[level-membership-for-plastic-reconstructive-surgery-category]
Chapter 20 Lipomyosculpture
• Morphological and histological analysis demonstrates differences in the superficial layer, regarding the layout of lobes, the shape disposition of interlobular septa tissue (collagen), and thickness of the different body parts.
• Marking before surgery is considered a key step for successful surgery. This should always be performed with the patient standing in front of the mirror. This ensures three-dimensional mobility and the patient can monitor all the surgeon’s movements and tracings.
• Ultrasonic energy (UAL) and vibroliposuction (VL) are useful as aids to conventional liposuction, but not for skin retraction.
• Liposuction must respect the histological peculiarities of the superficial layer of fat in order to stimulate skin retraction, and follow the muscle fibers’ direction; this makes it possible to carve the fat on the muscle, avoiding criss crossing.
Morpho-Histology of Subcutaneous Adipose Tissue
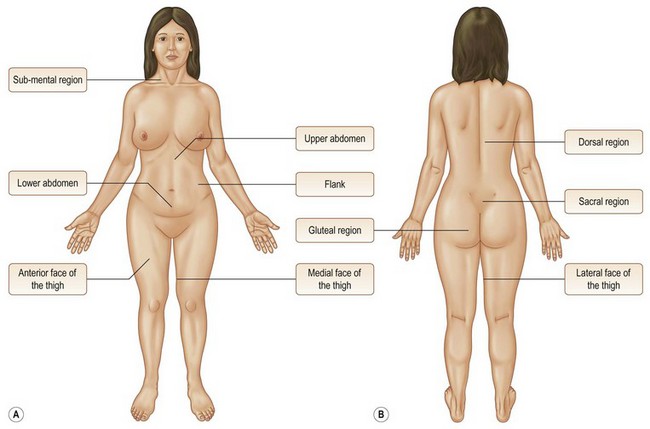
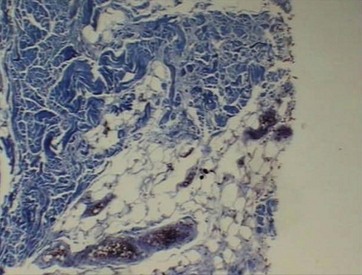
The subcutaneous tissue is divided into two layers. Its morphological and histological analysis demonstrates differences in the superficial layer, regarding the layout of lobes, shape, disposition of interlobular septa tissue (collagen), and thickness of different body parts (Fig. 20.1).
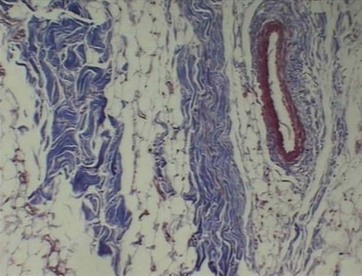
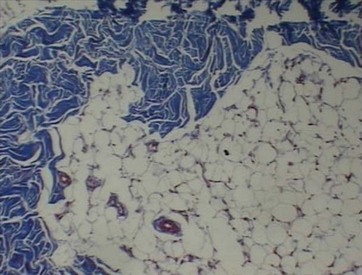
• Upper abdomen: irregular (50%), elliptical (40%) and rounded (10%) lobes with a parallel arrangement to the epidermis, thick (50%) and thin (50%) septa with a parallel arrangement in relation to the lobes (Fig. 20.2).
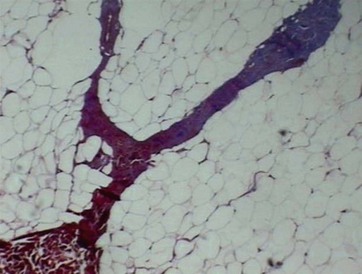
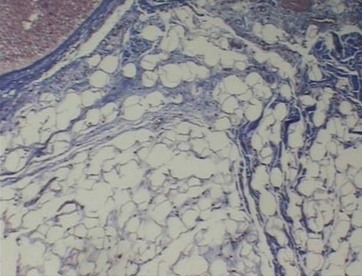
• Lower abdomen: irregular (50%), elliptical (30%) and rounded (20%) lobes with a parallel arrangement to the epidermis, thick (70%) and thin (30%) septa with a parallel arrangement in relation to the lobes (Fig. 20.3).
