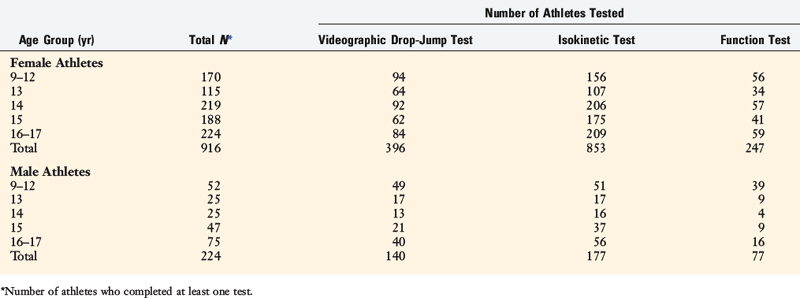
The number of athletes that participated in the tests for this investigation are shown in Table 16-6.8 In order to be able to compare data collected in this investigation with those previously reported,20–22,79,86 each subject was assigned to a category according to chronological age. This allowed establishment of age-related reference values, with age groups being as small as possible.9 The height and weight of the subjects fell within the 50th to 75th percentile according to Tanner-Whitehouse clinical growth charts.87,88
There was no statistically significant effect of lower limb dominance on any of the tests. The mean values provided for the isokinetic and videographic drop-jump tests are representative of the dominant limb. There was no difference in the results of the videographic drop-jump data when the knee and ankle separation distances were normalized to body height or BMI. Therefore, normalized data according to the hip separation distance are provided for consistency with other published data.7,65
Hypothesis #1: A Significant Increase in Isokinetic Knee Extensor and Flexor Strength Occurs with Age in Both Male and Female Athletes
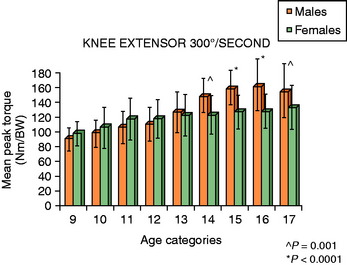
This hypothesis was supported for knee extensor strength in both female and male athletes. In the female athletes, a significant increase in the normalized mean extensor peak torque was noted from the ages of 9 to 13 (P < .001; Fig. 16-14). The average extensor peak torque in the 13-year-olds was 20% greater than that of the 9-year-old subjects. There were no significant increases in this factor after the age of 13. In the male athletes, significant increases in mean extensor peak torque were found from ages 9 to 14 (P < .001). The average extensor peak torque in the 14-year-olds was 38% greater than that of the 9-year-old subjects. There were no significant differences in this factor after the age of 14.
Critical Points STUDY #3: NEUROMUSCULAR INDICES IN ATHLETES 9–17 YEARS OF AGE
N = 1140 athletes tested; each subject was assigned to a category according to chronological age.
Hypothesis #4: Age and gender do not influence overall lower limb alignment on a drop-jump test.
Implications of Findings
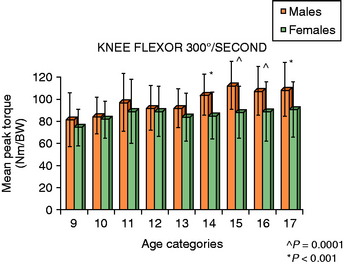
Whereas this hypothesis was supported for isokinetic knee flexion strength in male athletes, it was not supported in the female athletes. The normalized mean flexor peak torque was only slightly greater in female athletes 11 years of age than in those 9 to 10 years of age (Fig. 16-15). There was no significant difference in flexor peak torques in athletes older than the age of 11. Hamstrings-to-quadriceps ratios slightly declined with age (from 82% at age 10 to 70% at age 17). In the male athletes, normalized mean flexor peak torque significantly increased from 80 ± 26 Nm/BW at age 9 to 104 ± 16 Nm/BW at age 14 (P < .001). Hamstrings-to-quadriceps ratios declined significantly from ages 9 (mean, 87%) to 14 (mean, 72%; P < .001), after which this value remained constant. There was no correlation between age and extensor or flexor peak torque absolute values, peak torque normalized values, or the hamstrings-to-quadriceps ratio for either gender.
Hypothesis #2: Males Aged 14 and Older Have Significantly Greater Lower Limb Muscle Strength than Age-matched Females
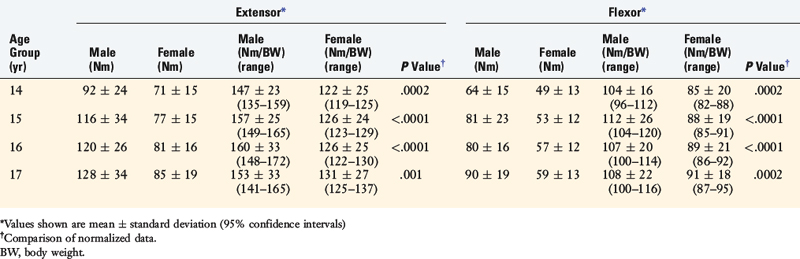
This hypothesis was supported, because from ages 14 to 17, male athletes had significantly greater mean extensor and flexor peak torques than age-matched female athletes (Table 16-7). There was no significant difference between genders in the hamstrings-to-quadriceps ratio in any age group.
