Section 4 Lower Limb Injections
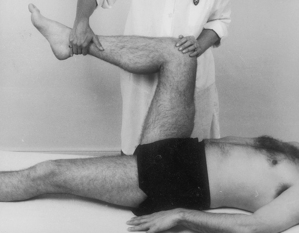
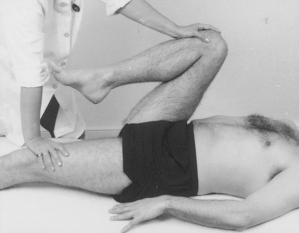
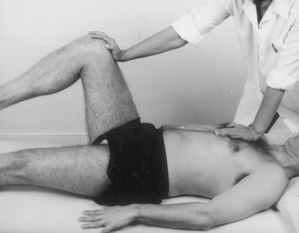
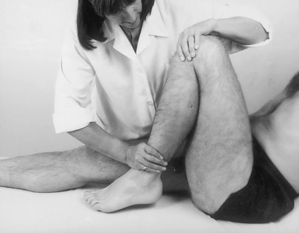
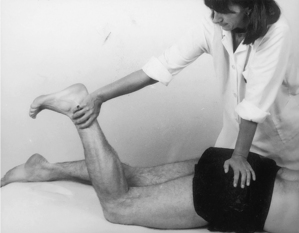
Examination of the lower limb
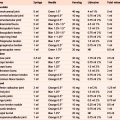
| Hip tests | ||
|---|---|---|
| In supine | In prone | |
| Passive lateral rotation | Passive extension | |
| medial rotation | Resisted lateral rotation | |
| flexion | medial rotation | |
| abduction | knee extension | |
| adduction | ||
| Resisted flexion | ||
| abduction | ||
| adduction | ||
| Hip capsular pattern: most loss of medial rotation, less of flexion and abduction, least of extension | ||
| Knee tests | ||
| Passive flexion | Draw test | |
| extension | Glide test | |
| valgus | Meniscal tests | |
| varus | Resisted extension | |
| rotation | flexion | |
| medial rotation | ||
| Knee capsular pattern: more loss of flexion than extension | ||
|---|---|---|
| Ankle and foot tests | ||
| Ankle | Subtalar | Forefoot |
| Passive dorsiflexion | Passive abduction | Passive abduction |
| plantarflexion | adduction | adduction |
| eversion | extension | |
| inversion | flexion | |
| Resisted dorsiflexion | ||
| plantarflexion | ||
| eversion | ||
| inversion | ||
| Ankle/foot capsular patterns: | ||
| Ankle: More loss of plantarflexion than dorsiflexion | ||
| Subtalar joint: More loss of adduction | ||
| Forefoot: Loss of adduction, dorsiflexion and supination | ||
| Big toe: More loss of extension than flexion | ||
| Toes: More loss of flexion than extension | ||






























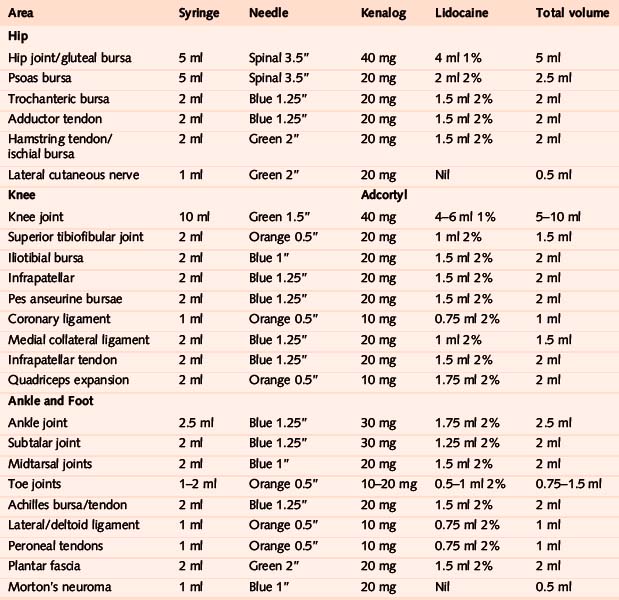
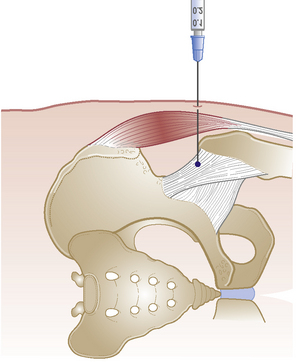
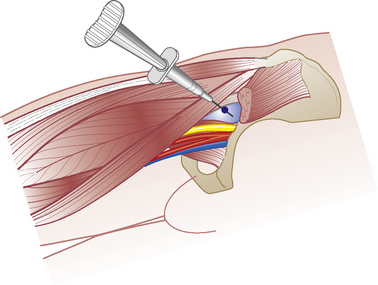
Hip joint
Acute or chronic capsulitis
Causes and findings