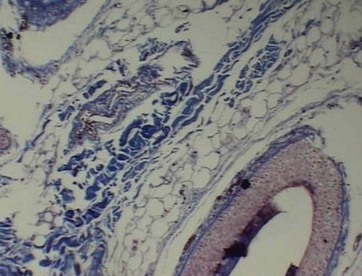
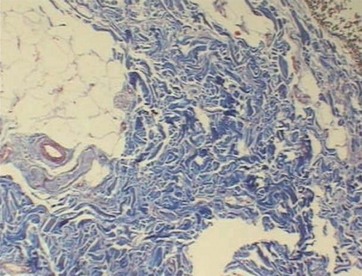
• Lateral thigh: irregular (80%), elliptical (10%) and rounded (10%) lobes with a parallel arrangement to the epidermis, thick (70%) and thin (30%) septa surrounding the lobes (Fig. 20.4).
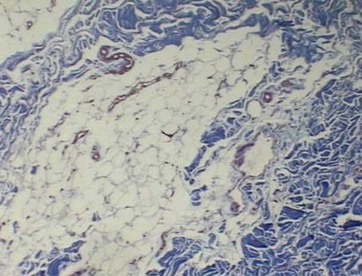
• Anterior thigh: irregular (60%), elliptical (30%) and rounded (10%) lobes with a parallel arrangement to the epidermis, thick (50%) and thin (50%) septa surrounding and penetrating the lobes (Fig. 20.5).
• Medial thigh: irregular (90%) and elliptical (10%) lobes with a parallel and perpendicular arrangement to the epidermis, thick (30%) and thin (70%) septa surrounding and perforating the lobes (Fig. 20.6).
• Dorsal region: irregular (80%), elliptical (10%) and rounded (10%) lobes with a parallel arrangement to the epidermis, thick (80%) and thin (20%) septa (Fig. 20.7).
• Flank: irregular (70%), elliptical (20%) and rounded (10%) lobes with a perpendicular arrangement to the epidermis, thick (50%) and thin (50%) septa surrounding and perforating the lobes (Fig. 20.8).
• Gluteal region: irregular (80%), elliptical (10%) and rounded (10%) lobes with a parallel arrangement to the epidermis, thick (90%) and thin (10%) septa surrounding and perforating the lobes (Fig. 20.9).
• Sacral promontory: irregular (80%), elliptical (10%) and rounded (10%) lobes with a parallel arrangement to the epidermis, thick (90%) and thin (10%) septa perpendicular to the lobes (Fig. 20.10).
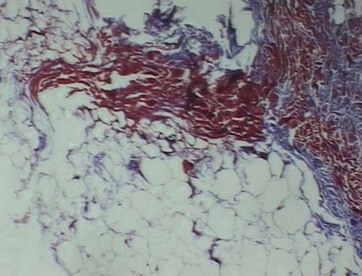
FIG. 20.10 Sacral promontory: thick and perforating septa tissue, elliptical lobe of adipose tissue.
• Submental region: irregular (90%) and elliptical (10%) lobes with a perpendicular arrangement to the epidermis, thick (40%) and thin (60%) septa surrounding the lobes (Fig. 20.11).
 ONLINE ONLY
ONLINE ONLY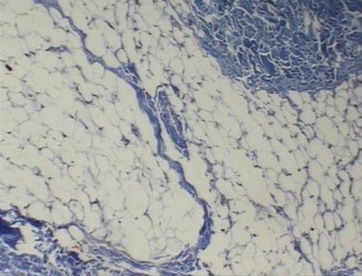
Surgical Technique
Marking
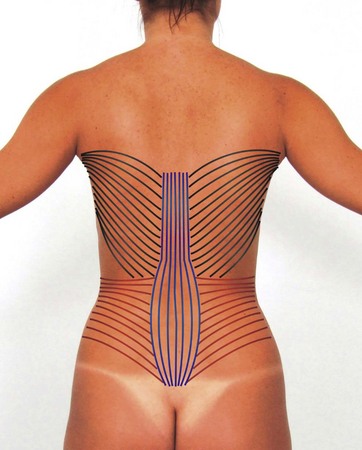
Marking before surgery is considered a key step for successful surgery. Marking is always performed with the patient standing, without the administration of preanesthetic and in front of the mirror. While ensuring three-dimensional mobility, the patient can monitor all the surgeon’s movements and tracings, and is able to give his/her opinion and indicate the areas that bother most and that may go unnoticed. Thus, patient and surgeon can match expectations and actual surgical possibilities. After defining the areas to be sucked, the direction of the muscle fibers is drawn to help in following the technique of lipomyosculpture (Figs 20.12–20.14).