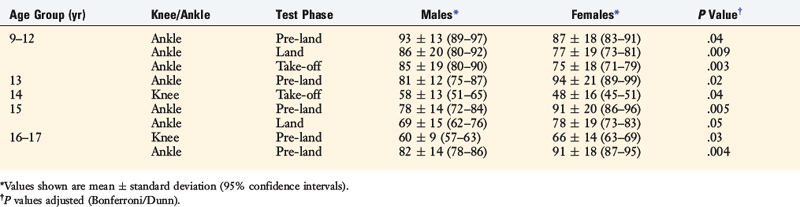
TABLE 16-7 Statistically Significant Differences between Male and Female Athletes in Knee Extensor and Flexor Strength
Critical Points STUDY #4: TIBIAL ROTATION STRENGTH IN MALE AND FEMALE ATHLETES 11–17 YEARS OF AGE
N = 94 athletes (47 female, 47 male), aged 11–17 yr.
Implications of Findings
Hypothesis #3: Age and Gender Do not Influence Lower Limb Symmetry on Single-Leg-Hop Functional Testing
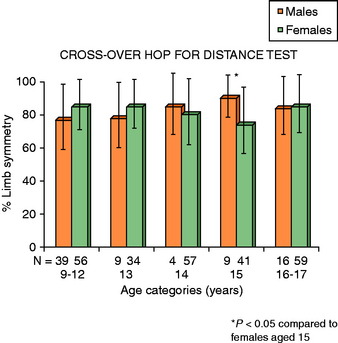
The hypothesis was supported, because no statistically significant difference was found in the mean lower limb symmetry values between any of the age groups for either the female or the male athletes in the single-leg-hop tests (Figs. 16-16 and 16-17). There was no correlation between extensor and flexor peak torques and limb symmetry.
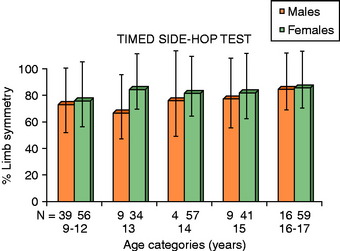
FIGURE 16-16 There was no effect of age or gender on limb symmetry in the timed side-hop test.
(From Barber-Westin, S. D.; Noyes, F. R.; Galloway, M.: Jump-land characteristics and muscle strength development in young athletes: a gender comparison of 1140 athletes 9 to 17 years of age. Am J Sports Med 34:375–384, 2006.)
Hypothesis #4: Age and Gender Do not Influence Overall Lower Limb Alignment on a Drop-Jump Test
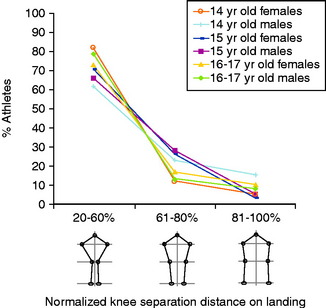
The hypothesis was supported, because there was no effect of age found in either the female or the male athletes on the mean normalized ankle and knee separation distances on landing (Fig. 16-18) or take-off. There was no significant difference in the percentage of athletes within the categories of less than 60%, 61% to 80%, or greater than 80% normalized knee separation distance (Fig. 16-19). A distinct overall lower limb valgus alignment (<60% knee separation distance) was measured in 78% of female athletes aged 9 to 12, 81% of athletes aged 13, 83% of athletes aged 14, 71% of athletes aged 15, and 74% of athletes aged 16 to 17. In the male athletes, a distinct valgus alignment was found in 79% of those aged 9 to 12, 70% of athletes aged 13, 62% of athletes aged 14, 67% of athletes aged 15, and 80% of athletes aged 16 to 17.
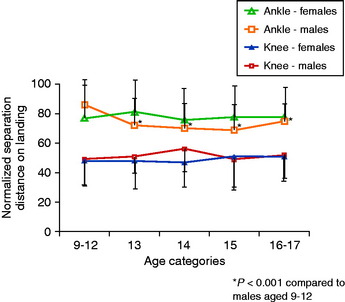
Significant differences were found in the male athletes between the age groups in mean ankle separation distances for all three phases of the drop-jump test (P < .005). The ankle separation distances were greatest in the 9- to 12-year-olds and smallest in the 15-year-olds. Significant differences were found between genders in the mean ankle separation distances in the pre-land phase (Table 16-8). Although male athletes had greater mean ankle separation distances in the 9- to 12-year-old group, female athletes had greater mean values in the 13-, 15-, and 16- to 17-year old groups. Few significant differences were found between genders within the age categories in the mean normalized knee separation distances.
Study Implications
The first hypothesis was that a significant increase in lower limb muscle strength occurs with age in both male and female athletes. There is disparity in the literature regarding age effects on knee extensor and flexor strength within gender owing to the few comprehensive cross-sectional or longitudinal studies that have been published. No age effects were found in females or males when tested at a low-velocity speed (30°/sec) after stature and mass were accounted for in two investigations.21,22 Other authors reported that an age effect existed in both genders for extensor and flexor torques at velocity speeds ranging from 12°/sec to 150°/sec.86 Another report claimed that an age effect existed for males, but not for females, in knee extensor and flexor peak torques at 300°/sec.41 De Ste Croix and colleagues22 tested 46 subjects aged 8 to 9 years, 47 subjects aged 13 to 14 years, and 48 subjects aged 18 to 27 years. Knee extensor and flexor strength increased with age, regardless of how the data were analyzed (absolute, body mass–related, or body mass–adjusted). Ramos and coworkers79 tested 18 subjects aged 11 to 12 years, 21 subjects aged 13 to 14 years, and 18 subjects aged 17 to 18 years, and reported increases in absolute and BW-corrected peak torque with age in both males and females.