Technique



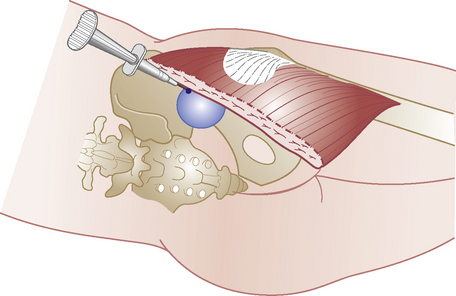
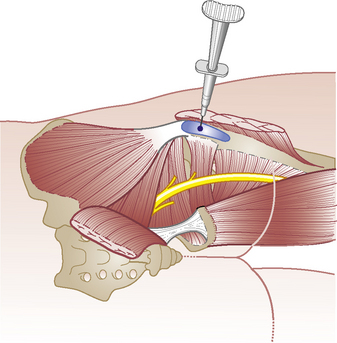
Psoas bursa
Chronic bursitis

Technique
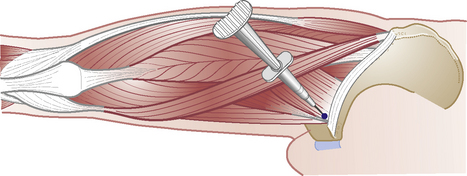
Trochanteric bursa


Adductor tendons


Hamstring tendon and ischial bursa

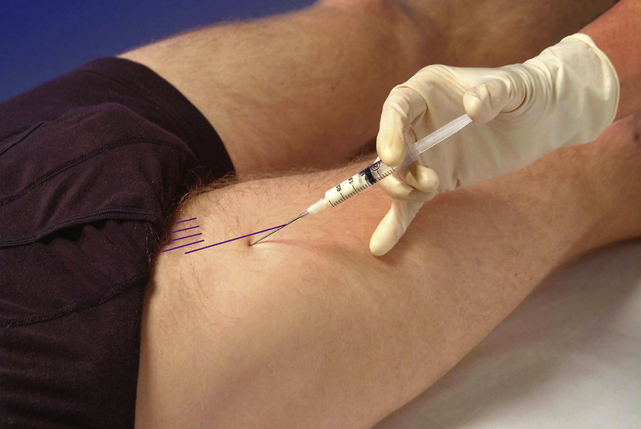
Lateral cutaneous nerve


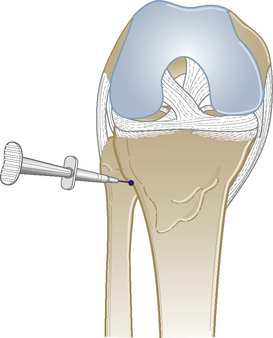
Knee joint
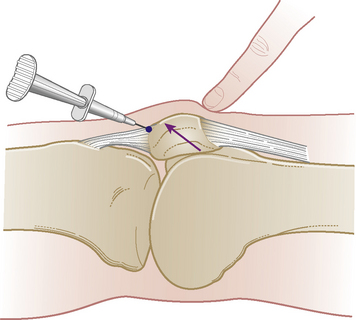
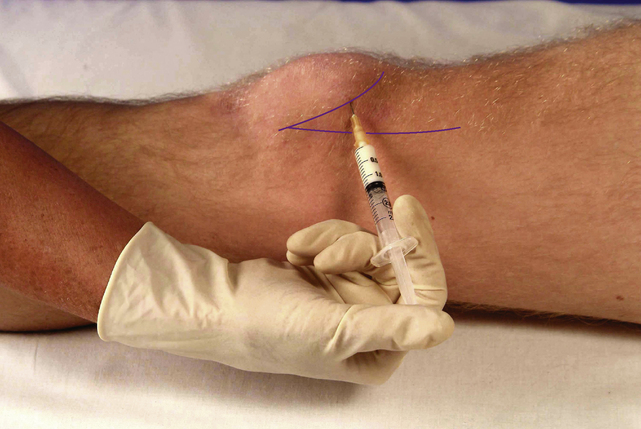
Acute or chronic capsulitis

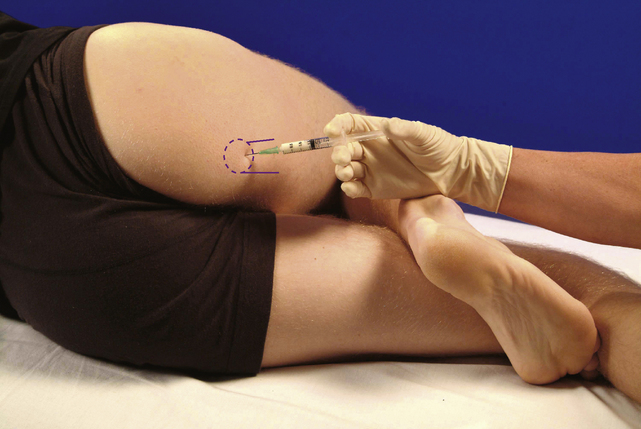
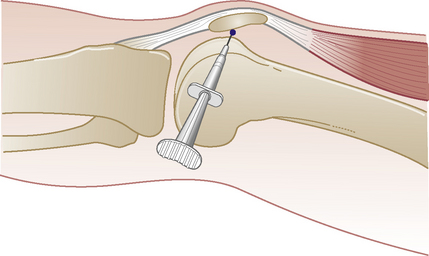
Alternative approaches
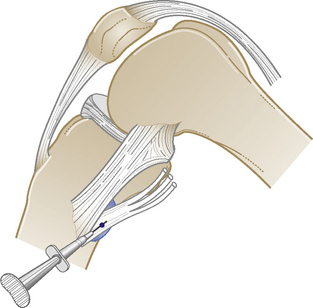
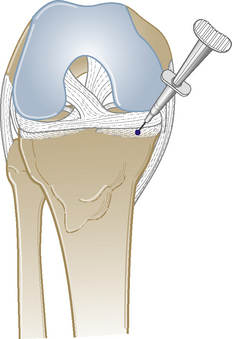
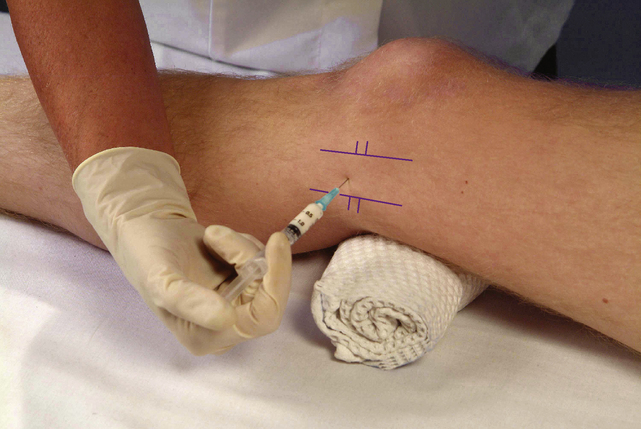
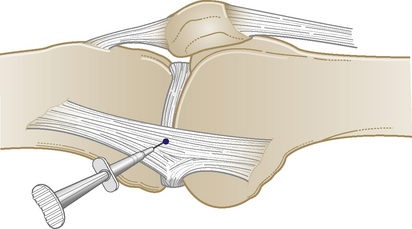
There are several ways to infiltrate or aspirate the knee joint – through the ‘eyes of the knee’, the supralateral approach into the suprapatella pouch just above the lateral pole of the patella, laterally at mid-point of patella or the medial approach as shown here42. One study showed that there was more successful intra-articular placement using the lateral patella approach than through the ‘eyes of the knee’, but did not compare the lateral with this medial approach. The advantage of this approach is that there is normally plenty of space to insert the needle between the medial condyle and the patella, where even small amounts of effusion can be aspirated. The same approach can be used whether infiltrating or aspirating serous fluid or blood. Using the larger volume of 40 mg of Adcortyl, giving 4 ml of volume, enables more of the joint surface to be bathed. Hyalgen or similar substances can also be injected here but are more expensive than corticosteroids and do not appear to have longer-lasting benefits (page 33).

