[level-membership-for-neurology-category]
Limbs
motor
Examination of motor function is divided into:





Tone
This is usually assessed at the wrist, elbow, hip and knee (Fig. 1). The joint is moved through its range, initially slowly and then at increasing speeds.

There are four patterns of abnormality (Table 1). Rigidity is usually easiest to find at the wrist and elbow. Spasticity is best found at the extension of the elbow or pronation and supination of the forearm, and is more marked as the joint is moved more rapidly.

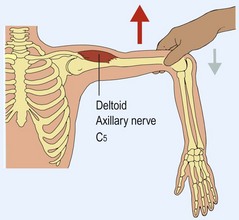
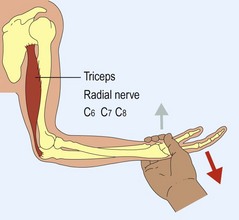
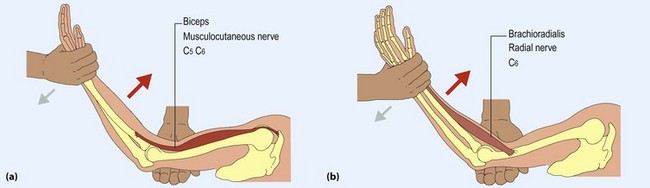
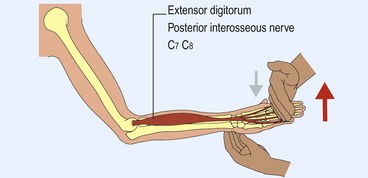
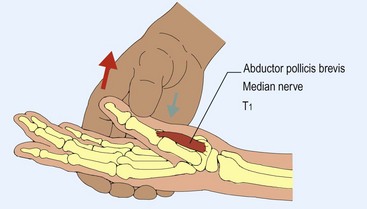
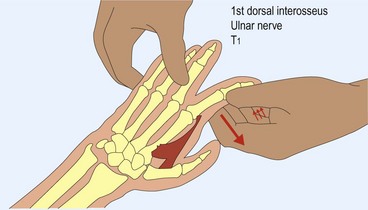
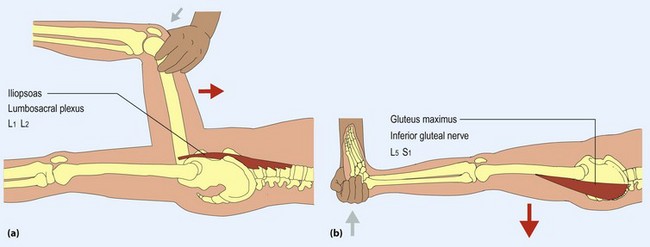
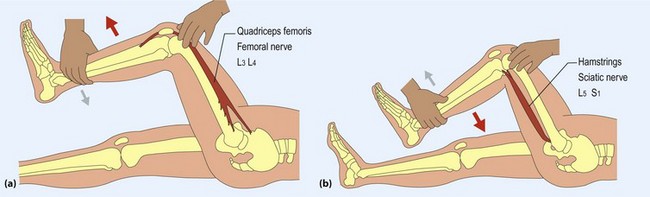
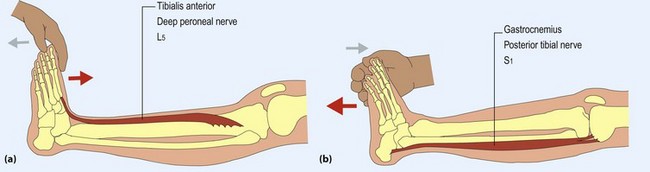
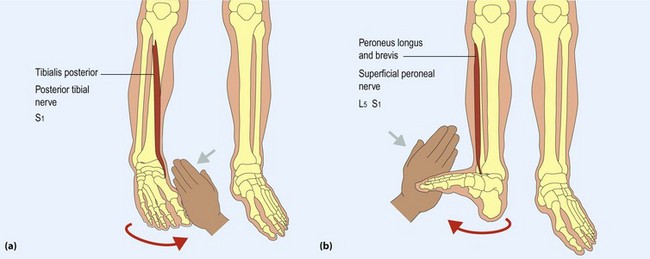
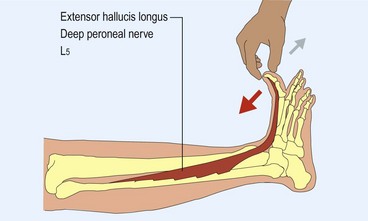
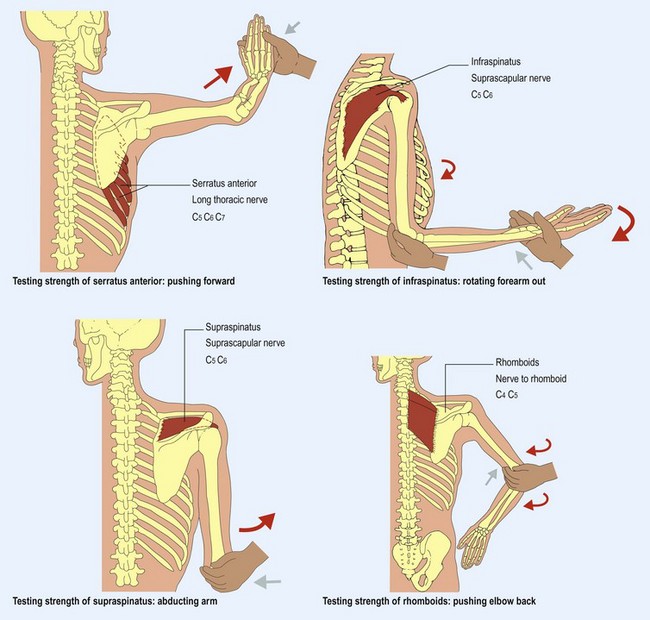
Power testing
Although traditionally called power testing, what is actually being measured, using your arms and hands as strain gauges, is force. It is important to develop a systematic approach to testing the different muscles and movements described here. As you test, try to think of the nerve root and peripheral nerve innervation of each muscle. The muscles routinely tested are shown in Figures 2–8 and 10–14 (pp. 24–25) and the less commonly tested muscles in Figure 9 (p. 24).

The amended Medical Research Council scale is used to record power and indicates the maximal power achieved, no matter how briefly (Box 1).



[/level-membership-for-neurology-category][not-level-membership-for-neurology-category]
Limbs
motor