The second hypothesis was that males aged 14 and older have significantly greater lower limb muscle strength than age-matched females. Three investigations on isokinetic testing in children reported no differences between boys and girls in knee extensor or flexor strength up to the age of 14, even after controlling for body mass and stature.21,22,79 Our data was in agreement, because there was no difference between genders in lower extremity muscle strength until the age of 14. One of the most important findings from this investigation was the difference between the male and the female athletes in strength increases in knee flexor peak torque according to the age categories. Whereas flexor peak torques in males gradually increased from ages 9 to 14, such increases were noted in females only from ages 9 to 11. In addition, the increases noted in extensor and flexor peak torques with age in males was approximately double those of females, even after controlling for BW. One theory of the increased incidence of ACL injury in female athletes compared with males relates to the quadriceps-dominance effect, or greater quadriceps activation measured during functional activities.16,53 An increased quadriceps muscle force combined with a decreased hamstring muscle force and decreased knee flexion angle produce an increased proximal tibial anterior shear force that may result in excessive strain on the ACL.16,45,53,80 It would appear from this study that an emphasis on hamstring-strengthening programs needs to be further pursued in young female athletes to enable them to continue to achieve strength gains past the age of 11.
The third hypothesis was that age and gender do not influence lower limb symmetry on single-leg-hop functional testing. There was no difference in limb symmetry between the age categories in either the male or the female athletes. Although the mean values of the two hop tests indicated adequate limb symmetry was present within most age categories, the large standard deviations prevent definitive conclusions. In a previous study from the authors’ institution that involved 93 subjects aged 17 to 34 years, 90% had limb symmetry of at least 85%. A relationship between extensor strength and single-leg-hop testing was reported in one study6; however, a second investigation failed to find a significant correlation.63 No association was found in the current investigation between extensor or flexor strength and limb symmetry values. Studies conducted elsewhere have presented wide variability in regard to a correlation between extensor strength and limb symmetry on single-leg-hop testing; moderate correlation coefficients (R = 0.60–0.78) were reported by Greenberger and Paterno,31 Sachs and associates,81 Wilk and colleagues,90 and Barber and coworkers.6 However, low correlation coefficients were described by other investigators,71,74,75,84 and no definitive conclusion may be reached regarding this association.
The fourth hypothesis was that age and gender do not influence overall lower limb alignment on a drop-jump test. Some authors have postulated that female athletes tend to land from a jump in a noteworthy valgus lower limb alignment, in contrast to male athletes who land in a more neutrally aligned position, and that a valgus alignment position increases the risk for a knee ligament injury.33,46 However, based on data from prior investigations, we believed no difference in lower limb alignment on a drop-jump task would be detected between genders.7,65 The results showed that, although males aged 9 to 12 had greater mean ankle separation distances than age-matched females, and males aged 14 had greater knee separation distances on take-off than females, the majority of all athletes had a distinct valgus lower limb alignment on landing. Valgus knee alignment on take-off and landing has been hypothesized to predispose an athlete to ACL rupture and indeed is commonly seen during noncontact ACL injuries.11,28,30
Hass and associates37 recently reported an age-dependent effect on knee biomechanics during landing between 16 prepubescent (aged 8–11 yr) and 16 postpubescent (aged 18–25 yr) females. The postpubescent group had reduced knee flexion upon initial contact (4.5°) and increased medial knee forces, but decreased landing forces and knee extensor moments than the younger group. Although the study’s results suggested the presence of a developmental effect on landing mechanisms, the authors concluded that further work is required on the effects of age, developmental level, and motor control during landing.
Chappell and colleagues16 reported no difference between genders aged 19 to 25 years in the magnitude of knee varus-valgus moments during three stop-jump tasks. Those authors concluded that the female knee varus-valgus moment may not be responsible for the gender differences in ACL strain during those tasks. The increased incidence of knee injuries in female athletes is most likely due to many factors. Whereas a valgus alignment position assumed on landing may increase the risk for a knee ligament injury, the fact that there was no difference detected in alignment between genders in the authors’ study in such a large number of athletes indicates that other factors most likely have a role in the increased ACL injury rate in females. In addition, injury mechanisms other than a valgus knee position have been noted during ACL ruptures,11 including a sudden deceleration, acceleration, or change of direction in response to avoiding contact with another player or in reaction to a ball or play. Differences between genders in muscle reaction and firing patterns,45,93 coordination, control of body and lower extremity positions during athletics, lower extremity and hip strength, and external-internal knee flexion moments all most likely contribute to this problem. Neuromuscular training (see Chapter 19, Decreasing the Risk of ACL Injuries in Female Athletes) is effective in improving lower limb alignment on the drop-jump test,65 increasing hamstrings strength, increasing knee flexion angles on landing,42,44,76 and reducing deleterious moments and ground reaction forces.