Superior tibiofibular joint






Infrapatellar bursa


Pes anseurine bursa


Coronary ligaments


Medial collateral ligament

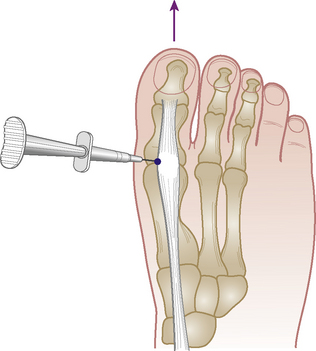
Infrapatellar tendon



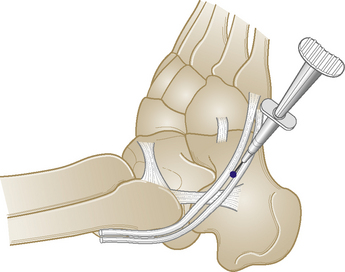
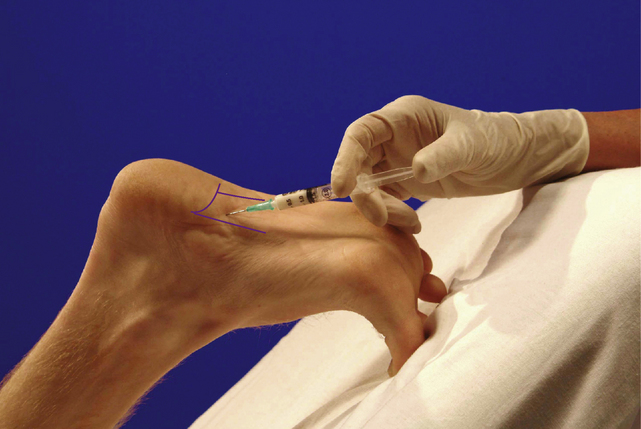
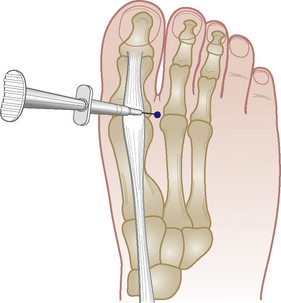
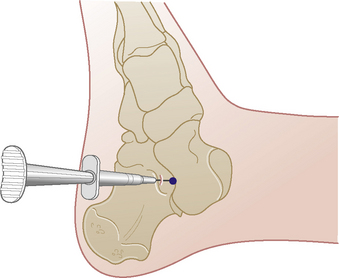
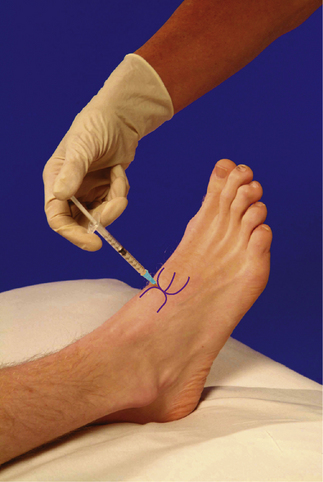
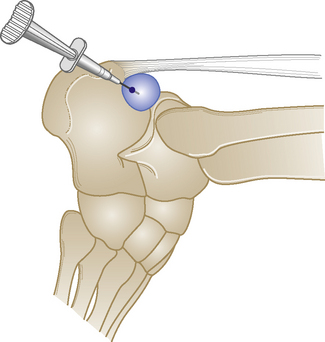
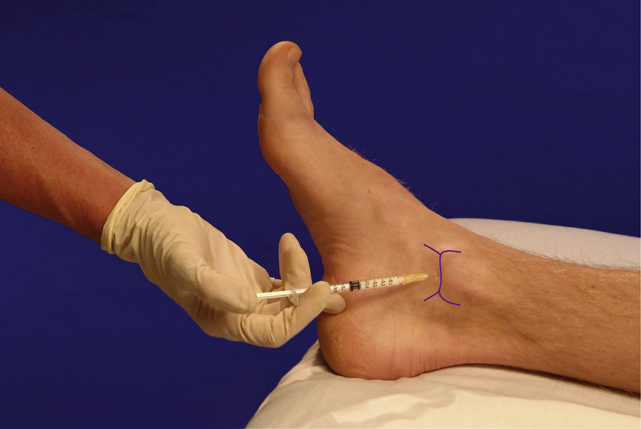
Ankle joint