Conclusion
Through this technique we can also minimize some common complications in conventional liposuction, such as intraoperative bleeding and muscle damage. This happens because the location of the subcutaneous neurovascular bundle follows the same direction as the muscle fibers, so there is less chance of bleeding (Fig. 20.15). Muscular trauma and its consequences are diminished when fibers are divided, instead of breaking them incidentally with the cannula.

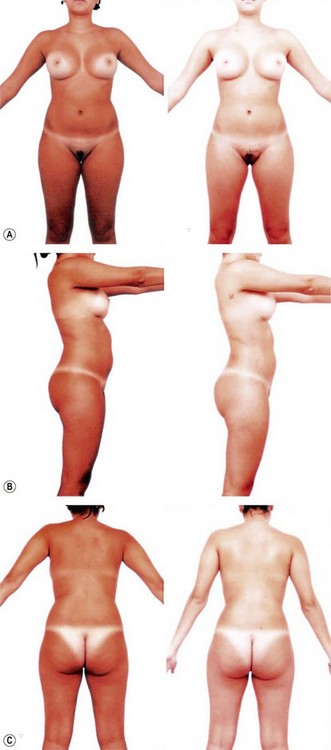
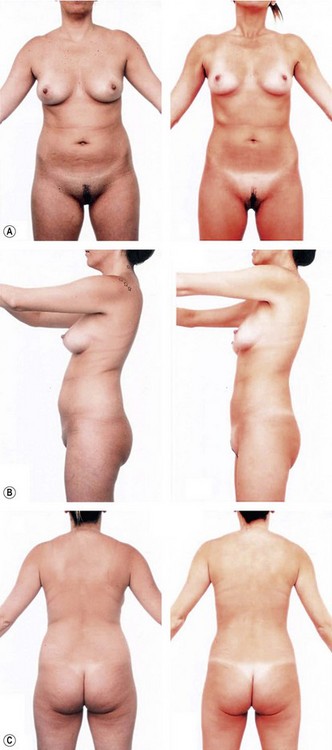
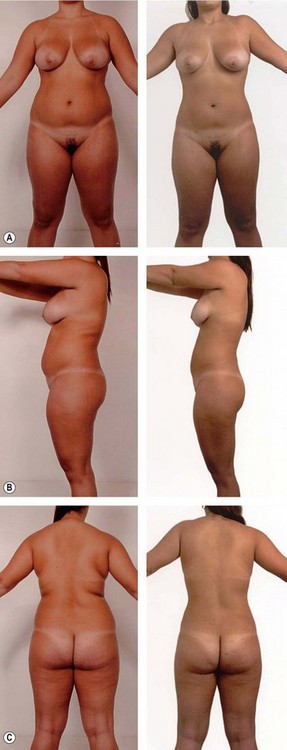
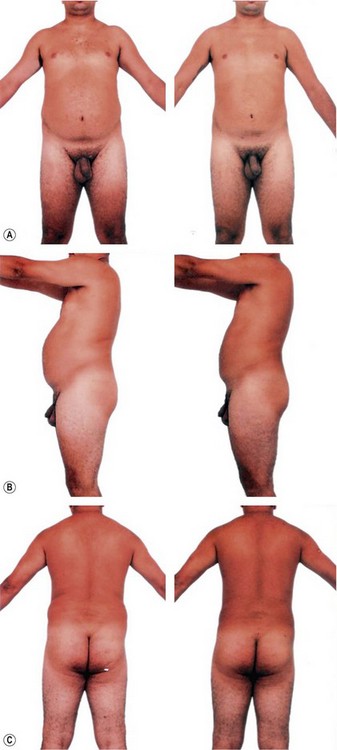
The technique achieves both layers, superficial and deep subcutaneous tissue, in order to obtain a good skin retraction and a smooth removal of fat tissue. This requires a careful surgical sequence to obtain the desired results. See case studies shown in Figs 20.16–20.21.