STUDY #4: TIBIAL ROTATION STRENGTH IN MALE AND FEMALE ATHLETES 11 TO 17 YEARS OF AGE
The study population comprised 94 athletes (47 females and 47 males), aged 11 to 17 years, who participated in a variety of organized sports including soccer, basketball, volleyball, baseball, football, and track and field.64 In order to evaluate the primary study outcomes (mean peak torque and time-to-peak torque), sample-size calculations and the power to detect a difference of 10% between gender and age group mean scores were determined by an independent statistician. With 94 patients in this study, it was found that the investigation had sufficient power (>80%) to detect differences in mean peak IR and ER torque and time-to-peak torque of at least 10% between genders and age group categories.
Hypothesis #1: A Significant Increase in IR and ER Strength Occurs with Age in Both Male and Female Athletes
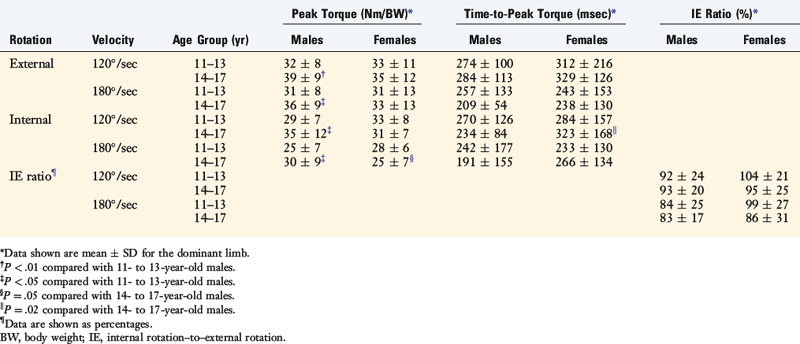
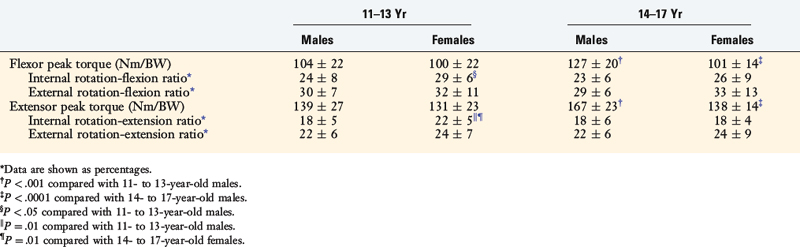
The hypothesis was proved true for the male athletes, but not for the female athletes. Male athletes aged 14 to 17 years had significantly greater mean IR and ER peak torques (Table 16-9), and significantly greater extensor and flexor peak torques (Table 16-10), than males aged 11 to 13 years. There was no significant difference in all of the lower limb muscle strength indices in female athletes between the ages of 11 to 13 years and 14 to 17 years.
Hypothesis #2: No Difference Exists between Male and Female Athletes Aged 11 to 13 in IR and ER Strength
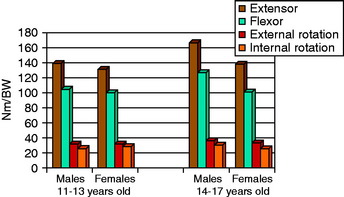
The hypothesis was supported, because there was no significant difference between male and female athletes 11 to 13 years of age regarding IR and ER strength (Fig. 16-20). Females aged 11 to 13 years had significantly greater mean IR-F and IR-E ratios than age-matched males.
Hypothesis #3: Male Athletes Aged 14 to 17 Have Significantly Greater IR and ER Strength than Age-matched Female Athletes
The hypothesis was supported for IR only, because males aged 14 to 17 years had a significantly greater mean IR peak torque (at 180°/sec) and a significantly faster mean time-to-reach IR peak torque than age-matched females (see Table 16-9). There was no significant difference between the male and the female athletes for mean ER peak torque.
Study Implications
This is the first study to conduct lower extremity tibial rotational strength testing in athletes 11 to 17 years of age with the specific purposes of assessing age- and gender-related effects. During a potential injury situation, dynamic muscular stabilization of the knee joint, particularly the hamstring muscles, may potentially reduce ACL strain.24,45,61,77,80 Several investigators have demonstrated that female athletes have weaker knee flexor peak torques, and take longer to develop flexor peak torque, than males even after normalizing for BW.18,32,42,45 The impetus for this study was the paucity of published data regarding the IR and ER isokinetic strength of the hamstring musculature.
The isokinetic test design and protocol was performed in a manner similar to that of other investigations.39,82,89 The joint angular positions were based on biomechanical studies that demonstrated that the rotational force of the pes anserinus musculature (sartorius, gracilis, semitendinosus) is greatest at 90° of knee flexion.66,85 A significant decrease in rotational force exists as the knee is extended, declining as much as 41% when the knee is fully extended (0°) compared with the strength measured at 90° of flexion. Hip flexion angle also affects the generation of internal rotational torque, with greater torque generated at higher hip flexion angles (when the knee is flexed 90°).70,85 The test protocol was similar to that described by other investigators with respect to hip and knee flexion angles, stabilization of the foot, and the resting position used to determine the neutral position before the onset of testing.39,82,89
A limitation of this study is the fact that it is not possible to isolate and measure the specific muscles that act as the primary internal rotators (semitendinosus, gracilis, popliteus, semimembranosus, and sartorius) and external rotators (biceps muscle, long and short head)13 with dynamometer systems. However, the testing procedure does provide a functional assessment of lower limb isokinetic capabilities. The data showed few effects of lower limb dominance on rotational strength, which agreed with the results of Osternig and coworkers72 and Hester and Falkel.39 The results of the IE ratios were also similar with those reported previously, because the mean ER peak torque slightly exceeded that of IR peak torque at both velocities.39,72
The first hypothesis, that a significant increase in IR and ER strength occurs with age in both genders, was proved for males but not for females. Male athletes aged 14 to 17 years had significantly greater mean IR (17% for both test velocities) and ER (14%–18%) peak torques than males aged 11 to 13 years. In contrast, females aged 14 to 17 years had only 6% greater ER strength than that measured in 11- to 13-year-old females. Further rotational strength testing is required in cross-sectional or longitudinal studies before a conclusion can be reached on the effects of aging on IR and ER peak torques. Our study did demonstrate a hierarchy of isokinetic peak torques in the musculature about the knee, which was similar in both genders and age groups (see Fig. 16-20).
