CHAPTER TWELVE LOWER LEG, ANKLE, AND FOOT
INTRODUCTION
ORTHOPEDIC GAMUT 12-1 IMPORTANT SHOE DESIGN FEATURES
The restrictive force of poorly fitting shoes produces little deformity on the tarsus because the tarsus is made up of short, heavy bones. Normal movement in the tarsal joints is limited because the articular surfaces of the tarsal joints are flat. However, the phalanges and metatarsals are long thin bones with a normally wide range of joint motion. Restrictive force on these bones produces most of the static deformities of the forefoot. These static deformities include first metatarsophalangeal joint deformities, hammertoe, tailor’s bunion, overlapping toes, and many other conditions that are deviations from the normal (Table 12-3).
| Articular |
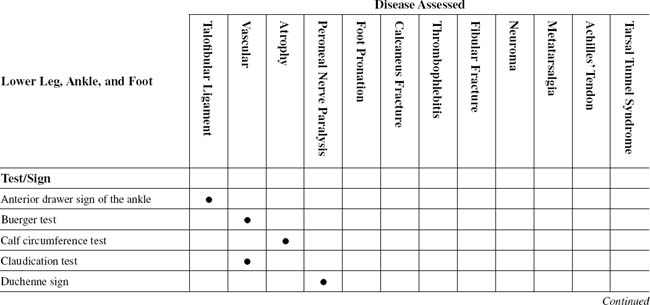
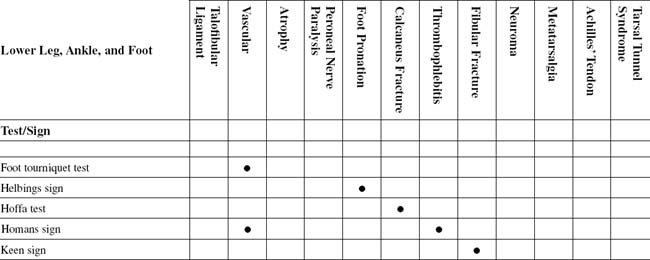
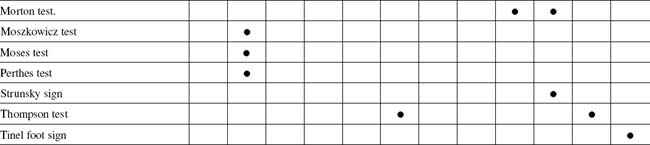
TABLE 12-2 LOWER LEG, ANKLE, AND FOOT CROSS-REFERENCE TABLE BY SYNDROME OR TISSUE
| Achilles tendon | Thompson test |
| Atrophy | Calf circumference test |
| Calcaneus fracture | |
| Fibular fracture | Keen sign |
| Foot pronation | Helbings sign |
| Metatarsalgia | |
| Neuroma | Morton test |
| Peroneal nerve paralysis | Duchenne sign |
| Talofibular ligament | Anterior drawer sign of the ankle |
| Tarsal tunnel syndrome | Tinel foot sign |
| Thrombophlebitis | |
| Vascular |
The human foot is uniquely specialized. The metatarsals and toes enable the body to stand erect. The versatility of the forefoot permits the human to retain an upright stance and allows for grace during walking, dancing, and athletics.
ESSENTIAL ANATOMY
The anterior leg muscles attach to the area between the tibia and fibula.
ESSENTIAL MOTION ASSESSMENT
ORTHOPEDIC GAMUT 12-5 ANKLE AND FOOT
Activities for testing range of motion of the ankle and foot:
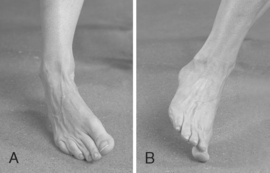
Movements of the lesser toes can be measured in a similar manner. Clinically, the examiner should note whether fixed contractures exist or if the joints are supple. Restriction of joint motion can be the result of soft-tissue contractures, bony abutment, or intraarticular adhesions. Motion may be restricted because of pain that results from inflammation or injuries (Figs. 12-1 and 12-2).

ESSENTIAL MUSCLE FUNCTION ASSESSMENT
The motions in the ankle joint are plantar flexion and dorsiflexion. The muscles in the posterior compartment, which are innervated by the tibial nerve, are responsible primarily for plantar flexion motion. The major muscles for plantar flexion are the gastrocnemius and soleus, and they are supplemented by the tibialis posterior, peroneus longus, flexor digitorum longus, and hallucis longus. The power of the gastrocnemius-soleus group is weakened when the knee is in flexion because the gastrocnemius is a two-joint muscle. However, while the knee is in flexion, the passive range of ankle dorsiflexion increases slightly. The muscles of the anterior compartment, innervated by the deep peroneal nerve, are responsible primarily for dorsiflexion motion. Dorsiflexion is performed by the tibialis anterior and the extensor digitorum longus. When these two muscles act together, their individual actions of inversion and eversion are neutralized. The extensor hallucis longus and peroneus tertius also aid in dorsiflexion (Figs. 12-3 to 12-6).




ANTERIOR DRAWER SIGN OF THE ANKLE
Assessment for Anterior Talofibular Ligament Sprain
ORTHOPEDIC GAMUT 12-7 ANKLE SPRAINS CLASSIFICATIONS
PROCEDURE

PROCEDURE

CALF CIRCUMFERENCE TEST
PROCEDURE

PROCEDURE

PROCEDURE


FOOT TOURNIQUET TEST
PROCEDURE

PROCEDURE

PROCEDURE

PROCEDURE

KEEN SIGN
Assessment for Distal Fibular Fracture
ORTHOPEDIC GAMUT 12-15 DISTAL TIBIAL AND FIBULAR FRACTURES
Types of distal tibial or fibular fractures include the following:
PROCEDURE

MORTON TEST
Assessment for Metatarsalgia or Morton Neuroma
Comment
Metatarsalgia, pain in the metatarsals, is very common in adults. This pain is caused by various foot deformities or arthritis of the metatarsophalangeal joints. This latter type of pain is most commonly caused by rheumatoid arthritis. The term metatarsalgia is used to refer to a pain syndrome and is not disease nomenclature per se (Table 12-4).
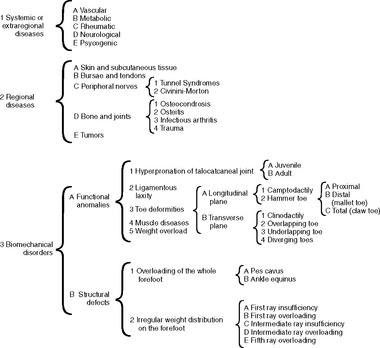 |
From Bardelli M, Turelli L, Scoccianti G: Definition and classification of metatarsalgia, Foot Ankle Surg 9(2):79-85, 2003.