 Bonus images for this chapter can be found online at http://www.expertconsult.com
Bonus images for this chapter can be found online at http://www.expertconsult.comda Rocha RP. Atlas de cirurgia estética para o residente. Revinter Ltda. 2005;1:29.
Ferner H, Staubes J, Sobotta J. – Atlas de anatomia humana, 18th ed. Editora: Guanabara Koogan SA; 1984.
Souza Pinto EB. Nossa experiência em lipoaspiração. Brasília/Brazil: Anais do Congresso Brasileiro de Cirurgia Plástica; 1983.
Souza Pinto EB. Lipoaspiração superficial. Revinter: Rio de Janeiro; 1999.
Souza Pinto EB. Morphohistologic analysis of fat tissue in áreas treated with lipoplasty. Aesth Plast Surg J. 2002:513–518.
Souza Pinto EB, Federico R, Pessoa de Melo SP, et al. Lipomioplasty with Vaser: A new approach to body contouring. Innovations in Plastic and Aesthetic Surgery. 2008;54:433–442.
[/level-membership-for-plastic-reconstructive-surgery-category][not-level-membership-for-plastic-reconstructive-surgery-category]
Chapter 20 Lipomyosculpture
• Morphological and histological analysis demonstrates differences in the superficial layer, regarding the layout of lobes, the shape disposition of interlobular septa tissue (collagen), and thickness of the different body parts.
• Marking before surgery is considered a key step for successful surgery. This should always be performed with the patient standing in front of the mirror. This ensures three-dimensional mobility and the patient can monitor all the surgeon’s movements and tracings.
• Ultrasonic energy (UAL) and vibroliposuction (VL) are useful as aids to conventional liposuction, but not for skin retraction.
• Liposuction must respect the histological peculiarities of the superficial layer of fat in order to stimulate skin retraction, and follow the muscle fibers’ direction; this makes it possible to carve the fat on the muscle, avoiding criss crossing.
Morpho-Histology of Subcutaneous Adipose Tissue
The subcutaneous tissue is divided into two layers. Its morphological and histological analysis demonstrates differences in the superficial layer, regarding the layout of lobes, shape, disposition of interlobular septa tissue (collagen), and thickness of different body parts (Fig. 20.1).
• Upper abdomen: irregular (50%), elliptical (40%) and rounded (10%) lobes with a parallel arrangement to the epidermis, thick (50%) and thin (50%) septa with a parallel arrangement in relation to the lobes (Fig. 20.2).
• Lower abdomen: irregular (50%), elliptical (30%) and rounded (20%) lobes with a parallel arrangement to the epidermis, thick (70%) and thin (30%) septa with a parallel arrangement in relation to the lobes (Fig. 20.3).
• Lateral thigh: irregular (80%), elliptical (10%) and rounded (10%) lobes with a parallel arrangement to the epidermis, thick (70%) and thin (30%) septa surrounding the lobes (Fig. 20.4).
• Anterior thigh: irregular (60%), elliptical (30%) and rounded (10%) lobes with a parallel arrangement to the epidermis, thick (50%) and thin (50%) septa surrounding and penetrating the lobes (Fig. 20.5).
• Medial thigh: irregular (90%) and elliptical (10%) lobes with a parallel and perpendicular arrangement to the epidermis, thick (30%) and thin (70%) septa surrounding and perforating the lobes (Fig. 20.6).
• Dorsal region: irregular (80%), elliptical (10%) and rounded (10%) lobes with a parallel arrangement to the epidermis, thick (80%) and thin (20%) septa (Fig. 20.7).
• Flank: irregular (70%), elliptical (20%) and rounded (10%) lobes with a perpendicular arrangement to the epidermis, thick (50%) and thin (50%) septa surrounding and perforating the lobes (Fig. 20.8).
• Gluteal region: irregular (80%), elliptical (10%) and rounded (10%) lobes with a parallel arrangement to the epidermis, thick (90%) and thin (10%) septa surrounding and perforating the lobes (Fig. 20.9).
[/not-level-membership-for-plastic-reconstructive-surgery-category]