Our second hypothesis, that no difference exists between genders aged 11 to 13 years in IR and ER strength, was supported. Other investigators have successfully used a variety of isokinetic velocity speeds to measure knee extension and flexion peak torque in children, ranging from 12°/sec86 to 300°/sec.26 No significant gender-related knee flexion and extension strength differences have been reported by authors in children between the ages of 8 and 14 years.21,22,86 Our investigation showed no difference between genders aged 11 to 13 years in mean ER and IR peak torque values, time-to-peak torque, or IE ratios.
Our third hypothesis, that male athletes aged 14 to 17 years have significantly greater tibial rotation isokinetic muscle strength than age-matched female athletes, was supported. The IR peak torques for the males were 17% greater than those of the females at 180°/sec. Viola and associates89 reported that the noninjured limb IR of males was approximately 25% stronger than the uninjured limb IR of females at 120°/sec; and approximately 11% stronger at 180°/sec. These data were not normalized for BW. Segawa and associates82 reported that (after normalization for BW) the male noninjured limb IR was approximately 16% stronger than the female uninjured limb IR at 120°/sec. There appears to be no difference in ER strength between genders, according to the data from our study and those of other investigators.89,93
Our study is the first we are aware of to report that male athletes have faster times-to-reach peak torque for IR than age-matched female athletes. Gender differences in muscular protection of the knee joint during weight-bearing and non–weight-bearing activities have been reported by many authors, but only a few have included IR data. Wojtys and colleagues93 compared the amount of IR and rotational stiffness in collegiate athletes participating in high-risk sports with those participating in low-risk endurance sports. Gender comparisons were performed regarding the amount of passive and active IR in response to a medially directed 80-N force (with the subjects seated) and the resultant amount of apparent knee joint stiffness. Male athletes participating in high-risk sports had significantly less IR (mean, 3°) during muscle activation, and significantly greater (42%) apparent joint stiffness than the female athletes. However, Lephart and coworkers50 found that collegiate women who participated in high-risk sports had less knee flexion and IR maximum angular displacements during single-leg landing and forward hop landing tasks than age- and activity-matched males. McLean and associates55 reported that women had an average of 5° less IR during a sidestep maneuver, along with less hip flexion, hip abduction, hip internal rotation, and knee flexion than age-matched males. The protection provided by the dynamic neuromuscular control of the lower extremity is multifactorial and beyond the scope of the authors’ study.
CONCLUSIONS
The important findings from the four studies are
1 Adirim T.A., Cheng T.L. Overview of injuries in the young athlete. Sports Med. 2003;33:75-81.
2 Alricsson M., Harms-Ringdahl K., Werner S. Reliability of sports-related functional tests with emphasis on speed and agility in young athletes. Scand J Med Sci Sports. 2001;11:229-232.
3 Anderson M., Messner M.B., Green W.T. Distribution of lengths of the normal femur and tibia in children from one to eighteen years of age. J Bone Joint Surg Am. 1964;46:1197-1202.
4 Arendt E., Dick R. Knee injury patterns among men and women in collegiate basketball and soccer. NCAA data and review of literature. Am J Sports Med. 1995;23:694-701.
5 Bandy W., Rusche K., Tekulve F.X. Reliability and limb symmetry for five unilateral functional tests of the lower extremities. Isok Exer Sci. 1994;4:108-111.
6 Barber S.D., Noyes F.R., Mangine R.E. Quantitative assessment of functional limitations in normal and anterior cruciate ligament–deficient knees. Clin Orthop. 1990;255:204-214.
7 Barber-Westin S.D., Galloway M., Noyes F.R., et al. Assessment of lower limb neuromuscular control in prepubescent athletes. Am J Sports Med. 2005;33:1853-1860.
8 Barber-Westin S.D., Noyes F.R., Galloway M. Jump-land characteristics and muscle strength development in young athletes: a gender comparison of 1140 athletes 9 to 17 years of age. Am J Sports Med. 2006;34:375-384.
9 Beenakker E.A., van der Hoeven J.H., Fock J.M., Maurits N.M. Reference values of maximum isometric muscle force obtained in 270 children aged 4–16 years by hand-held dynamometry. Neuromuscul Disord. 2001;11:441-446.
10 Berns G.S., Hull M.L., Patterson H.A. Strain in the anteromedial bundle of the anterior cruciate ligament under combination loading. J Orthop Res. 1992;10:167-176.
