168
Leprosy (Hansen disease)

Anesthetic hypopigmented patches with inflamed border on the shins of borderline leprosy. From Peters W, Pasvol G. Atlas of Tropical Medicine and Parasitology, 6th edn. Mosby; 2007.

Diffuse lepromatous leprosy macules with little inflammation. From James WD, Berger T, Elston DMD, eds. Andrew’s Diseases of the Skin. 11th edn. London, Saunders; 2011.
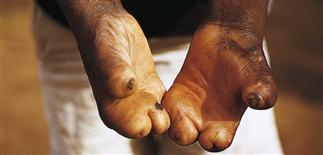
Loss of digits from chronic anesthesia, trauma, neurotrophic atrophy and eventual resorption of bone and soft tissue. From Peters W, Pasvol G. Atlas of Tropical Medicine and Parasitology, 6th edn. Mosby; 2007.

Infiltrated nodules of the forehead and face resulting in leonine facies of lepromatous leprosy. From Peters W, Pasvol G. Atlas of Tropical Medicine and Parasitology, 6th edn. Mosby; 2007.
DESCRIPTION
• A chronic infectious mycobacterial disease affected the skin and nerves, caused by Mycobacterium leprae. • It mainly affects the poor, in underdeveloped countries. It carries the most negative stigma the world has known. • There are several clinical variants, from mild to severe, which fluctuate depending on the number of mycobacteria and the host’s cell-mediated immune response. • Multidrug therapy, which includes sulfonamides, has reversed the course of the disease.
HISTORY
• This infection has been recorded though out the history of the world, from the ancient cultures of Egypt, China, India, the Middle Ages and to the present. • It affects millions worldwide, mostly the poor, who live in crowded conditions, in developing countries. • Named after Hansen in the 1870s, for his extensive clinical, epidemiological and microbiological studies of the M. leprae organism. • Many classifications, including Ridley and Jopling, based on the polarity of the disease (1966), and WHO, based on paucibacillary and multibacillary disease (1997). Treatment with systemic sufonamides changed the course of the disease.
PHYSICAL FINDINGS
• The spectrum of clinical signs and symptoms depends on the stage of the infection and host immunity. • Categorized as lepromatous, borderline-lepromatous, borderline-borderline, borderline-tuberculoid, tuberculoid. • Lepromatous leprosy: most inflammatory, multibacillary, poor cellular immune response. Macules, papules and nodules symmetrically over the cooler areas of the face, ears, wrists, elbows, knees and buttocks. Lesions may be hypopigmented and anesthetic. Leonine facies, saddle nose-deformity, madarosis and enlarged earlobes are all part of this variant. • Borderline leprosy: most common form. May have larger plaques and nodules, affects the peripheral nervous system. Unstable variant, moves toward lepromatous or tuberculoid form. • Tuberculoid leprosy: smaller, fewer patches or plaques on the trunk and extremities, which are less elevated, may be anesthetic and either hypopigmented or hyperpigmented. Neural invasions may lead to pain, muscle weakness, loss of fingers and toes as well as blindness. • Non-skin findings: enlarged peripheral nerves such as the greater auricular, ulnar, radial, common peroneal and posterior tibial. Decreased sensation to pain, temperature and touch is common.
TREATMENT
• There were no effective treatments for leprosy until dapsone, a sulfonamide, was introduced in the 1940s. • Resistance developed with monotherapy, and combination therapy emerged in the 1960s with clofazimine and rifampicin and dapsone. • Other medications, such as minocycline and ofloxacin, may be used in combinations, with the above.