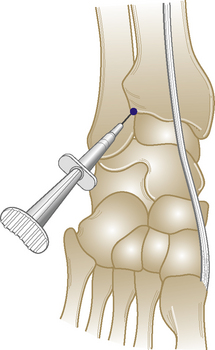
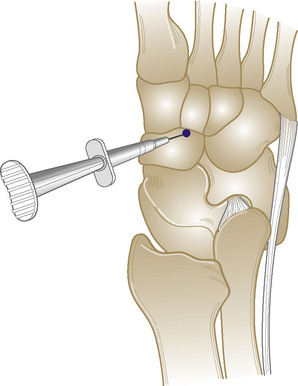
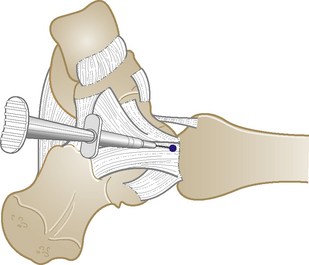
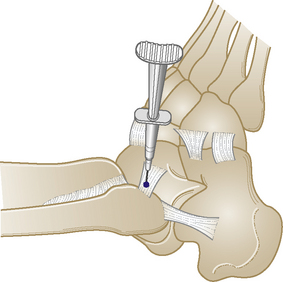
Subtalar joint







Deltoid ligament

Lateral ligament


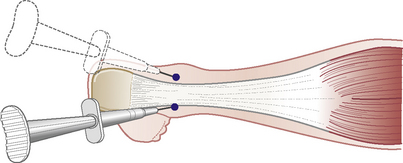
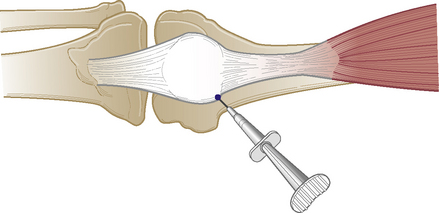
Achilles tendon
Chronic tendinopathy

Technique
Comments
Although there are reports of tendon rupture after injection here, this has usually occurred as a result of repeated injections of large dose and volume into the body of a degenerate tendon and with excessive exercise postinjection. Because of this recognized risk therefore, we recommend always scanning the tendon prior to injecting to ascertain the extent of the degeneration (page 18). Degenerative changes within the substance of the tendon, rather than just around the periphery, would indicate an absolute contraindication to injection.
Alternative approaches
No one method has been entirely successful in treating this condition. Recent novel approaches include the continuous application of topical glyceryl trinitrate, injection of a sclerosing local anaesthetic or autologous blood preparation (page 34).