11 Boden B.P., Dean G.S., Feagin J.A.Jr, Garrett W.E.Jr. Mechanisms of anterior cruciate ligament injury. Orthopedics. 2000;23:573-578.
12 Bolgla L.A., Keskula D.R. Reliability of lower extremity functional performance tests. J Orthop Sports Phys Ther. 1997;26:138-142.
13 Buford W.L.Jr, Ivey F.M.Jr, Nakamura T., et al. Internal/external rotation moment arms of muscles at the knee: moment arms for the normal knee and the ACL-deficient knee. Knee. 2001;8:293-303.
14 Chalmers D.J. Injury prevention in sport: not yet part of the game? Inj Prev. 2002;8(suppl 4):IV22-IV25.
15 Chandy T.A., Grana W.A. Secondary school athletic injury in boys and girls: A three-year comparison. Physician Sportsmed. 1985;13:106-111.
16 Chappell J.D., Yu B., Kirkendall D.T., Garrett W.E. A comparison of knee kinetics between male and female recreational athletes in stop-jump tasks. Am J Sports Med. 2002;30:261-267.
17 Cherng R.J., Chen J.J., Su F.C. Vestibular system in performance of standing balance of children and young adults under altered sensory conditions. Percept Mot Skills. 2001;92(3 pt 2):1167-1179.
18 Cowling E.J., Steele J.R. Is lower limb muscle synchrony during landing affected by gender? Implications for variations in ACL injury rates. J Electromyogr Kinesiol. 2001;11:263-268.
19 De Ste Croix M., Deighan M., Armstrong N. Assessment and interpretation of isokinetic muscle strength during growth and maturation. Sports Med. 2003;33:727-743.
20 De Ste Croix M.B., Armstrong N., Chia M.Y., et al. Changes in short-term power output in 10- to 12-year-olds. J Sports Sci. 2001;19:141-148.
21 De Ste Croix M.B., Armstrong N., Welsman J.R., Sharpe P. Longitudinal changes in isokinetic leg strength in 10- to 14-year-olds. Ann Hum Biol. 2002;29:50-62.
22 De Ste Croix M. B.A., Armstrong N., Welsman J.R. Concentric isokinetic leg strength in pre-teen, teenage and adult males and females. Biol Sport. 1999;16:75-86.
23 DeMorat G., Weinhold P., Blackburn T., et al. Aggressive quadriceps loading can induce noncontact anterior cruciate ligament injury. Am J Sports Med. 2004;32:477-483.
24 Draganich L.F., Vahey J.W. An in vitro study of anterior cruciate ligament strain induced by quadriceps and hamstrings forces. J Orthop Res. 1990;8:57-63.
25 Dufek J.S., Bates B.T. The evaluation and prediction of impact forces during landings. Med Sci Sports Exerc. 1990;22:370-377.
26 Ellenbecker T.S., Roetert E.P. Concentric isokinetic quadriceps and hamstrings strength in elite junior tennis players. Isok Exer Sci. 1995;5:3-6.
27 Ferber R., Davis I.M., Williams D.S.3rd. Gender differences in lower extremity mechanics during running. Clin Biomech (Bristol, Avon). 2003;18:350-357.
28 Gerberich S.G., Luhmann S., Finke C., et al. Analysis of severe injuries associated with volleyball activities. Physician Sportsmed. 1987;15:75-79.
29 Goh S., Boyle J. Self-evaluation and functional testing two to four years post ACL reconstruction. Aust J Physiother. 1997;43:255-262.
30 Gray J., Taunton J.E., McKenzie D.C., et al. A survey of injuries to the anterior cruciate ligament of the knee in female basketball players. Int J Sports Med. 1985;6:314-316.
31 Greenberger H.B., Paterno M.V. Relationship of knee extensor strength and hopping test performance in the assessment of lower extremity function. J Orthop Sports Phys Ther. 1995;22:202-206.
32 Griffin J.W., Tooms R.E., vander Zwaag R., et al. Eccentric muscle performance of elbow and knee muscle groups in untrained men and women. Med Sci Sports Exerc. 1993;25:936-944.
33 Griffin L.Y., et al. Noncontact anterior cruciate ligament injuries: risk factors and prevention strategies. J Am Acad Orthop Surg. 2000;8:141-150.
34 Griffin L.Y., et al. Understanding and preventing noncontact anterior cruciate ligament injuries: a review of the Hunt Valley II Meeting, January 2005. Am J Sports Med. 2006;34:1512-1532.
35 Grood E.S., Suntay W.J., Noyes F.R., Butler D.L. Biomechanics of the knee-extension exercise. Effect of cutting the anterior cruciate ligament. J Bone Joint Surg Am. 1984;66:725-734.
36 Gwinn D.E., Wilckens J.H., McDevitt E.R., et al. The relative incidence of anterior cruciate ligament injury in men and women at the United States Naval Academy. Am J Sports Med. 2000;28:98-102.
37 Hass C.J., Schick E.A., Tillman M.D., et al. Knee biomechanics during landings: comparison of pre- and postpubescent females. Med Sci Sports Exerc. 2005;37:100-107.
38 Henderson R.C., Howes C.L., Erickson K.L., et al. Knee flexor-extensor strength in children. J Orthop Sports Phys Ther. 1993;18:559-563.
39 Hester J.T., Falkel J. Isokinetic evaluation of tibial rotation: assessment of a stabilization technique. J Orthop Sports Phys Ther. 1984;6:46-51.
40 Hewett T.E., Lindenfeld T.N., Riccobene J.V., Noyes F.R. The effect of neuromuscular training on the incidence of knee injury in female athletes. A prospective study. Am J Sports Med. 1999;27:699-706.
41 Hewett T.E., Myer G.D., Ford K.R. Decrease in neuromuscular control about the knee with maturation in female athletes. J Bone Joint Surg Am. 2004;86:1601-1608.
42 Hewett T.E., Stroupe A.L., Nance T.A., Noyes F.R. Plyometric training in female athletes. Decreased impact forces and increased hamstring torques. Am J Sports Med. 1996;24:765-773.
43 Holm I., Steen H., Olstad M. Isokinetic muscle performance in growing boys from pre-teen to maturity. An eleven-year longitudinal study. Isok Exer Sci. 2005;13:153-158.
44 Huston L.J., Vibert B., Ashton-Miller J.A., Wojtys E.M. Gender differences in knee angle when landing from a drop-jump. Am J Knee Surg. 2001;14:215-219.
45 Huston L.J., Wojtys E.M. Neuromuscular performance characteristics in elite female athletes. Am J Sports Med. 1996;24:427-436.
46 Hutchinson M.R., Ireland M.L. Knee injuries in female athletes. Sports Med. 1995;19:288-302.
47 Jones S.J., Lyons R.A., Sibert J., et al. Changes in sports injuries to children between 1983 and 1998: comparison of case series. J Public Health Med. 2001;23:268-271.
48 Kellis E., Kellis S., Gerodimos V. Reliability of isokinetic concentric and eccentric strength in circumpubertal soccer players. Pediatr Exerc Sci. 1999;11:218-228.
49 Lees A. Methods of impact absorption when landing from a jump. Eng Med. 1981;10:207-211.
50 Lephart S.M., Ferris C.M., Riemann B.L., et al. Gender differences in strength and lower extremity kinematics during landing. Clin Orthop. 2002;401:162-169.
51 Lindenfeld T.N., Schmitt D.J., Hendy M.P., et al. Incidence of injury in indoor soccer. Am J Sports Med. 1994;22:364-371.
52 MacKay M., Scanlan A., Olsen L., et al. Looking for the evidence: a systematic review of prevention strategies addressing sport and recreational injury among children and youth. J Sci Med Sport. 2004;7:58-73.
53 Malinzak R.A., Colby S.M., Kirkendall D.T., et al. A comparison of knee joint motion patterns between men and women in selected athletic tasks. Clin Biomech (Bristol, Avon). 2001;16:438-445.
54 Markolf K.L., Burchfield D.M., Shapiro M.M., et al. Combined knee loading states that generate high anterior cruciate ligament forces. J Orthop Res. 1995;13:930-935.
55 McLean S.G., Lipfert S.W., van den Bogert A.J. Effect of gender and defensive opponent on the biomechanics of sidestep cutting. Med Sci Sports Exerc. 2004;36:1008-1016.
56 McLean S.G., Neal R.J., Myers P.T., Walters M.R. Knee joint kinematics during the sidestep cutting maneuver: potential for injury in women. Med Sci Sports Exerc. 1999;31:959-968.
57 McNair P.J., Prapavessis H., Callender K. Decreasing landing forces: effect of instruction. Br J Sports Med. 2000;34:293-296.
58 Merlini L., Dell’Accio D., Granata C. Reliability of dynamic strength knee muscle testing in children. J Orthop Sports Phys Ther. 1995;22:73-76.
59 Micheli L.J., Glassman R., Klein M. The prevention of sports injuries in children. Clin Sports Med. 2000;19:821-834.
60 Molnar G.E., Alexander J., Gutfeld N. Reliability of quantitative strength measurements in children. Arch Phys Med Rehabil. 1979;60:218-221.
61 More R.C., Karras B.T., Neiman F., et al. Hamstrings—an anterior cruciate ligament protagonist: an in vitro study. Am J Sports Med. 1993;21:231-237.
62 Moti A.W., Micheli L.J. Meniscal and articular cartilage injury in the skeletally immature knee. Instr Course Lect. 2003;52:683-690.
63 Noyes F.R., Barber S.D., Mangine R.E. Abnormal lower limb symmetry determined by function hop tests after anterior cruciate ligament rupture. Am J Sports Med. 1991;19:513-518.
64 Noyes F.R., Barber-Westin S.D. Isokinetic profile and differences in tibial rotation strength between male and female athletes 11 to 17 years of age. Isok Exer Sci. 2005;13:251-259.
65 Noyes F.R., Barber-Westin S.D., Fleckenstein C., et al. The drop-jump screening test: difference in lower limb control by gender and effect of neuromuscular training in female athletes. Am J Sports Med. 2005;33:197-207.
66 Noyes F.R., Sonstegard D.A. Biomechanical function of the pes anserinus at the knee and the effect of its transplantation. J Bone Joint Surg Am. 1973;55:1225-1241.
67 O’Connor J.J. Can muscle co-contraction protect knee ligaments after injury or repair? J Bone Joint Surg Br. 1993;75:41-48.
68 Olsen O.E., Myklebust G., Engebretsen L., et al. Relationship between floor type and risk of ACL injury in team handball. Scand J Med Sci Sports. 2003;13:299-304.
69 Onate J.A., Guskiewicz K.M., Sullivan R.J. Augmented feedback reduces jump landing forces. J Orthop Sports Phys Ther. 2001;31:511-517.
70 Oshimo T.A., Greene T.A., Jensen G.M., Lopopolo R.B. The effect of varied hip angles on the generation of internal tibial rotary torque. Med Sci Sports Exerc. 1983;15:529-534.
71 Ostenberg A., Roos E., Ekdahl C., Roos H. Isokinetic knee extensor strength and functional performance in healthy female soccer players. Scand J Med Sci Sports. 1998;8(5 pt 1):257-264.
72 Osternig L.R., Bates B.T., James S.L. Patterns of tibial rotary torque in knees of healthy subjects. Med Sci Sports Exerc. 1980;12:195-199.
73 Pandy M.G., Shelburne K.B. Dependence of cruciate-ligament loading on muscle forces and external load. J Biomech. 1997;30:1015-1024.
74 Petschnig R., Baron R., Albrecht M. The relationship between isokinetic quadriceps strength test and hop tests for distance and one-legged vertical jump test following anterior cruciate ligament reconstruction. J Orthop Sports Phys Ther. 1998;28:23-31.
75 Pincivero D.M., Lephart S.M., Karunakara R.G. Relation between open and closed kinematic chain assessment of knee strength and functional performance. Clin J Sport Med. 1997;7(1):11-16.
76 Prapavessis H., McNair P.J. Effects of instruction in jumping technique and experience jumping on ground reaction forces. J Orthop Sports Phys Ther. 1999;29:352-356.
77 Prietto C.A., Caiozzo V.J. The in vivo force-velocity relationship of the knee flexors and extensors. Am J Sports Med. 1989;17:607-611.
78 Radelet M.A., Lephart S.M., Rubinstein E.N., Myers J.B. Survey of the injury rate for children in community sports. Pediatrics. 2002;110:e28.
79 Ramos E., Frontera W.R., Llopart A., Feliciano D. Muscle strength and hormonal levels in adolescents: gender-related differences. Int J Sports Med. 1998;19:526-531.
80 Renstrom P., Arms S.W., Stanwyck T.S., et al. Strain within the anterior cruciate ligament during hamstring and quadriceps activity. Am J Sports Med. 1986;14:83-87.
81 Sachs R.A., Daniel D.M., Stone M.L., Garfein R.F. Patellofemoral problems after anterior cruciate ligament reconstruction. Am J Sports Med. 1989;17:760-765.
82 Segawa H., Omori G., Koga Y., et al. Rotational muscle strength of the limb after anterior cruciate ligament reconstruction using semitendinosus and gracilis tendon. Arthroscopy. 2002;18:177-182.
83 Seger J.Y., Thorstensson A. Muscle strength and electromyogram in boys and girls followed through puberty. Eur J Appl Physiol. 2000;81:54-61.
84 Sekiya I., Muneta T., Ogiuchi T., et al. Significance of the single-legged hop test to the anterior cruciate ligament–reconstructed knee in relation to muscle strength and anterior laxity. Am J Sports Med. 1998;26:384-388.
85 Shoemaker S.C., Markolf K.L. In vivo rotatory knee stability. Ligamentous and muscular contributions. J Bone Joint Surg Am. 1982;64:208-216.
86 Sunnegardh J., Bratteby L.E., Nordesjo L.O., Nordgren B. Isometric and isokinetic muscle strength, anthropometry and physical activity in 8- and 13-year-old Swedish children. Eur J Appl Physiol Occup Physiol. 1988;58:291-297.
87 Tanner J.M., Buckler J.M. Revision and update of Tanner-Whitehouse clinical longitudinal charts for height and weight. Eur J Pediatr. 1997;156:248-249.
88 Tanner J.M., Davies P.S. Clinical longitudinal standards for height and height velocity for North American children. J Pediatr. 1985;107:317-329.
89 Viola R.W., Sterett W.I., Newfield D., et al. Internal and external tibial rotation strength after anterior cruciate ligament reconstruction using ipsilateral semitendinosus and gracilis tendon autografts. Am J Sports Med. 2000;28:552-555.
90 Wilk K.E., Romaniello W.T., Soscia S.M., et al. The relationship between subjective knee scores, isokinetic testing, and functional testing in the ACL-reconstructed knee. J Orthop Sports Phys Ther. 1994;20:60-73.
91 Wojtys E.M., Ashton-Miller J.A., Huston L.J. A gender-related difference in the contribution of the knee musculature to sagittal-plane shear stiffness in subjects with similar knee laxity. J Bone Joint Surg Am. 2002;84:10-16.
92 Wojtys E.M., Huston L.J. Neuromuscular performance in normal and anterior cruciate ligament–deficient lower extremities. Am J Sports Med. 1994;22:89-104.
93 Wojtys E.M., Huston L.J., Schock H.J., et al. Gender differences in muscular protection of the knee in torsion in size-matched athletes. J Bone Joint Surg Am. 2003;85:782-789.
94 Wojtys E.M., Huston L.J., Taylor P.D., Bastian S.D. Neuromuscular adaptations in isokinetic, isotonic, and agility training programs. Am J Sports Med. 1996;24:187-192.
95 Wolff D.R., Rose J., Jones V.K., et al. Postural balance measurements for children and adolescents. J Orthop Res. 1998;16:271-275.






